Chronic Venous Insuffiency
Chronic venous insufficiency is the impaired return of venous blood from the lower extremities due to valvular incompetence or venous obstruction, often manifesting as varicose veins, edema, skin changes, and ulceration.
Chronic Venous Insufficiency and Varicose Veins
Chronic venous disease (CVD) is the most common vascular disorder and refers to the presence of morphological (e.g., venous dilation) and/or functional (e.g., venous reflux) abnormalities of the venous system of prolonged duration [1][2].
Let's break down the key terminology, because students constantly mix these up:
- Chronic venous disease (CVD): The umbrella term — encompasses the entire spectrum from asymptomatic spider veins (C1) through to active venous ulceration (C6). Think of it as "anything wrong with the veins over time."
- Chronic venous insufficiency (CVI): A subset of CVD referring specifically to the presence of oedema, skin changes, or ulceration (i.e., CEAP C3–C6). It implies the venous system has failed to the point that tissue damage is occurring. Most commonly associated with chronic venous reflux [1][2].
- Varicose veins: Dilated, tortuous subcutaneous veins ≥ 3 mm in diameter measured in the upright position with demonstrable reflux [1][2]. The "≥ 3 mm" and "upright position" qualifiers are important — veins that are dilated when supine may be physiological.
- Telangiectasia (spider veins): Intradermal venules < 1 mm [3].
- Reticular veins: Dilated subdermal veins 1–2.9 mm, typically bluish and non-palpable [3].
Don't Confuse CVD and CVI
CVD = entire spectrum (C0–C6). CVI = only the clinically significant end (C3–C6, i.e., oedema, skin changes, or ulceration). Every patient with CVI has CVD, but not every patient with CVD has CVI.
Global and Hong Kong Context
- Prevalence: CVD is extremely common. Varicose veins affect approximately 25–30% of women and 15–20% of men in Western populations. In the Edinburgh Vein Study, trunk varices were seen in ~40% of men and ~32% of women [4].
- More common in older people [1]
- More common in females (~10× more common than males in some series) — though modern epidemiological data suggests the sex ratio is closer to 1.5–3:1 (F:M) when standardised assessment is used. The older "10×" figure likely reflects reporting/cosmetic consultation bias [1].
- More common in Europe and North America compared to Africa and Asia, though prevalence in urbanised Asian populations (including Hong Kong) is rising with lifestyle changes (sedentary jobs, obesity) [1].
- CVI (C3–C6) affects ~5% of the adult population; venous ulcers affect ~1%, with enormous healthcare cost implications.
- In Hong Kong, the ageing population and high prevalence of sedentary office work contribute to significant disease burden. Exact local prevalence data is limited but clinical experience suggests it is common in surgical outpatient clinics.
3. Anatomy and Function of the Lower Limb Venous System
Understanding the anatomy is absolutely essential — you cannot understand varicose veins or CVI without knowing how blood gets back to the heart from the legs.
The lower limb venous system is divided into three compartments, separated by the deep fascia [1][2][3]:
| System | Location | Key Veins |
|---|---|---|
| Deep veins | Below the deep fascia, within the muscular compartments | Common femoral, femoral (formerly "superficial femoral" — a misnomer!), deep femoral (profunda femoris), popliteal, anterior tibial, posterior tibial, fibular (peroneal), soleal and gastrocnemius sinuses |
| Superficial veins | Above the deep fascia, in the subcutaneous tissue | Great saphenous vein (GSV), Small (lesser/short) saphenous vein (SSV) |
| Perforator (communicating) veins | Penetrate the deep fascia, connecting superficial to deep systems | Named perforators (Hunterian, Dodd, Boyd, Cockett I/II/III, May) |
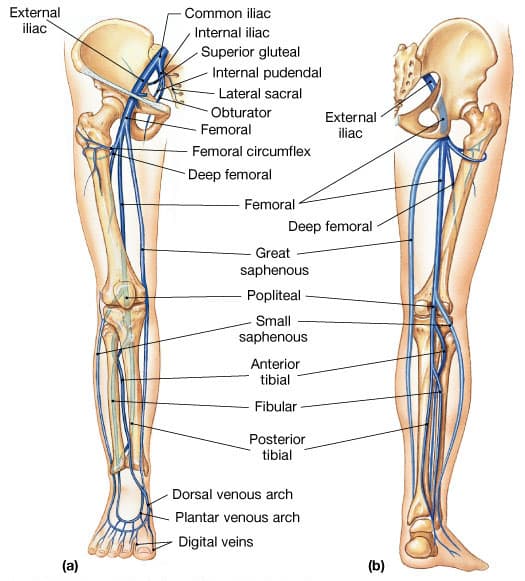
The GSV is the longest vein in the body [1][2]:
- Origin: Arises from the medial side of the dorsal venous arch of the foot
- Course: Ascends anterior to the medial malleolus → runs up the leg posterior to the medial border of the patella → ascends obliquely along the medial aspect of the thigh
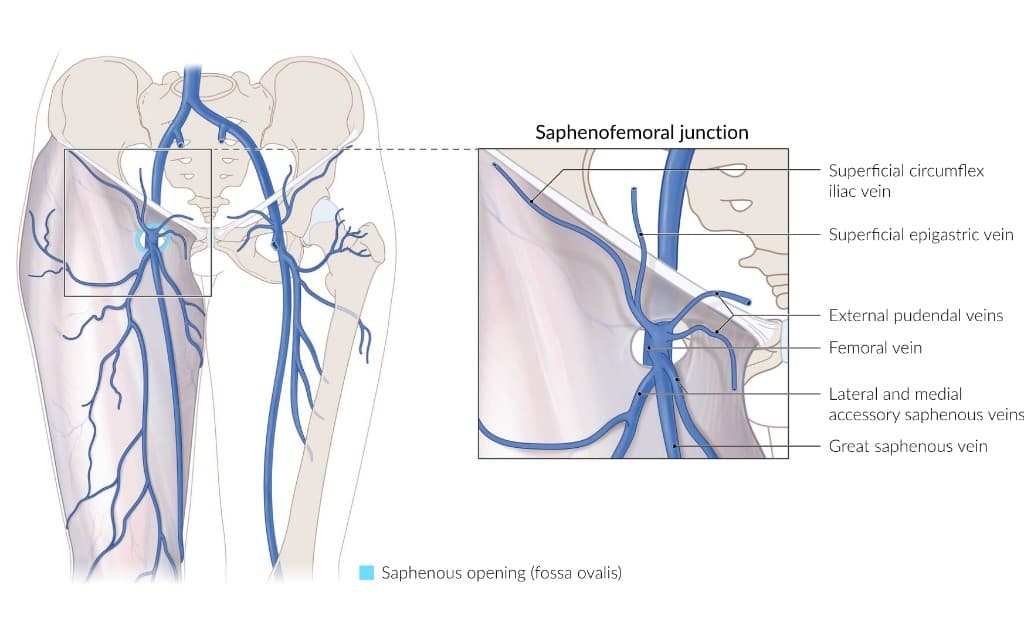
- Termination: Pierces the cribriform fascia at the saphenofemoral junction (SFJ) and drains into the common femoral vein
- SFJ is located approximately 2.5 cm lateral and inferior to the pubic tubercle [1]
- Nerve companion: The saphenous nerve accompanies the GSV, especially below the knee — this is why GSV stripping below the knee risks saphenous nerve injury (numbness along medial calf/foot)
High Yield – SFJ Location
The SFJ is 2.5 cm lateral and inferior to the pubic tubercle. This is where you'd feel a saphena varix and where the Trendelenburg operation is performed. The "Mickey Mouse sign" on duplex ultrasound shows the CFV, CFA, and GSV in cross-section at this level.
- Origin: Arises from the lateral side of the dorsal venous arch of the foot
- Course: Ascends posterior to the lateral malleolus → runs up the midline of the calf posteriorly
- Termination: Pierces the deep fascia over the popliteal fossa and drains into the popliteal vein at the saphenopopliteal junction (SPJ)
- Nerve companion: The sural nerve accompanies the SSV — SSV surgery risks sural nerve injury (numbness along posterolateral leg and lateral foot) [1][2]
These are valved veins that join the superficial to the deep veins at inconstant sites, allowing blood to flow from superficial → deep venous system [1][2]. They are critical because when their one-way valves fail, high-pressure deep venous blood refluxes into the superficial system, contributing to CVI.
Named perforators (from proximal to distal):
| Perforator | Location | Drains Into |
|---|---|---|
| Hunterian | Proximal thigh | Femoral vein |
| Dodd | Mid-thigh | Superficial femoral vein |
| Boyd | Below knee (proximal calf) | Gastrocnemius vein |
| Cockett I, II, III | Lower leg (medial aspect) | Posterior tibial vein |
| May | Ankle | Posterior tibial vein and plantar vein |
The Cockett perforators are particularly important because they are in the "gaiter area" (lower medial calf/ankle) — this is precisely where venous ulcers develop.
Why doesn't blood just pool in our legs when we stand up? Several mechanisms work together [2][3]:
-
Calf muscle pump (the "peripheral heart") — this is the major mechanism
- Contraction of calf muscles (gastrocnemius, soleus) compresses the large venous sinuses within the muscles
- This squeezes blood into the popliteal veins and propels it cephalad towards the heart
- During relaxation, the deep venous pressure drops, and blood flows from the superficial system into the deep system via the perforator veins
-
One-way bicuspid valves
- Present in all three venous systems (deep, superficial, perforator)
- Ensure unidirectional flow: deep veins → towards the heart; superficial → towards deep; perforators → superficial to deep only
- Valve closure is triggered by retrograde flow — when blood starts to fall back, the valve cusps fill and coapt
-
Respiratory pump
- Decreased intrathoracic pressure during inspiration creates a pressure gradient that sucks blood from the abdomen and lower limbs into the thorax
-
Vis a tergo (force from behind) — residual arterial pressure transmitted through capillary beds
-
Venous tone — smooth muscle in venous walls maintains basal tone under sympathetic control
Key Concept – The Calf Muscle Pump
Think of it as a "second heart." When you walk, your calf muscles squeeze blood upward through the deep veins. During relaxation, the deep venous pressure drops below the superficial venous pressure, allowing blood to flow inward through perforators. Valves prevent backflow. When any part of this system fails (valves, muscles, or venous patency), venous hypertension develops.
4. Etiology and Risk Factors
The risk factors make intuitive sense once you understand the physiology — anything that increases venous pressure, damages valves, or impairs the calf pump [1][2][3]:
| Risk Factor | Mechanism |
|---|---|
| Female sex | Oestrogen/progesterone cause venous wall relaxation and valve dysfunction; pregnancy; higher collagen laxity |
| Increasing age | Progressive loss of venous wall elastin and collagen, cumulative valve damage |
| Obesity | Increased abdominal pressure → impedes venous return; chronic inflammation; reduced physical activity |
| Family history | Genetic predisposition to weak venous wall/valve structure (collagen subtypes, MMPs) |
| Prolonged standing (occupational) | Sustained hydrostatic pressure column without calf pump activation (teachers, surgeons, hairdressers) |
| Pregnancy | ① Increased blood volume, ② Hormonal venous wall relaxation, ③ Uterine compression of IVC/iliac veins, ④ Increased abdominal pressure |
| Previous DVT | Valve destruction by thrombotic/inflammatory process (post-thrombotic syndrome) |
| Chronic cough / constipation | Increased abdominal pressure → impedes venous return |
| Sedentary lifestyle | Reduced calf muscle pump activity |
| Smoking | Endothelial damage, chronic inflammation |
| Previous superficial thrombophlebitis | Direct valve damage |
| Trauma | Direct venous/valve damage |
4.2 Causes — Primary vs. Secondary
This simple bedside framework is still useful, but if you want the formal 2020 CEAP etiologic classification, think:
- Ec = congenital
- Ep = primary
- Esi = secondary, intravenous (inside the vein; wall/valve damage)
- Ese = secondary, extravenous (outside the vein or systemic hemodynamic / calf-pump problem)
- En = no venous cause identified
- Idiopathic — most common
- Intrinsic abnormalities in the venous wall:
- Dysfunctional smooth muscle cell proliferation
- Abnormal collagen deposition
- Decreased elastin content
- Increased matrix metalloproteinase (MMP) activity — MMPs degrade the extracellular matrix of the venous wall, weakening it [1]
- The vein wall weakens → dilates → the valve leaflets can no longer coapt → reflux → further dilation → a vicious cycle
The 2020 CEAP update recommends splitting secondary disease into intravenous vs. extravenous causes, because these can produce similar clinical findings but require different management [1][2][3]:
| CEAP Etiologic Group | Mechanism | Causes | Explanation |
|---|---|---|---|
| Esi | Intravenous wall / valve damage or intraluminal pathology | DVT (accounts for most secondary cases) — post-thrombotic syndrome; superficial thrombophlebitis; arterio-venous (AV) fistula (congenital or acquired) | Thrombus organisation and recanalisation damages valve leaflets → permanent reflux. This is the most important secondary cause [1]. AV fistula causes pathological high-flow venous hypertension from within the circulation |
| Ese | Extravenous obstruction or altered venous hemodynamics | Pregnancy; external compression (ovarian cysts, fibroids, pelvic cancers — CA cervix/uterus/ovary/rectum); May-Thurner syndrome; stroke, musculoskeletal weakness, paralysis, prolonged immobility | If outflow is blocked, pressure builds up distally. May-Thurner = left common iliac vein compressed by right common iliac artery against lumbar vertebra — important cause of left-sided DVT/CVI in young women. Without a functioning calf muscle pump, venous return depends on gravity and the respiratory pump alone — totally inadequate |
-
Klippel-Trénaunay syndrome: Congenital venous malformation causing a triad of:
- Varicose veins (classically over lateral aspect of thigh — i.e., NOT in typical GSV/SSV distribution)
- Port wine stains (capillary malformation)
- Bony and soft tissue hypertrophy of the affected limb
-
Parkes-Weber syndrome: Multiple congenital AV fistulae with limb hypertrophy, potentially causing high-output heart failure (because the fistulae shunt blood from the arterial to the venous system, increasing preload)
May-Thurner Syndrome
If a young woman presents with left leg swelling and varicose veins, think May-Thurner: the left common iliac vein is compressed between the right common iliac artery and the lumbar spine. It predisposes to left ilio-femoral DVT and chronic venous insufficiency. This is a favourite exam question.
5. Pathophysiology
The core pathophysiology of both varicose veins and CVI is venous hypertension [2][3].
Normal ambulatory venous pressure in the foot is ~20–25 mmHg (because the calf muscle pump effectively empties the veins during walking). In CVI, ambulatory venous pressure rises to 60–90 mmHg.
Here is the pathophysiological cascade:
-
Reflux (>80% of cases) [1]: When valves are incompetent, blood refluxes during relaxation of the calf pump. In the standing position, this creates a continuous column of hydrostatic pressure from the heart to the ankle, with no effective "breaks."
-
White cell trapping hypothesis (Coleridge-Smith): Venous hypertension causes leucocytes to marginate, adhere to capillary endothelium, become activated, and release inflammatory mediators (proteolytic enzymes, free radicals) → endothelial damage and tissue destruction.
-
Fibrin cuff hypothesis (Browse and Burnand): Fibrinogen leaks through distended capillaries, polymerises into pericapillary fibrin cuffs → acts as a physical barrier to O₂ and nutrient diffusion → tissue ischaemia.
-
Growth factor trapping hypothesis (Falanga and Eaglstein): Macromolecules that leak into the interstitium bind and "trap" growth factors essential for tissue repair, impeding wound healing.
In practice, all three mechanisms likely operate simultaneously.
Venous ulcers classically occur at the medial gaiter area (the zone between the lower calf and medial malleolus). Why?
- This is the site of the medial calf perforators (Cockett perforators), which connect the posterior tibial vein to the GSV tributaries
- When these perforator valves fail, high-pressure deep venous blood is transmitted directly to the superficial subcutaneous tissues in this area
- The skin here is thin and poorly vascularised to begin with, making it particularly vulnerable to venous hypertension-mediated injury [3]
6. Classification — CEAP
The CEAP classification is the internationally accepted classification system for chronic venous disease. It stands for Clinical-Etiological-Anatomical-Pathophysiological [1][2][3].
| Class | Description | Key Details / Pathophysiology |
|---|---|---|
| C0 | No visible or palpable signs of venous disease | Patient may still be symptomatic (e.g., heaviness, aching) |
| C1 | Telangiectasia (< 1 mm) or reticular veins (1–2.9 mm) | Intradermal venules; "spider veins." |
| C2 | Varicose veins (≥ 3 mm) | Dilated, tortuous subcutaneous veins with demonstrable reflux |
| C3 | Oedema without skin changes | Pitting oedema from increased capillary permeability and interstitial fluid accumulation due to venous hypertension |
| C4a | Pigmentation and/or eczema | Pigmentation: Haemosiderin deposition from extravasated RBCs broken down by macrophages. Eczema (venous stasis dermatitis): Inflammatory response to leaked plasma proteins; itchy, erythematous, sometimes weeping |
| C4b | Lipodermatosclerosis (LDS) and/or atrophie blanche | LDS: Progressive fibrosis of skin and subcutaneous tissue due to chronic inflammation and fibrin deposition. Clinically: hyperpigmentation + erythema + induration + tenderness (palpate!). Gives the classic "inverted champagne bottle" appearance. Atrophie blanche: Avascular fibrotic scars — ivory-white areas with hyperpigmented borders. Prone to secondary ulceration due to poor blood supply [3] |
| C4c | Corona phlebectatica | Fan-shaped intradermal veins at the ankle/foot (malleolar flare), typically below or around the malleoli. In the 2020 CEAP update this became its own C4 subclass, reflecting that it is an early sign of advanced chronic venous disease rather than simple C1 telangiectasia [3] |
| C5 | Healed venous ulceration with skin changes as above | Evidence of prior tissue breakdown. At medial gaiter area. Long-standing ulcer → Marjolin's ulcer (2%) — malignant transformation, usually to SCC [3] |
| C6 | Active venous ulceration | Full-thickness skin loss. Usually painless unless infected (commonly S. aureus) [3]. Located at medial gaiter area |
Each C class is further subscripted as S (symptomatic) or A (asymptomatic). For example, C2S = symptomatic varicose veins.
| Code | Meaning |
|---|---|
| Ec | Congenital |
| Ep | Primary (most common — degenerative, idiopathic) |
| Esi | Secondary, intravenous cause (e.g., post-thrombotic valve / wall damage) |
| Ese | Secondary, extravenous cause (e.g., extrinsic compression, systemic venous hypertension, calf-pump failure) |
| En | No venous cause identified |
| Code | Meaning |
|---|---|
| As | Superficial veins |
| Ap | Perforator veins |
| Ad | Deep veins |
| An | No venous location identified |
| Code | Meaning |
|---|---|
| Pr | Reflux |
| Po | Obstruction |
| Pr,o | Reflux + Obstruction |
| Pn | No venous pathophysiology identified |
Example: A patient with symptomatic varicose veins from primary GSV reflux would be classified as: C2S, Ep, As, Pr
Another common example: post-thrombotic CVI with deep venous reflux would fall under Esi, not the older undifferentiated Es bucket.
CEAP is High Yield
Students often only memorise the C classification and forget E, A, and P. The full CEAP classification is frequently asked in summative exams. Remember: C = what you see, E = why it happened, A = where it is, P = what went wrong mechanistically.
7. Clinical Features
| Symptom | Details | Pathophysiological Basis |
|---|---|---|
| Cosmetic concern / unsightly veins | The principal complaint for many patients — visible dilated, tortuous veins. Truncal, tributary, reticular, and perforatory varicosities [1] | Venous wall weakness and valve failure → vein dilation and tortuosity |
| Pain / Aching | Dull ache, tingling, or burning, usually in the calf and lower leg. Worse with prolonged standing; relieved by lying down, leg elevation, or compression stockings [1][3] | Venous hypertension → distension of vein walls → stimulation of nociceptors. Standing worsens the hydrostatic column; elevation reduces it. Compression counteracts the distension |
| Heaviness / dragging sensation | Heavy, tired legs, especially at end of day [1][3] | Increased venous pooling → increased leg volume → sensation of heaviness |
| Ankle swelling | Usually worse at end of day, improves overnight [1] | Venous hypertension → increased capillary hydrostatic pressure → transudation of fluid into interstitium (Starling forces) |
| Night cramps | Painful involuntary muscle contractions at night [1] | Mechanism not fully understood — possibly related to electrolyte shifts from chronic oedema, or muscle metabolite accumulation from venous stasis |
| Itchiness (pruritus) | Especially around ankles [1][3] | Venous stasis dermatitis — inflammatory mediators released from trapped leucocytes and degraded blood products stimulate cutaneous nerve endings |
| Early fatigue | Legs tire easily [1] | Impaired venous return → reduced clearance of metabolic waste products from exercising muscle → early fatigue |
| Worsening pattern | Symptoms typically worsen throughout the course of the day / with standing and are relieved by lying down / leg elevation [3] | Cumulative venous pooling during the day with hydrostatic load; elevation eliminates the hydrostatic component |
7.2 Signs (with pathophysiological basis)
On examination, signs progress along the CEAP spectrum:
- Surgical scars — previous venous surgery? (recurrent varicose veins) [1][3]
- Location of varicosities — this tells you which system is incompetent [1][2][3]:
- Medial thigh and medial calf → GSV incompetence
- Posterior calf → SSV incompetence
- Anterolateral thigh and anterolateral calf → Isolated incompetence of proximal anterolateral GSV tributary
- Skin changes of CVI:
- Corona phlebectatica (malleolar flare; CEAP C4c): Fan-shaped intradermal veins on the ankle/foot, first appearing in a triangular area below the medial malleolus with the apex over the first/second lower leg communicating vein [3]. This is an early sign of advanced chronic venous disease.
- Hyperpigmentation: Brown discolouration from haemosiderin (breakdown product of extravasated RBCs). May cover the entire lower limb in severe cases [3].
- Venous stasis eczema: Erythematous, scaly, weeping skin — inflammatory response to leaked plasma proteins and haemosiderin.
- Lipodermatosclerosis (LDS): Hyperpigmentation + erythema + induration + tenderness — progressive fibrosis giving the "inverted champagne bottle" leg [3]. Acute LDS is often misdiagnosed as cellulitis or acute thrombophlebitis because it is painful, hot, red, and tender [3].
- Atrophie blanche: Ivory-white avascular scars with hyperpigmented borders — represents areas where tissue has undergone fibrosis and the microvasculature has been obliterated [3].
- Venous ulcers: At medial gaiter area (see Section 5.3 for why). Typically shallow, irregular but gently sloping edges, with slough or granulation tissue at base. Usually painless unless infected [3].
- Fixed flexion of ankle — subcutaneous fibrosis from chronic LDS and/or painful ulceration may cause contracture [3]
Acute Lipodermatosclerosis — Common Misdiagnosis
Acute LDS presents with a painful, hot, red, tender area on the medial lower leg — it looks exactly like cellulitis. The key differentiator: acute LDS occurs in the context of known CVI, is bilateral (or at least in the expected distribution), and does not respond to antibiotics. Always examine for underlying CVI when you see "cellulitis" on the lower leg.
- Palpate along the course of the GSV and SSV and their tributaries to feel for varicosities and tenderness [1][3]
- Check peripheral pulses — this is critical because:
- You need to rule out peripheral arterial disease (PAD) before applying compression therapy
- Compression on an ischaemic limb can cause tissue necrosis
- ABPI must be checked — absolute contraindication to compression if ABPI < 0.4 [3]
- Pitting oedema — increased interstitial fluid from venous hypertension; usually confined to the ankle but can extend to the foot and rest of the leg [1]
- Saphena varix — a compressible lump in the inguinal region (at the SFJ) that:
- Palpate inguinal lymph nodes — if venous ulcers are present, check for lymphadenopathy (infection, or rarely Marjolin's ulcer — malignant transformation) [3]
- Test neurological function (e.g., sural nerve) if surgical scars are present — to assess for iatrogenic nerve injury from prior surgery [3]
- Auscultate over varicosities for AV malformations — a continuous bruit suggests an arteriovenous fistula as the cause of the varicosities [1]
Tourniquet Test (Trendelenburg Test) — a bedside test to assess the level of venous incompetence [1][3]:
- Patient supine → elevate the leg to empty the superficial veins
- Apply a tourniquet to occlude the superficial veins (this blocks SFJ reflux)
- Patient stands up → observe filling of varicose veins
- If veins remain empty (fill slowly from below over > 30 seconds) → the tourniquet has controlled the point of reflux. This implies SFJ incompetence
- If veins fill rapidly from below despite the tourniquet → there is incompetence below the level of the tourniquet (perforator or other level of reflux)
- Release the tourniquet → if veins suddenly fill from above → confirms SFJ incompetence
- The test can be repeated at different levels: just below SFJ, mid-thigh, above knee, below knee to localise the level of perforator incompetence [3]
Note: In modern practice, the tourniquet test has been largely replaced by duplex ultrasound, which is far more accurate. However, it is still examined in clinical exams.
- Examine the inguinal region for mass or lymphadenopathy causing venous outflow obstruction [1]
- Abdominal and pelvic examination if secondary causes are suspected (ovarian cyst, fibroid, pelvic tumour)
- ABPI measurement — essential before planning any compression or surgical therapy
This is a classic exam comparison [3][5]:
| Feature | Venous Ulcer | Arterial Ulcer |
|---|---|---|
| Location | Medial gaiter area | Tips of toes, between digits, lateral malleolus, heel — pressure points and most distal areas |
| Depth | Shallow | Deep |
| Edge | Gently sloping | Punched-out |
| Base | Slough with granulation tissue | Unhealthy, necrotic, pale |
| Pain | Usually painless unless infected | Very painful (ischaemic pain) |
| Surrounding skin | Haemosiderin-stained, eczematous, fibrotic (LDS), oedema | Cold, thin, shiny, hairless skin |
| Pulses | Present | Absent or weak |
| Associated conditions | Varicose veins, DVT, recurrent phlebitis | DM, hypertension, PAD, smoking |
| Feature | Venous | Arterial | Neuropathic | Pressure |
|---|---|---|---|---|
| Location | Gaiter area | Toes, heel, lateral malleolus | Plantar foot, tips of toes, lateral to 5th MT | Bony prominences, heel |
| Pain | Minimal | Severe | Painless | Variable |
| Surrounding skin | Pigmented, eczematous | Cold, shiny, hairless | Dry, cracked, calluses | Atrophic, macerated |
| Pulses | Present | Absent/weak | Present | Present |
| Sensation | Normal | Normal | Diminished | Normal |
From the lecture slides on toe gangrene and leg ulcers [5]:
- Venous ulcers account for ~70% of all lower limb ulcers
- Arterial ulcers account for ~10–15%
- Mixed venous-arterial ulcers are common (~15%)
- Always check ABPI before applying compression — compression on an ischaemic limb is dangerous
From the wound healing lecture [6]:
- Chronic venous ulcers represent wounds "stuck" in the inflammatory phase of healing
- Bacterial colonisation (especially S. aureus) delays healing but does not necessarily mean clinical infection — clinical infection requires signs of surrounding cellulitis, purulent discharge, or systemic features
- Biofilms are common in chronic venous ulcers and contribute to treatment resistance
High Yield Summary
Definition: Varicose veins = dilated, tortuous subcutaneous veins ≥ 3 mm with demonstrable reflux. CVI = oedema, skin changes, or ulceration from chronic venous dysfunction (CEAP C3–C6).
Core pathophysiology: Venous valve incompetence → reflux → sustained venous hypertension → capillary distension → leakage of RBCs, fluid, proteins → haemosiderin deposition, fibrin cuffs, WBC trapping → inflammation, tissue hypoxia → skin changes, fibrosis, and ulceration.
CEAP: C0 (no signs) → C1 (telangiectasia/reticular veins) → C2 (varicose veins) → C3 (oedema) → C4a (pigmentation/eczema) → C4b (LDS/atrophie blanche) → C4c (corona phlebectatica) → C5 (healed ulcer) → C6 (active ulcer). Plus E (aetiology), A (anatomy), P (pathophysiology).
Anatomy: GSV runs medially (SFJ at groin, saphenous nerve companion). SSV runs posteriorly in calf (SPJ at popliteal fossa, sural nerve companion). Perforators (Hunterian → Dodd → Boyd → Cockett → May) connect superficial to deep.
Risk factors: Female, age, obesity, family history, prolonged standing, pregnancy, previous DVT, increased abdominal pressure.
Primary (idiopathic, intrinsic wall weakness) vs. Secondary (DVT → post-thrombotic syndrome is the most important secondary cause).
Clinical features: Cosmetic concern, aching (worse standing, better elevation), heaviness, ankle swelling, night cramps, itching → skin changes (pigmentation, eczema, LDS, atrophie blanche) → ulceration (medial gaiter area, painless unless infected).
Must check ABPI before compression — absolute CI if < 0.4.
Venous ulcer: Shallow, sloping edge, gaiter area, painless, haemosiderin-stained surrounding skin, pulses present.
Acute LDS mimics cellulitis — don't be fooled.
Marjolin's ulcer (SCC transformation) in 2% of long-standing venous ulcers.
Active Recall - CVI and Varicose Veins (Definition to Clinical Features)
[1] Senior notes: felixlai.md (Chapter 13: Vascular System — Chronic Venous Disease, pp. 941–949; Varicose Veins, pp. 950–961) [2] Senior notes: maxim.md (Section 7.3: Chronic Venous Insufficiency, pp. 169–175) [3] Senior notes: maxim.md (CEAP Classification, Varicose Veins section, pp. 170–175) [4] Edinburgh Vein Study epidemiological data (referenced in lecture context) [5] Lecture slides: WCS 002 - Toe gangrene and leg ulcer - by Prof SWK Cheng.pdf [6] Lecture slides: GC 178. An ugly wound Wound healing; Wound infection; Anti-septic technique.pdf [7] Image credit: Amboss (saphenofemoral junction anatomy)
Differential Diagnosis of CVI and Varicose Veins
When a patient presents with lower limb swelling, skin changes, visible veins, or ulceration, your job is to work through a structured differential. The key question is: is this truly venous disease, or is something else mimicking it? Let me walk you through this systematically.
The differential depends on the presenting complaint. A patient with varicose veins/CVI may present with one or more of:
- Visible dilated leg veins
- Lower limb oedema
- Leg pain / heaviness
- Skin changes (pigmentation, eczema, lipodermatosclerosis)
- Lower limb ulceration
Each of these presentations has its own differential, but there is considerable overlap. The mermaid diagram below maps out the clinical reasoning:
| Condition | Key Distinguishing Features | Why It Mimics CVI/VV |
|---|---|---|
| Primary varicose veins | Most common. GSV/SSV distribution. Risk factors (age, female, family history, standing occupation). Demonstrable reflux on duplex | The "diagnosis" itself — dilated tortuous subcutaneous veins ≥ 3 mm with reflux |
| Secondary varicose veins (post-thrombotic) | History of DVT. Skin changes may be more severe for the degree of visible varicosity. Deep venous incompetence on duplex | DVT destroys valves → secondary reflux → venous hypertension → same endpoint as primary VV |
| Klippel-Trénaunay syndrome | Congenital venous malformation with triad: varicose veins (often lateral thigh — atypical distribution), port wine stains, bony/soft tissue hypertrophy [2][7] | Varicose veins present from childhood/adolescence in atypical distribution (lateral thigh rather than medial GSV territory). The port wine stain and limb hypertrophy are the giveaways |
| Parkes-Weber syndrome | Multiple congenital AV fistulae with limb hypertrophy, possibly causing high-output heart failure [2][7] | AV fistulae increase venous pressure → venous dilation. Listen for bruit/thrill over the limb. Limb may be warm (arterialised venous blood) |
| Saphena varix | Compressible groin lump at the SFJ with a cough impulse. Disappears on lying down [1][2] | Must be distinguished from femoral hernia (below and lateral to pubic tubercle, may be irreducible, no venous hum) and inguinal lymphadenopathy (firm, non-compressible, no cough impulse) |
| Pelvic venous congestion syndrome | Chronic pelvic pain (worse standing, post-coital), vulval/perineal/upper thigh varices, often in multiparous women | Reflux from incompetent ovarian/internal iliac veins → atypical distribution varicosities. Suspect when varices are in vulval/perineal/upper medial thigh distribution without SFJ/SPJ incompetence |
| IVC obstruction | Bilateral prominent abdominal wall/lower limb veins, bilateral leg oedema, possible pelvic mass or history of IVC filter | Obstruction of IVC forces venous return through superficial collateral pathways → visible dilated veins on abdomen and legs bilaterally |
Lateral Thigh Varicose Veins
If you see varicose veins on the lateral aspect of the thigh, this is NOT typical GSV or SSV territory. Think Klippel-Trénaunay syndrome (congenital) or isolated lateral accessory saphenous vein reflux. Always ask about onset (childhood = congenital) and look for port wine stains and limb length discrepancy.
This is a crucial differential because CVI is only one cause of leg swelling, and the treatment differs radically. The key is to determine whether the oedema is unilateral vs. bilateral and pitting vs. non-pitting.
| Condition | Unilateral/Bilateral | Pitting? | Key Distinguishing Features | Why It Mimics CVI |
|---|---|---|---|---|
| CVI | Usually unilateral (or asymmetric bilateral) | Yes (pitting) initially | Skin changes (pigmentation, LDS, eczema), varicose veins, gaiter area distribution. Worse at end of day, better with elevation | — |
| DVT | Usually unilateral | Yes (pitting) | Acute onset, painful, warm, red, swollen calf. Homan's sign unreliable. Risk factors: immobility, malignancy, recent surgery, OCP [1][3] | Acute venous obstruction causes leg swelling. A missed DVT can progress to PE — this is the dangerous diagnosis to exclude |
| Lymphoedema | Usually unilateral initially → bilateral | Initially pitting → later non-pitting (warty, thickened skin) | Stemmer sign positive (unable to lift skin fold of 2nd toe). Dorsum of foot involved. Does not improve overnight. No pigmentation/eczema. Causes: filariasis (MC worldwide), malignancy/post-radiation (MC in developed countries), primary (Milroy, Meige) [4] | Both cause leg swelling. Key difference: lymphoedema affects the dorsum of the foot and spares the gaiter area; CVI preferentially affects the gaiter area. Lymphoedema skin becomes thickened and fibrotic, not pigmented |
| Lipodema | Bilateral, symmetric | No (non-pitting) | Fat distribution disorder, almost exclusively in women. Symmetric bilateral leg enlargement sparing the feet. Tender to palpation. Easy bruising. No Stemmer sign | Bilateral swollen legs that are tender — but the feet are spared (the "cuff sign" at the ankle where fat stops and normal foot begins) |
| Cardiac failure | Bilateral, symmetric | Yes (pitting) | Raised JVP, orthopnoea, PND, bilateral leg oedema, hepatomegaly, sacral oedema if bedridden | Bilateral pitting oedema from elevated systemic venous pressure. But this is generalised — no focal skin changes, no varicose veins |
| Hypoalbuminaemia (nephrotic syndrome, liver cirrhosis, protein-losing enteropathy) | Bilateral, symmetric | Yes (pitting) | Periorbital oedema (nephrotic), ascites (liver), generalised oedema. Low serum albumin. No skin changes of CVI | Reduced oncotic pressure → transudative oedema. Bilateral, generalised, no focal venous signs |
| Drug-induced (CCBs e.g. amlodipine, NSAIDs, steroids, pioglitazone) | Bilateral, symmetric | Yes (pitting) | Temporal relationship with drug initiation. No skin changes | CCBs cause arteriolar vasodilation → increased capillary hydrostatic pressure → dependent oedema. Very common! |
| Dependency / immobility oedema | Bilateral | Yes (pitting) | Wheelchair-bound, elderly, paralysed patients. No skin changes initially | Lack of calf muscle pump + gravity = venous pooling and transudation |
DVT Must Be Excluded
CVI causes a dull ache/heaviness that is worse with standing and better with elevation [1]. But leg pain has many causes:
| Condition | Character of Pain | Key Differentiators |
|---|---|---|
| CVI / varicose veins | Dull ache, heaviness, burning. Worse with prolonged standing, better with elevation and walking [1] | Visible varicosities, skin changes, oedema |
| DVT | Acute, unilateral calf pain and swelling. Tender on palpation [3] | Acute onset, risk factors (Virchow's triad), calf tenderness and swelling |
| Superficial thrombophlebitis | Localised pain, redness, and tenderness along a palpable, tender, cord-like superficial vein [1] | The affected vein is visible and palpable as a tender cord. Surrounding erythema and warmth |
| Peripheral arterial disease (intermittent claudication) | Cramping pain in calf/buttock on walking, relieved by rest [5] | Pain with exercise (not standing). Absent pulses, reduced ABPI, cold/hairless limb. Pain radiation: distal → proximal. Relieved by rest. Walking uphill worsens it [5] |
| Sciatica / lumbar radiculopathy | Sharp, shooting pain radiating from back/buttock down the leg in a dermatomal distribution | Back pain, positive straight-leg raise, neurological deficits. Neurogenic claudication (spinal stenosis): pain radiates proximal → distal, worsened by walking downhill, relieved by bending forward ("park bench to park bench" rather than "shop window to shop window") [5] |
| Cellulitis | Diffuse erythema, warmth, tenderness, swelling. Systemic features (fever, raised WCC/CRP) | Unilateral. Poorly demarcated erythema. May have entry wound. Responds to antibiotics. Acute LDS is often misdiagnosed as cellulitis [2] |
| Ruptured Baker's cyst | Acute onset posterior calf pain and swelling mimicking DVT [3] | History of knee arthropathy (RA, OA). Popliteal fossa fullness. USG confirms |
| Muscle strain / tear | History of trauma or sudden exertion. Localised tenderness | Temporal relationship with activity. Bruising may appear |
Skin changes in CVI are distinctive but can be mimicked:
| CVI Skin Change | Differential / Mimic | How to Distinguish |
|---|---|---|
| Hyperpigmentation (haemosiderin) | Haemochromatosis, chronic dermatitis, fixed drug eruption, post-inflammatory hyperpigmentation | CVI pigmentation is in the gaiter area with associated oedema, varicosities. Haemochromatosis is generalised ("bronze diabetes") |
| Venous eczema (stasis dermatitis) | Allergic contact dermatitis (e.g., from wound dressings, topical agents), asteatotic eczema | Contact dermatitis has a sharp boundary matching the allergen contact site. Patch testing helps. Venous eczema is in CVI distribution with other venous signs |
| Lipodermatosclerosis (acute) | Cellulitis, erysipelas, superficial thrombophlebitis [2] | Acute LDS: painful, red, hot, tender medial lower leg in context of known CVI. Cellulitis: entry point, systemic features, responds to antibiotics. LDS does NOT respond to antibiotics. Thrombophlebitis: tender cord along a vein |
| Pretibial myxoedema | CVI skin changes | Pretibial myxoedema occurs in Graves' disease — localised thickening of pretibial skin with a "peau d'orange" appearance. Associated with thyroid eye disease, thyroid acropachy. No varicosities or venous oedema |
This is the most commonly examined differential. The lecture slides [6] emphasise that all lower limb ulcers must be characterised by type because management differs fundamentally.
| Feature | Venous Ulcer | Arterial Ulcer | Neuropathic Ulcer | Pressure Ulcer | Malignant Ulcer (Marjolin) |
|---|---|---|---|---|---|
| Location | Gaiter area (medial malleolus) | Tips of toes, between digits, lateral malleolus, heel | Plantar foot, over metatarsal heads | Bony prominences, heel, sacrum | At site of chronic ulcer/scar |
| Depth | Shallow | Deep | Shallow or deep | Deep | Variable, often deep with rolled/everted edge |
| Edge | Gently sloping | Punched-out | Punched-out | Macerated | Everted, raised, irregular |
| Base | Slough with granulation tissue | Unhealthy, necrotic | Not very painful | Often macerated | Fungating, friable tissue |
| Pain | Usually painless unless infected | Very painful | Painless (neuropathy) | Variable | May be painless initially |
| Surrounding skin | Haemosiderin-stained, eczematous, fibrotic, oedematous [2][6] | Cold, thin, shiny, hairless, delayed cap refill, gangrene | Dry, cracked, calluses, loss of sensation | Skin atrophy, muscle wasting | May show chronic CVI changes |
| Pulses | Present | Absent or weak | Present | Present | Present |
| Associations | VV, DVT, phlebitis | DM, HT, PVD, smoking | DM, trauma | Immobility | 2% of long-standing venous ulcers → SCC [2] |
Other important ulcer differentials:
- Vasculitic ulcers: Associated with autoimmune conditions (RA, SLE, polyarteritis nodosa). Punched-out, painful, often multiple, may have palpable purpura. Check ESR, ANA, ANCA, complement
- Pyoderma gangrenosum: Rapidly enlarging, very painful ulcer with violaceous undermined borders. Associated with IBD, RA, haematological malignancies. Pathergy phenomenon (worsens with debridement — important to recognise so you DON'T debride it)
- Marjolin's ulcer: Malignant transformation (usually SCC, rarely BCC) occurring in chronically scarred or ulcerated tissue, seen in ~2% of long-standing venous ulcers [2][6]. Suspect if a chronic ulcer changes character — becomes raised, has an everted edge, bleeds easily, or fails to heal despite adequate therapy. Requires 4-quadrant biopsy and palpation of groin lymph nodes [6]
Pyoderma Gangrenosum Trap
If a rapidly expanding, extremely painful leg ulcer with violaceous undermined edges worsens after surgical debridement — think pyoderma gangrenosum. This demonstrates "pathergy" (trauma worsens the lesion). Treatment is immunosuppression (steroids, cyclosporine), NOT surgery. Debridement will make it worse.
A saphena varix at the SFJ can mimic other groin lumps [1][2]:
| Diagnosis | Key Features | How to Distinguish from Saphena Varix |
|---|---|---|
| Saphena varix | Compressible, with cough impulse, disappears on lying down, bluish tinge, located at SFJ (2.5 cm inferolateral to pubic tubercle). Venous hum may be present | — |
| Femoral hernia | Below and lateral to pubic tubercle. Cough impulse present. May be irreducible. No blue colour. Bowel sounds may be auscultated | Femoral hernia is typically not easily compressible and does not have a venous hum. Location is similar but hernia sits more lateral |
| Inguinal lymphadenopathy | Firm, non-compressible, no cough impulse. May be tender (infection) or hard/fixed (malignancy) | No relationship to venous system. Look for source of infection/malignancy in the drainage territory |
| Femoral artery aneurysm | Expansile, pulsatile mass. Located over femoral artery | Pulsatile rather than compressible. Duplex confirms |
| Psoas abscess | Fluctuant mass below inguinal ligament. Patient holds hip in flexion. Psoas sign positive. May have fever, back pain | Often secondary to spinal TB or Crohn's disease. CT confirms |
When working up a patient with suspected CVI or varicose veins, ask yourself three questions:
- Is this truly venous disease? — Exclude arterial (check pulses, ABPI), lymphatic (check Stemmer sign), cardiac (check JVP, bilateral), metabolic (check albumin), or drug-induced causes
- If venous, is it primary or secondary? — Exclude DVT (duplex), pelvic pathology (abdominal exam, pelvic USS), and congenital causes (Klippel-Trénaunay, Parkes-Weber)
- If there is an ulcer, what type? — Venous vs. arterial vs. neuropathic vs. mixed vs. malignant (Marjolin) vs. other (vasculitic, PG)
High Yield Summary
Core differential for lower limb oedema: CVI, DVT, lymphoedema, cardiac failure, hypoalbuminaemia, lipodema, drug-induced (CCBs), dependency oedema. Use unilateral vs. bilateral and pitting vs. non-pitting to narrow it down.
Core differential for lower limb ulcer: Venous (gaiter area, shallow, painless, sloping edge), arterial (toes/heel, deep, punched-out, painful, absent pulses), neuropathic (plantar, painless, punched-out), pressure (bony prominences), malignant/Marjolin (2% of chronic venous ulcers → SCC).
Must-exclude diagnoses: DVT (before attributing swelling to CVI), PAD (before applying compression — check ABPI), Marjolin ulcer (4-quadrant biopsy for any non-healing chronic ulcer).
Acute LDS mimics cellulitis — medial lower leg, painful, hot, red, tender but in context of CVI and does NOT respond to antibiotics.
Lateral thigh varicosities → think Klippel-Trénaunay (congenital: VV + port wine stain + limb hypertrophy).
Saphena varix DDx: femoral hernia, inguinal lymphadenopathy, femoral artery aneurysm, psoas abscess.
Lymphoedema vs. CVI: Lymphoedema affects dorsum of foot, Stemmer sign positive, non-pitting in late stages, warty/thickened skin. CVI affects gaiter area, pitting, haemosiderin pigmentation.
Active Recall - DDx of CVI and Varicose Veins
References
[1] Senior notes: felixlai.md (Chapter 13: Vascular System — Chronic Venous Disease, pp. 941–961) [2] Senior notes: maxim.md (Section 7.3: Chronic Venous Insufficiency, pp. 169–175) [3] Senior notes: felixlai.md (DVT and PE section, pp. 962–964) [4] Senior notes: maxim.md (Section 4.6: Lymphoedema) [5] Senior notes: maxim.md (Chronic limb ischaemia / Differential diagnosis, p. 169); Senior notes: felixlai.md (Chronic Arterial Insufficiency) [6] Senior notes: maxim.md (Section 7.4: Lower extremity ulcers, pp. 174–175) [7] Lecture slides: GC 201. Skin ulcers skin and subcutaneous lesions; skin cancer.pdf (p37 — Vascular malformations, Klippel-Trenaunay, Parkes-Weber)
Diagnostic Criteria, Algorithm, and Investigations
1. Diagnostic Criteria — What Makes the Diagnosis?
Unlike conditions such as rheumatic fever or SLE, CVI and varicose veins do not have strict "diagnostic criteria" in the traditional sense (no scoring system with X out of Y needed). Instead, the diagnosis is made through a combination of clinical assessment and confirmatory imaging, structured by the CEAP classification.
Let me lay out the diagnostic requirements for each key entity:
The diagnosis requires ALL of [1][2]:
- Clinical: Visible dilated, tortuous subcutaneous veins ≥ 3 mm in diameter, measured in the upright position
- Functional: Demonstrable reflux — this is confirmed by duplex ultrasound showing retrograde flow with valve closure time > 0.5 seconds [1][2]
Without demonstrable reflux on duplex, a dilated vein is just that — a dilated vein. It is the reflux that makes it a "varicose vein" by definition.
The CEAP classification itself serves as the diagnostic framework — once you have completed your clinical assessment and investigations, you assign the full CEAP descriptor. This is the international standard for documenting and communicating the diagnosis [1][2][3]:
| Component | What You're Classifying | How You Determine It |
|---|---|---|
| C (Clinical) | What you see and what the patient reports (C0–C6, S or A) | Clinical inspection and history |
| E (Etiological) | Why it happened (Ec, Ep, Esi, Ese, En) | History plus context: congenital? idiopathic primary disease? post-DVT / intraluminal damage? extrinsic compression or calf-pump failure? |
| A (Anatomical) | Which venous system is affected (As, Ap, Ad, An) | Duplex USG |
| P (Pathophysiological) | What went wrong (Pr, Po, Pr,o, Pn) | Duplex USG |
The key insight: C is clinical; E, A, and P require investigations (primarily duplex USG) to complete.
You Cannot Complete CEAP Without Duplex USG
Clinical inspection alone gives you the C class. But to assign the A (anatomical) and P (pathophysiological) components — i.e., to know whether it's reflux vs. obstruction, and whether the superficial, deep, or perforator system is involved — you need duplex ultrasound. This is why duplex is the cornerstone investigation.
Here is the systematic approach to diagnosing CVI and varicose veins, from initial presentation through to pre-operative planning:
The history in CVI/varicose veins is not just a formality — it determines etiology (E component of CEAP), guides investigation, and identifies contraindications to treatment [1][2]:
| History Component | Specific Questions | Clinical Reasoning |
|---|---|---|
| Presenting complaint | Onset, duration, progression. Cosmetic concern vs. symptomatic (pain, heaviness, swelling, itching) | Determines whether treatment is needed and urgency. Acute onset of unilateral swelling → think DVT, not chronic CVI |
| Symptom pattern | Worse at end of day? Relieved by elevation? Worse with standing? | Venous symptoms worsen throughout the day and with standing, and are relieved by elevation and walking [1]. If pain is worse with walking and relieved by rest → think arterial |
| PMHx — DVT | Previous DVT or superficial thrombophlebitis [1] | Post-thrombotic syndrome is the most common secondary cause. Also, DVT must be excluded as it is a contraindication to varicose vein surgery [1] |
| PMHx — Pregnancy | Number of pregnancies, current pregnancy | Increased abdominal pressure + hormonal changes. Pregnancy is a contraindication to surgery [1] |
| PMHx — Comorbidities | Heart failure, liver disease, renal disease, thyroid disease, diabetes | Exclude other causes of oedema. Diabetes → check for neuropathic component of ulcers |
| Drug history | OCP, HRT, CCBs, NSAIDs, anticoagulants | OCP/HRT increase DVT risk. CCBs cause dependent oedema (mimic). Anticoagulants relevant for surgical planning |
| FHx | Family history of varicose veins [1] | Strong genetic component in primary varicose veins |
| SHx | Occupation requiring prolonged standing [1], exercise habits, smoking | Occupational risk; exercise promotes calf pump; smoking → assess atherosclerotic risk if mixed disease |
4. Physical Examination — A Systematic Approach
The examination should be performed with the patient standing (veins fill in the dependent position) with the legs fully exposed [1][2]:
- Surgical scars — previous venous surgery (recurrence is common — 30%) [2]
- Location of varicosities — the single most important inspection finding for localising incompetence [1]:
| Distribution | Implies Incompetence Of |
|---|---|
| Medial thigh and medial calf | Great saphenous vein (GSV) |
| Posterior calf | Small saphenous vein (SSV) |
| Anterolateral thigh and anterolateral calf | Isolated incompetence of proximal anterolateral GSV tributary |
| Lateral thigh (atypical) | Consider Klippel-Trénaunay or lateral accessory saphenous reflux |
- Signs of CVI — systematically assess for all C-class features [1][2]:
- Corona phlebectatica (malleolar flare)
- Hyperpigmentation (gaiter area)
- Venous eczema
- Lipodermatosclerosis (hyperpigmentation + erythema + induration + tenderness — palpate!) [2]
- Atrophie blanche
- Healed or active ulceration (medial gaiter area)
- Palpate along course of GSV and SSV and their tributaries for varicosities and tenderness [1][2]
- Check peripheral pulses — rule out PAD since management includes compression [1][2]. This is not optional — it is a safety-critical step
- Pitting oedema — confined to ankle area usually, may extend proximally [1]
- Saphena varix — at the inguinal region: a compressible lump with cough impulse that refills on release [1][2]
- Inguinal lymph nodes — if venous ulcers present, check for lymphadenopathy (infection or Marjolin transformation) [2]
- Neurological function — test sensation (e.g., sural nerve territory) if surgical scars present, to document pre-existing nerve damage [2]
This classic bedside test localises the level of valvular incompetence. Although largely superseded by duplex USG, it remains an exam favourite [1][2]:
Procedure [1]:
- Patient lies supine → elevate leg to empty superficial veins (or stroke blood proximally)
- Apply tourniquet tightly around the upper thigh (just below SFJ)
- Patient stands up quickly → observe filling of varicose veins
Interpretation [1]:
| Finding | Interpretation | Explanation |
|---|---|---|
| NO refilling below tourniquet while standing; rapid filling on release | SFJ incompetence only | The tourniquet blocked reflux from the SFJ, keeping the veins empty. When released, blood refluxes down from the femoral vein through the incompetent SFJ |
| Rapid refilling below tourniquet while standing | Incompetence at sites BELOW the tourniquet (perforators or other levels) | Blood is entering the superficial system below the tourniquet level — through incompetent perforators or lower reflux points |
| Partial filling while standing; further filling on release | SFJ incompetence AND perforator/other incompetence below | Both levels contributing |
This tests deep venous patency [2]:
- Apply tourniquet around the SFJ (blocking superficial reflux)
- Ask the patient to walk (activating the calf muscle pump)
- If the deep system is patent: walking should empty the leg via the deep veins → varicosities decrease
- If the deep system is NOT patent: walking causes swelling and pain — blood cannot drain through the deep system and the tourniquet blocks superficial drainage → the leg is trapped
Why Perthes' Test Matters
If the deep venous system is occluded (e.g., old DVT), the superficial varicose veins may be the patient's ONLY route for venous return. Stripping or ablating these veins would be catastrophic — you'd remove their only outflow pathway. This is why assessing deep venous patency is essential before surgery, and Perthes' test is the clinical correlate of what duplex USG confirms definitively.
- Auscultate over varicosities for a continuous bruit — suggests AV malformation [1]
- Examine inguinal region for mass or lymphadenopathy causing venous outflow obstruction [1]
- Abdominal and PR examination — if secondary causes suspected (pelvic mass obstructing IVC/iliac veins) [2]
- ABPI measurement — to rule out PAD before compression therapy [2]
5. Investigation Modalities
What it is: Ratio of the highest systolic BP at the ankle (dorsalis pedis or posterior tibial) to the highest brachial systolic BP, measured using a handheld Doppler and sphygmomanometer [1][5].
Why you need it: Compression therapy (stockings, bandaging) is the mainstay of CVI management. Applying compression to an ischaemic limb can cause tissue necrosis. ABPI is therefore a mandatory safety check before any compression or surgical planning [2].
| ABPI Value | Interpretation | Clinical Implication |
|---|---|---|
| > 1.3 | Calcified (incompressible) arteries — e.g., diabetes, CKD | ABPI unreliable. Need alternative arterial assessment (toe pressures, duplex) |
| 0.9–1.3 | Normal | Safe for full compression therapy |
| 0.5–0.9 | Moderate PAD (claudication range) | Mixed arterio-venous disease. Use reduced compression with caution. Needs arterial assessment |
| < 0.5 | Severe PAD (critical limb ischaemia range) | Compression is dangerous |
| < 0.4 | Absolute contraindication to compression [2] | Do NOT apply compression stockings or bandaging |
ABPI Before Compression — Non-Negotiable
Every student and junior doctor must check ABPI before prescribing compression. An ABPI below 0.4 is an absolute contraindication. In diabetics, ABPI may be falsely elevated due to calcified arteries — use toe pressures instead.
5.2 Venous Duplex Ultrasound — The Gold Standard Investigation
This is the cornerstone investigation for CVI and varicose veins. "Duplex" means it combines two modalities [1][2]:
- B-mode USG (real-time 2D greyscale imaging) — shows anatomy (vein diameter, course, thrombus)
- Doppler (colour flow and spectral waveform) — shows haemodynamics (flow direction, velocity, reflux)
It answers every question you need answered before making treatment decisions:
| Question | How Duplex Answers It |
|---|---|
| Is there reflux? | Reflux = retrograde flow in the reverse direction to physiological flow. Valve closure time > 0.5 seconds is defined as abnormal [1]. Elicited by calf compression-release (manual squeeze or cuff deflation) or Valsalva |
| Where is the reflux? | Maps reflux at SFJ, SPJ, along GSV/SSV trunks, perforators — completing the A component of CEAP |
| Which junctions are incompetent? | SFJ and/or SPJ incompetence determines the surgical approach [1] |
| What is the vein diameter? | Determines suitability for endovenous treatment (most devices work best in 5–12 mm diameter range) |
| Is the vein tortuous? | Tortuosity affects whether an endovenous catheter can be passed. Very tortuous veins may need surgical stripping instead [2] |
| Is there a saphena varix? | Visible on B-mode as a dilated segment at the SFJ |
| Is there DVT? | DVT must be excluded since it is a contraindication to varicose vein surgery [1]. B-mode shows non-compressible vein (normally a vein should be fully compressible with probe pressure). Intraluminal thrombus may be visible |
| Is the deep system competent? | Competence of the deep venous system must be assessed — if both deep and superficial systems are incompetent, surgery on the superficial system alone is contraindicated (blood has no alternative route) [1][2] |
| Is there perforator incompetence? | Incompetent perforators appear as bidirectional flow with reflux > 0.35 seconds |
On transverse B-mode at the groin, three circular structures are visible side by side:
- Common femoral artery (CFA) — larger circle, pulsatile
- Common femoral vein (CFV) — compressible circle
- Great saphenous vein (GSV) at the SFJ — smaller circle joining the CFV
This looks like Mickey Mouse's head and ears — a classic teaching image for locating the SFJ.
- All patients being considered for intervention (endovenous or surgical)
- Recurrent varicose veins [1]
- Complications of CVI: hyperpigmentation, venous stasis eczema, venous ulcers [1]
- History of superficial thrombophlebitis or DVT [1]
- Atypical presentation or suspected secondary cause
- Pre-operative mapping and planning
The patient is examined in the standing or reverse Trendelenburg position (to maximise venous pooling). The sonographer:
- Places the probe over the vein segment being tested
- Squeezes the calf (or uses a pneumatic cuff) to push blood proximally
- Releases → observes for retrograde flow on the Doppler waveform
- If reflux lasts > 0.5 seconds → incompetent valve [1]
For perforators, the threshold is slightly different: > 0.35 seconds is considered abnormal.
- Pen-like handheld probe that detects blood flow direction using the Doppler principle [1]
- Helpful for screening reflux at SFJ and SPJ in the office setting [1]
- Limitations: Unable to quantitate reflux or provide precise anatomical information [1] — it tells you "there is reflux here" but not exactly which vein, how much, or whether the deep system is involved
- In modern practice, this has been largely replaced by duplex USG for definitive assessment, but remains useful as a quick bedside screening tool
- Indication: When a secondary cause is suspected [2] — e.g., pelvic mass (ovarian cyst, fibroid, pelvic malignancy), IVC obstruction, May-Thurner syndrome
- Look for: Pelvic masses compressing the iliac veins, lymphadenopathy, ascites
- Consider in:
- Young patients with unexplained unilateral CVI
- Patients with no typical risk factors
- New-onset varicose veins with abdominal symptoms
- Not routine — reserved for complex or recurrent cases
- Indications:
- Suspected iliocaval obstruction (May-Thurner syndrome, IVC thrombosis)
- Pelvic venous congestion syndrome
- Planning for deep venous reconstruction or stenting
- Congenital venous anomalies (Klippel-Trénaunay)
- CT venography: Good spatial resolution, involves contrast and radiation
- MR venography: No radiation, excellent soft tissue contrast, but longer acquisition time and limited availability
- Intravascular ultrasound (IVUS): Increasingly used during endovascular procedures to assess iliac vein stenosis (May-Thurner) — gives cross-sectional area and degree of compression from within the vessel
Laboratory tests are not used to diagnose CVI itself but are important in the work-up of complications and differential diagnoses:
| Investigation | Indication | What You're Looking For |
|---|---|---|
| CBC with differential | Venous ulcer with suspected infection | Leucocytosis (infection). Also baseline before surgery |
| CRP / ESR | Suspected infection, vasculitis | Elevated in infection and inflammation |
| Wound swab for C/ST | Infected venous ulcer | Identify causative organism (commonly S. aureus) and guide antibiotic therapy |
| Serum albumin | Exclude hypoalbuminaemia as cause of oedema | Low albumin → nephrotic, liver disease, malnutrition |
| Renal / liver function | Exclude non-venous causes of oedema | Renal failure → fluid overload; liver failure → hypoalbuminaemia + portal hypertension |
| Thyroid function | Pretibial myxoedema mimicking CVI skin changes | Hyperthyroidism (Graves) |
| Coagulation screen + thrombophilia screen | Young patient with DVT-related CVI, recurrent VTE | Factor V Leiden, protein C/S deficiency, antithrombin III deficiency, antiphospholipid antibodies |
| HbA1c / fasting glucose | Diabetic patient with ulcer | Assess glycaemic control; diabetic ulcers have different pathogenesis and management |
| 4-quadrant biopsy | Non-healing venous ulcer | Exclude Marjolin's ulcer (SCC transformation, ~2% of chronic venous ulcers) [2] |
When a patient presents with a lower limb ulcer in the context of CVI:
- Duplex USG — confirm venous aetiology and plan venous treatment
- ABPI — exclude arterial component (mixed ulcers are common ~15%)
- Wound swab C/ST — if signs of clinical infection (erythema, purulent discharge, cellulitis, systemic sepsis)
- 4-quadrant biopsy + palpate groin lymph nodes — if ulcer is chronic, non-healing, or has suspicious features (raised/everted edges, bleeding easily) → exclude Marjolin's ulcer [2][6]
- Bloods: CBC, CRP, albumin, HbA1c
| Clinical Scenario | First-Line Investigation | Additional Investigations |
|---|---|---|
| Symptomatic varicose veins (C2S) | ABPI + Duplex USG | None usually needed |
| CVI with skin changes (C4–C6) | ABPI + Duplex USG | Bloods (CBC, CRP, albumin). Wound swab if infected. Biopsy if non-healing |
| Recurrent varicose veins | Duplex USG (essential — map the recurrence) | Consider CT/MR venography if complex anatomy |
| Suspected secondary CVI | Duplex USG + USG abdomen/pelvis | CT/MR venography for iliocaval pathology |
| Young patient with DVT-related CVI | Duplex USG + thrombophilia screen | CT venography if May-Thurner suspected |
| Venous ulcer, non-healing | ABPI + Duplex USG + wound swab + 4-quadrant biopsy | Exclude Marjolin's, mixed ulcer, vasculitis |
High Yield Summary
Diagnosis of varicose veins requires visible dilated tortuous veins ≥ 3 mm in upright position PLUS demonstrable reflux (valve closure time > 0.5 s on duplex USG).
CEAP is the diagnostic framework: C = clinical inspection; E, A, P = require duplex USG to complete.
Duplex USG is the gold standard — it answers: Is there reflux? Where? Is the deep system competent? Is there DVT? Is the vein suitable for endovenous treatment?
ABPI is mandatory before compression — absolute contraindication if ABPI < 0.4. In diabetics with calcified arteries (ABPI > 1.3), use toe pressures instead.
Tourniquet test: No refilling below tourniquet = incompetence at tourniquet level. Rapid refilling despite tourniquet = incompetence below that level. Largely replaced by duplex but still examined.
Perthes' test assesses deep venous patency: tourniquet at SFJ + walking. If deep system is occluded → pain and swelling (superficial veins are the only outflow — do NOT ablate them).
DVT is a contraindication to varicose vein surgery — must always be excluded by duplex before any intervention.
Combined deep + superficial incompetence → conservative management only (surgery on superficial system would remove the patient's only functional outflow pathway).
Non-healing venous ulcer → 4-quadrant biopsy to exclude Marjolin's ulcer (SCC, 2%).
Active Recall - Diagnosis of CVI and Varicose Veins
References
[1] Senior notes: felixlai.md (Chapter 13: Vascular System — Chronic Venous Disease, pp. 941–957; Varicose Veins, pp. 950–957) [2] Senior notes: maxim.md (Section 7.3: Chronic Venous Insufficiency, pp. 169–175) [3] Senior notes: felixlai.md (CEAP classification tables, pp. 944–945, 952–953) [5] Lecture slides: WCS 002 - Toe gangrene and leg ulcer - by Prof SWK Cheng.pdf [6] Senior notes: maxim.md (Section 7.4: Lower extremity ulcers, pp. 174–175)
Management of CVI and Varicose Veins
Before diving into modalities, let's understand what we're trying to achieve. The goals of treatment address the underlying pathophysiology directly [1][8]:
- Improve O₂ transport to skin and subcutaneous tissue — by reversing venous hypertension, which causes pericapillary fibrin cuffs that block O₂ diffusion
- Decrease inflammation — venous hypertension triggers a chronic inflammatory cascade (WBC trapping, protease release); reducing venous pressure breaks this cycle
- Decrease oedema and compress dilated veins — by external compression and reducing venous reflux, you restore Starling forces towards normal and reduce venous pooling
The overarching principle: reduce venous hypertension. Everything else follows from this.
The management approach is determined by CEAP class, duplex findings, and patient factors:
3. Conservative Management
Conservative management is the foundation for ALL patients regardless of CEAP class — it is never wrong, and for many patients it is sufficient [1][2][8]:
| Intervention | Mechanism | Details |
|---|---|---|
| Avoid prolonged standing [2] | Reduces the hydrostatic column and venous pooling | Advise regular walking breaks during work. Alternate between standing and sitting |
| Weight loss [2] | Reduces abdominal pressure → reduces impedance to venous return; reduces chronic inflammation | Significant benefit even with modest weight loss (5–10%) |
| Increase exercise [2] | Promotes calf muscle pump — the "peripheral heart" that actively propels blood from deep veins towards the heart | Walking, calf raises, swimming. Avoid prolonged static standing or sitting |
| Leg elevation | Eliminates the hydrostatic pressure column. When legs are above the level of the heart, venous return is gravity-assisted | Advise elevating legs when sitting, sleeping with foot of bed raised |
3.2 Compression Therapy
This is the single most important conservative intervention and the backbone of CVI management [1][2][8]:
- At least 20 mmHg at the ankle with decreasing pressure proximally [2] — this creates a pressure gradient that pushes blood from distal (high pressure) to proximal (lower pressure), augmenting venous return
- Available in ranges: 20–30, 30–40, or 40–50 mmHg [1]
- Stocking length: knee-high to waist-high; should cover all symptomatic varicosities
- Below-knee stockings are usually prescribed due to better patient acceptance [1]
- Relieves symptoms and improves quality of life (QOL) [1][8]
- BUT no evidence that compression prevents occurrence or progression of varicose veins [1] — it is symptomatic treatment, not disease-modifying
- Compliance is poor and long-term tolerance is limited (difficult to don/doff, hot in summer) [1]
Pre-requisite: ABPI must be checked — absolute contraindication if ABPI < 0.4 [2]. Why? Because compression on an ischaemic limb would further reduce arterial perfusion pressure, potentially causing tissue necrosis.
Complications of compression stockings [2]:
- Pressure necrosis — if applied too tightly or incorrectly, especially over bony prominences
- Contact dermatitis — skin sensitivity to stocking material
- Fungal infection — warm, moist environment under the stocking
Compression Stockings Are Contraindicated in Acute DVT
Many students confuse this. While compression is the mainstay of CVI treatment, it is contraindicated in patients with acute DVT [1]. In acute DVT, compression can theoretically dislodge thrombus or worsen symptoms. Once DVT has been treated and the acute phase has passed, compression is then used to prevent post-thrombotic syndrome.
- Combination of compression therapy with zinc oxide paste that assists wound healing
- Indication: Skin ulceration — provides continuous compression + topical therapy to prevent further skin breakdown
- Advantages: Requires minimal patient involvement; continuous compression and topical therapy
- Disadvantages: Bulky and uncomfortable (poor compliance); ulcer cannot be monitored after boot is applied; technique is labour-intensive and operator-dependent
- The gold standard for venous ulcer management [6]
- Components: orthopaedic wool → cotton crepe → elastic bandage → cohesive bandage [6]
- Achieves sustained graduated compression (typically 40 mmHg at the ankle)
- Pre-requisite: ABPI > 0.4 [6]
- Conservative management with 4-layer bandaging heals 50–70% of venous ulcers within 3 months [6]
- Provides dynamic sequential compression — intermittent inflation/deflation of pneumatic cuffs
- Used primarily for DVT prophylaxis in hospitalised patients but also used to treat venous insufficiency
- Particularly useful when patients cannot tolerate stockings or in refractory oedema
- Daflon (micronised purified flavonoid fraction / micronised diosmin) [2]: A venotonic that increases venous tone and lymphatic drainage
- Mechanism: Increases venous wall contractility by modulating noradrenaline release; reduces capillary permeability; has anti-inflammatory effects (reduces leucocyte adhesion)
- Good for oedema (CEAP ≥ C3) [2]
- Limited role in earlier disease; used as adjunctive therapy rather than primary treatment
- Available over the counter in Hong Kong
For patients with C5/C6 disease:
- Leg elevation and encourage mobilisation [6] — elevation reduces venous pressure; mobilisation activates the calf muscle pump
- Wound swab for C/ST + antibiotics if signs of infection [6] — only treat clinical infection (cellulitis, purulence, systemic signs), not colonisation
- Ulcer care: debridement of necrotic tissue, appropriate wound dressings, barrier cream for surrounding skin [6]
- Four-layered graduated compression bandage (ABPI > 0.4) [6]
- Treat the underlying varicose veins (intervention if appropriate)
- If non-healing despite adequate treatment: 4-quadrant biopsy and palpate groin LN to exclude Marjolin ulcer (2% — malignant transformation to SCC, rarely BCC) [6]
- Fenestrated split-thickness skin graft — for large or refractory ulcers after the wound bed is adequately prepared [6]
4. Interventional / Surgical Management
Intervention is indicated when there is documented superficial venous reflux (retrograde flow > 0.5 seconds on duplex) [2] AND one or more of:
| Indication | Explanation |
|---|---|
| Symptomatic varicose veins failing conservative therapy | Pain, heaviness, swelling not adequately controlled by stockings |
| Bleeding from varicosities [8] | Telangiectasia, reticular, and varicose veins near bony prominences are prone to haemorrhage |
| Recurrent superficial thrombophlebitis [8] | Veins prone to recurrent thrombosis; intervention reduces thrombosis burden |
| Severe disease (C4 or above) [2] | Skin changes, LDS, atrophie blanche, ulceration — these indicate significant venous hypertension requiring definitive treatment |
| Cosmetic concern (C1–C2) | Patient request for visible vein treatment (usually sclerotherapy) |
| Contraindication | Reason |
|---|---|
| Pregnancy | Risk of DVT during/after procedure; varicose veins often improve post-partum; defer treatment [1][2] |
| Acute superficial or deep vein thrombosis (DVT) | Active thrombus risks embolisation during manipulation; superficial veins may serve as collateral drainage [1] |
| Combined deep AND superficial venous insufficiency | Blood has no alternative route back — ablating the superficial system would leave the patient with no functional outflow → limb would become worse [2] |
| Moderate to severe peripheral artery disease (PAD) | Compression post-procedure would compromise arterial perfusion [1] |
| Congenital venous abnormalities (relative) | Aberrant anatomy increases procedural risk; specialist planning required [1] |
Combined Deep + Superficial Incompetence = Conservative Only
This is the most important contraindication to understand from first principles. If the deep system is incompetent AND you ablate the superficial system, where does the blood go? Nowhere. You've removed the patient's last functional venous outflow pathway. This patient must be managed conservatively. The deep system has limited surgical options — valvular reconstruction has limited efficacy [2].
Endovenous therapy and surgery appear equally effective [1], but there are important differences:
| Factor | Endovenous Treatment | Surgical Treatment |
|---|---|---|
| Anaesthesia | Under local anaesthesia (LA), USG-guided [2] | General or regional anaesthesia |
| Recovery | More rapid recovery [1] | Longer recovery |
| Post-op pain | Less post-operative pain and analgesic use [1] | More pain |
| QOL impairment | Minimal postoperative QOL impairment [1] | Greater initial impairment |
| First-line? | Yes — endovenous treatment usually first line [2] | Second line in most cases |
Surgical treatment is preferred over endovenous if [2]:
- Superficial varicose veins (< 1 cm deep): Risk of skin burns from thermal energy
- Tortuous veins: Endovenous catheter/fibre cannot be passed through tortuous segments
- Chronic/recurrent phlebitis: Adhesions prevent passage of endovenous devices
5. Endovenous Treatment Modalities — In Detail
5.1 Thermal Ablation (Requires Tumescent Anaesthesia)
Tumescent anaesthesia is a key concept for thermal techniques [2]:
- Composition: saline + lignocaine + epinephrine + NaHCO₃ (to reduce stinging) [2]
- Injected around the vein under USG guidance
- Roles [2]:
- Increase maximum dose of lignocaine (dilution effect)
- Facilitate contact of vein wall with the ablation device (compresses the vein)
- Move the vein away from the skin to protect the skin from thermal injury
- Acts as a heat sink to protect surrounding tissues (nerves, skin, subcutaneous fat)
- Preferred treatment modality (but self-paid under HA system in Hong Kong) [1]
- Mechanism: Insertion of a laser fibre into the lumen of the incompetent vein under USG guidance → generation of heat denatures the proteins constituting the vein wall → the vein fibroses shut [1][8]
- Comparison with RFA: Higher success rate than RFA [1]; less expensive than RFA [1]
- Ideal candidates: Straight veins, > 1 cm deep, diameter 5–12 mm
- Complications [1]:
- Skin burns (thermal injury to overlying skin)
- Bruising/ecchymosis
- Superficial thrombophlebitis (reduced with NSAIDs)
- DVT
- Saphenous nerve injury
- Mechanism: Bipolar catheter delivers radiofrequency energy into the vein lumen → controlled thermal ablation → vein fibrosis [1]
- Comparison with EVLA: Faster recovery than EVLA [1]; less post-operative pain and analgesic use than EVLA [1]
- Complications: Same as EVLA — skin burns, bruising, thrombophlebitis, DVT, nerve injury [1]
EVLA vs. RFA — How to Remember
EVLA = Extra Victory (higher success rate, cheaper) but more painful post-op. RFA = Rapid Fast recovery (quicker recovery, less pain) but slightly lower success rate and more expensive. Both are excellent; choice depends on patient preference and local expertise.
5.2 Non-Thermal Ablation (No Tumescent Required)
The major advantage of non-thermal techniques: tumescent anaesthesia is NOT required [2]. This means fewer needles, less discomfort, and no risk of thermal injury to surrounding structures.
- Mechanism: Cyanoacrylate adhesive agent is injected sequentially through a catheter to seal off varicose veins [1]
- Requires compression along the length of the vein from proximal to distal after injection [1][2]
- Major advantage: Non-thermal, non-tumescent technique — less burns and fewer needle injections [1]
- Compression stockings are NOT required postoperatively [1][2] — a significant patient comfort benefit
- Limitations: Risk of vein hyperpigmentation and foreign body reaction; newer technique with less long-term data
Tumescent is a dilute lidocaine mixture injected around the vein to anaesthetise the area and provide a heat-sink so surrounding tissues are not damaged during high-temperature treatment such as ablation [1]
- Mechanism: Combines mechanical damage (rotating wire disrupts the endothelium) + chemical damage (simultaneous sclerosant injection) [2]
- Dual mechanism increases endothelial destruction → more reliable vein closure
- No tumescent required; lower risk of thermal injury
- Risk of vein hyperpigmentation and ulceration (from sclerosant extravasation)
- Mechanism: Irritant agent is injected into the vein, causing endothelial damage by detergent or osmotic action → inflammation → fibrosis → vein obliteration [1][8]
- Can be USG-guided to directly inject sclerosant at the level of refluxing perforators [8]
- Post-operative compression stockings for 2 weeks to appose the inflamed vein walls and prevent thrombus formation [2]
- Types of sclerosing agents [1]:
- Indications: C1 disease (telangiectasia, reticular veins, small varicose veins < 3 mm) [1]; adjunctive treatment of residual tributaries after truncal ablation; patients unfit for other procedures
- Complications [1]: Skin pigmentation, skin necrosis, thrombophlebitis, DVT, allergic reactions
- Improves symptoms but recurrence rate and need for re-intervention is high [1]
6. Surgical Treatment — In Detail
Surgery reduces venous volume in the limbs and thereby the effects of venous hypertension upon the cutaneous tissues [8]. It physically removes or disconnects the incompetent veins.
6.2 Procedures for GSV Incompetence
- Oblique incision in the groin below the inguinal ligament over the femoral artery, extending medially for ~4 cm [1]
- Flush ligation = ligating the GSV very close to its junction with the femoral vein [1][2]
- Why "flush"? If the saphenous vein is ligated too distally from the SFJ, the remaining stump of GSV and all its tributaries will get dilated, forming a saphena varix [1][2] — essentially creating a new reflux source
- All tributaries of the saphenous vein at the SFJ are dissected and ligated individually [1]
- Pass a metal guidewire through the GSV with an olive (bulbous end) → pull out the entire vein in a proximal direction [1][2]
- Stripping is required to decrease the risk of recurrence due to persistent venous reflux via thigh perforators or neovascularisation in the groin [1]
- Critical safety point: Stripping of the GSV is limited to the THIGH ONLY [1]
- Stripping below the knee to ankle does NOT improve symptomatic relief but SIGNIFICANTLY increases the risk of saphenous nerve injury [1]
- Why? Because the saphenous nerve runs in close proximity to the GSV in the distal calf — stripping here would inevitably damage it
- Varicose veins are marked preoperatively with indelible ink [1]
- Multiple small incisions are made directly over branch varicosities [1]
- The vein is elevated from the incision with a small vein hook, divided, and avulsed from surrounding subcutaneous tissues [1]
- Removes the tributary varicosities that won't resolve with truncal ablation alone
| System | Treatment Options | Notes |
|---|---|---|
| Perforators | Sub-fascial endoscopic perforator surgery (SEPS) [2][8]; perforator mapping and ligation; open sub-fascial ligation | SEPS uses small incisions + endoscopic visualisation; CO₂ insufflation of the subfascial space; perforators are clipped and divided. Lower morbidity than open approach [8] |
| Deep venous system | Conservative management; valvular reconstruction (limited efficacy) [2] | Deep system incompetence is very difficult to treat surgically. Options include valve repair, transposition, or transplantation, but results are inconsistent |
- A mechanical alternative to stab avulsion
- Powered mechanical aspirator device inserted adjacent to the target vein after tumescent anaesthesia [8]
- Blade activated → vein aspirated into the device and destroyed [8]
- Advantage: Fewer incisions needed
- Disadvantage: More postoperative pain and haematoma formation [8]
| Complication | Details | Why It Happens |
|---|---|---|
| Haematoma formation [1] | Common after stripping and avulsion | Disruption of venous tributaries and surrounding tissue |
| Wound infection [1] | Groin incisions in the warm, moist inguinal crease | Standard surgical site infection risk |
| Saphenous nerve injury [1][2] | Pain or numbness along medial aspect of calf and medial foot | Runs alongside GSV especially below the knee — why GSV stripping is limited to above-knee only |
| Sural nerve injury [1][2] | Pain or numbness in posterolateral leg and lateral foot | Runs alongside SSV |
| Superficial thrombophlebitis [1] | Inflammation along course of excised veins or residual varicosities. Self-limited; treat with compression stockings and NSAIDs | Endothelial damage and blood stasis in residual vein segments |
| DVT [1] | Complication of venous dissection. Thromboprophylaxis should be given in high-risk individuals [1] | Surgical trauma activates coagulation cascade; venous manipulation promotes Virchow's triad |
| Skin burns (thermal ablation) | Overlying skin damage from EVLA/RFA | Insufficient tumescent, vein too superficial (< 1 cm deep) |
| Skin pigmentation (sclerotherapy/non-thermal) | Hyperpigmentation along treated vein [2] | Sclerosant extravasation, haemosiderin from trapped blood |
| Recurrence (30%) [2] | More common in SSV | Causes: neovascularisation, reflux in residual axial vein, new junctional reflux, inadequate initial surgery [2] |
Setting expectations (crucial for informed consent):
- Surgery will NOT alter existing skin changes [2] — pigmentation, LDS, and atrophie blanche are permanent tissue damage. Treatment prevents progression but does not reverse it
- May not improve all symptoms (e.g., pain may have other causes) [2]
- Recurrence rate is ~30% — this is high, and patients must understand this is a chronic condition [2]
Pre-operative points:
- Antiplatelet/anticoagulant medications can be continued [2] — no need to stop aspirin or warfarin in most cases (unlike arterial surgery)
- Mark varicosities with indelible ink while standing (they collapse when supine)
Post-operative care [2]:
- Early ambulation — prevents DVT and promotes healing
- Follow-up Doppler USG 2–3 days post-op — to check for DVT and treatment success
- Compression stockings × 4 weeks — maintains compression while treated veins fibrose
- No driving × 1 week
- Normal to have pain and pulling tightness along the treated vein
- Consult if: excessive pain with swelling (suspect DVT) or numbness/discolouration of toes (tight stocking)
Since varicose vein surgery involves manipulation of venous structures, DVT prophylaxis is important:
- Mechanical prophylaxis: Intra-operative sequential compression devices (SCD); post-op early mobilisation + elastic compression stockings [9]
- Pharmacological prophylaxis (LMWH): Not routinely given to all patients in HK; indicated for patients with history of VTE, congenital thrombophilias, Caucasians [9]
- Established DVT pre-op: IVC filter to prevent PE → remove 2 weeks later [9]
| Modality | Mechanism | Best For | Key Advantages | Key Disadvantages |
|---|---|---|---|---|
| Compression stockings | External compression reduces venous diameter, augments calf pump | All CEAP classes; mainstay of conservative Mx | Non-invasive, symptom relief | Poor compliance, no disease modification, C/I if ABPI < 0.4 |
| Foam sclerotherapy | Chemical endothelial destruction | C1, small C2 (< 3 mm), residual tributaries | Office-based, cheap, minimally invasive | High recurrence, pigmentation, allergic reactions |
| EVLA | Thermal protein denaturation | Truncal incompetence (GSV/SSV) | Higher success rate, preferred modality | Needs tumescent, risk of burns, more painful than RFA |
| RFA | Radiofrequency thermal ablation | Truncal incompetence | Faster recovery, less pain than EVLA | Slightly lower success rate, more expensive |
| VenaSeal / Cyanoacrylate glue | Adhesive vein sealing | Truncal incompetence | Non-thermal, no tumescent, no post-op stockings | Newer, less long-term data, foreign body reaction |
| MOCA | Mechanical + chemical | Truncal incompetence | No tumescent, dual mechanism | Risk of pigmentation, ulceration |
| Trendelenburg + stripping | SFJ flush ligation + vein removal | GSV incompetence, tortuous/superficial veins | Definitive, long track record | GA required, longer recovery, nerve injury risk |
| SEPS | Endoscopic perforator division | Perforator incompetence, venous ulcers | Lower morbidity than open ligation | Technically demanding |
High Yield Summary
Treatment principles: Reduce venous hypertension → improve tissue O₂, decrease inflammation, decrease oedema.
Conservative (for ALL patients): Risk factor modification (avoid standing, weight loss, exercise), graduated compression stockings (at least 20 mmHg at ankle, C/I if ABPI < 0.4), venotonics (Daflon for oedema C3+).
Intervention indications: Documented superficial reflux (> 0.5 s on duplex) with symptoms, complications (C4+), bleeding, or recurrent phlebitis.
Contraindications: Pregnancy, acute DVT, combined deep + superficial incompetence (blood has no route back), severe PAD.
Endovenous treatment is first line: EVLA (preferred — higher success) or RFA (faster recovery, less pain). Both need tumescent anaesthesia. VenaSeal (non-thermal, no tumescent, no post-op stockings) is a newer alternative.
Surgery preferred if: veins superficial (< 1 cm deep), tortuous, or adhesions from recurrent phlebitis.
GSV surgery: Trendelenburg operation (SFJ flush ligation) + above-knee stripping + stab avulsion. Do NOT strip below knee (saphenous nerve injury).
SSV surgery: SPJ ligation + stripping (risk of sural nerve injury).
Venous ulcer management: 4-layer compression bandage (ABPI > 0.4), wound care, treat VV. 50–70% heal in 3 months. Non-healing → biopsy for Marjolin (2% SCC).
Surgery will NOT reverse skin changes — it prevents progression only. Recurrence rate ~30%.
Post-op: Early ambulation, compression stockings × 4 weeks, FU duplex 2–3 days, no driving × 1 week.
Active Recall - Management of CVI and Varicose Veins
References
[1] Senior notes: felixlai.md (Chapter 13: Vascular System — Varicose Veins, pp. 957–961) [2] Senior notes: maxim.md (Section 7.3: Chronic Venous Insufficiency — Management, pp. 173–175) [6] Senior notes: maxim.md (Section 7.4: Lower extremity ulcers — Management of venous ulcers, pp. 174–175) [8] Senior notes: felixlai.md (Chapter 13: Vascular System — Chronic Venous Disease Treatment, pp. 947–949) [9] Senior notes: maxim.md (DVT prophylaxis section)
Complications of CVI and Varicose Veins
Complications can be divided into two broad categories: complications of the disease itself (what happens if CVI/varicose veins are left untreated or inadequately treated) and complications of treatment (iatrogenic). Let me walk through both systematically, explaining the pathophysiology behind each.
1. Complications of the Disease
These complications represent the natural history of progressive venous hypertension — each is a step further along the CEAP spectrum. Understanding them as a continuum rather than isolated events is key.
- What it is: Pruritic, scaling skin with erosions and crusting, typically around the gaiter area [1][8]
- Pathophysiology: Venous hypertension → capillary distension → leakage of plasma proteins and inflammatory mediators into the dermis → chronic inflammatory response → eczematous change. The leaked fibrinogen polymerises into pericapillary fibrin cuffs, which trap growth factors and impair tissue repair, perpetuating inflammation.
- Why it matters: Itching leads to scratching → excoriation → breaks in skin barrier → portal of entry for bacteria → secondary infection (cellulitis). The eczema itself also indicates the skin is already compromised and at risk of ulceration.
- Management: Emollients, topical corticosteroids (short courses for flares), compression therapy to address the underlying venous hypertension. Avoid known contact allergens (many patients develop sensitivity to dressings, topical antibiotics like neomycin, or lanolin).
Contact Dermatitis Trap
Patients with venous eczema are at high risk of developing contact dermatitis to topical preparations — including wound dressings, adhesive tape, and topical antibiotics. If eczema worsens despite treatment, suspect a superimposed allergic contact dermatitis and consider patch testing. Don't just apply more creams.
- What it is: Brown discolouration of the gaiter area skin [1][8]
- Pathophysiology: Venous hypertension → capillary distension → extravasation of red blood cells into the dermis → macrophages phagocytose and break down the RBCs → haemosiderin deposition (an iron-rich pigment from haemoglobin degradation) [1][8]
- Clinical significance: Haemosiderin staining is permanent — surgery will NOT alter existing skin changes [2]. This is a crucial counselling point. Treatment prevents further pigmentation but cannot reverse what is already there.
- Distribution: Commonly occurs in gaiter area (medial lower 1/3 of the leg) [1][8]. In severe cases, pigmentation may cover the entire lower limb [3]
- What it is: Fibrosing panniculitis of subcutaneous tissue due to chronic venous insufficiency [1][8]
- Clinical features: Hyperpigmentation + subcutaneous induration + redness + tenderness + pitting oedema [1][8]
- Pathophysiology: Chronic venous hypertension → sustained capillary leak → fibrinogen leak → pericapillary fibrin deposition → impaired O₂/nutrient diffusion → tissue hypoxia → chronic inflammation with release of TGF-β and other fibrogenic cytokines → progressive replacement of skin and subcutaneous fat by fibrous tissue [1][8]
- Consequences:
- Classic "inverted champagne bottle" leg — the lower leg becomes narrowed and hardened while the calf above remains relatively normal
- Fixed flexion contracture of the ankle joint — subcutaneous fibrosis and/or painful ulceration restricts ankle range of motion [3]. This creates a vicious cycle: reduced ankle mobility → impaired calf muscle pump → worsening venous hypertension
- Acute LDS: Painful, hot, red, and tender on the medial side of the gaiter area. Often misdiagnosed as cellulitis or acute thrombophlebitis [3]. The distinction matters because acute LDS does not respond to antibiotics.
- What it is: Ivory-white avascular fibrotic scars with hyperpigmented borders and telangiectasia [1][8]
- Pathophysiology: End-stage microvascular damage — the dermal capillaries have been obliterated by the chronic inflammatory process, leaving areas of avascular scar tissue. The surrounding hyperpigmented border represents the still-active zone of haemosiderin deposition.
- Clinical significance: Prone to secondary venous ulceration due to poor blood supply [1][8] — these avascular white areas have minimal capacity for repair, so even minor trauma can trigger ulceration that heals poorly.
This is the most clinically significant complication and the one that generates the greatest healthcare burden.
- Location: At the medial gaiter area — the site of medial calf perforators (Cockett perforators) [2]
- Characteristics: Shallow, gently sloping edges, with slough or granulation tissue at the base
- Pain: Usually painless unless infected (commonly S. aureus) [2]. However, acute venous ulcers in the context of active tissue sloughing can be very painful [3]
- Pathophysiology: The culmination of the entire venous hypertension cascade — tissue hypoxia from fibrin cuffs + white cell trapping + growth factor sequestration → skin breakdown → full-thickness skin loss (C6 = active; C5 = healed)
- Infection: Chronic venous ulcers are typically colonised by bacteria (this is expected and does not necessarily require antibiotics). Clinical infection — characterised by expanding cellulitis, purulent discharge, increased pain, or systemic features — requires wound swab for C/ST and appropriate antibiotics [6]
- Healing: With adequate conservative management (4-layer compression bandaging, wound care, leg elevation), 50–70% of venous ulcers heal within 3 months [6]
- Recurrence: High recurrence rate if the underlying venous pathology is not treated. Treating the varicose veins reduces ulcer recurrence.
- What it is: Malignant transformation of a chronic venous ulcer, usually to squamous cell carcinoma (SCC), rarely basal cell carcinoma (BCC) [2][6]
- Incidence: ~2% of long-standing venous ulcers [2]
- Why it happens: Chronic ulcers create a microenvironment of persistent inflammation, repeated tissue destruction and regeneration, and impaired immune surveillance — this promotes accumulation of genetic mutations in keratinocytes over years to decades, eventually leading to malignant transformation. This is conceptually similar to how chronic inflammation anywhere in the body increases cancer risk (e.g., Barrett's → oesophageal adenocarcinoma, ulcerative colitis → colorectal cancer).
- When to suspect: A chronic ulcer that changes character — becomes raised, develops everted or rolled edges, bleeds easily, grows rapidly, or fails to heal despite months of adequate therapy
- Investigation: 4-quadrant biopsy of the ulcer edge and palpation of groin lymph nodes for metastasis [6]
- Management: Wide local excision ± lymph node dissection depending on staging
Marjolin's Ulcer — Don't Miss It
Any venous ulcer that has been present for years and suddenly changes character (raised edges, easy bleeding, failure to heal) demands a biopsy. The 2% transformation rate sounds low but is clinically significant given how common venous ulcers are. A 4-quadrant biopsy from the ulcer edge (not the base — the base is necrotic/granulation tissue) is the standard approach.
- Bleeding from attenuated vein clusters [1] — varicose veins near the surface, especially over bony prominences (medial malleolus), can rupture with minimal trauma
- Pathophysiology: The vein wall is already weakened (decreased elastin, increased MMPs). As the vein dilates and becomes more superficial, the overlying skin thins (atrophic changes from CVI). A minor knock can rupture both the skin and the vein.
- Clinical picture: Can be dramatic — venous bleeding from a varicose vein can produce surprisingly large volumes of blood, causing alarm in patients. However, it is low-pressure venous bleeding and is readily controlled.
- Management: Elevation and direct pressure. Lay the patient down, elevate the leg above heart level, and apply firm pressure with a pad. This simple manoeuvre controls virtually all varicose vein bleeds. Once controlled, the underlying vein should be treated to prevent recurrence.
Emergency Varicose Vein Bleeding
Patients sometimes present to ED in a panic with blood-soaked clothing. The key is: lie them down, elevate the leg, apply direct pressure. Venous bleeding (low pressure) is almost always controlled this way. Do NOT apply a tourniquet — it will worsen venous congestion and increase bleeding. Refer for definitive treatment of the varicose vein.
- What it is: Thrombosis and inflammation within a superficial varicose vein [1]
- Clinical features: Localised pain, redness, warmth, and a tender, palpable, cord-like vein
- Pathophysiology: Venous stasis within a dilated, incompetent varicose vein → activation of coagulation cascade (Virchow's triad: stasis + endothelial damage from chronic distension + hypercoagulable microenvironment) → thrombus formation → inflammatory response
- Risk: Superficial thrombophlebitis can propagate into the deep venous system via the SFJ or SPJ, or via perforator veins. If the thrombus extends to within 3 cm of the SFJ, there is a real risk of DVT and PE. Always assess with duplex USG.
- Management: Usually self-limited — compression stockings, NSAIDs for pain and inflammation. If extensive or proximal, consider anticoagulation.
- Patients with varicose veins have an increased risk of DVT — the chronic venous stasis and endothelial dysfunction create a prothrombotic environment
- DVT can also be a cause of secondary CVI (post-thrombotic syndrome), creating a bidirectional relationship
- Complication of DVT → chronic venous insufficiency and pulmonary embolism [10]
- Post-thrombotic syndrome: DVT damages venous valves → permanent valvular incompetence → secondary CVI → further venous hypertension. This is why DVT prophylaxis and early treatment of DVT are so important.
- In advanced CVI, chronic inflammation and fibrosis can damage lymphatic vessels running alongside the veins
- This adds a lymphatic component to the venous oedema, creating phlebo-lymphoedema — harder to treat because lymphatic damage is largely irreversible
- The skin may develop features of both CVI (pigmentation, eczema) and lymphoedema (thickening, warty changes)
- Subcutaneous fibrosis from chronic lipodermatosclerosis and/or painful ulceration may cause a fixed flexion contracture of the ankle joint [3]
- This impairs the calf muscle pump mechanism (which requires full ankle dorsiflexion to function efficiently) → worsening venous hypertension → a self-perpetuating vicious cycle
- Physiotherapy and early treatment of LDS can help prevent this debilitating complication
2. Complications of Treatment
| Complication | Mechanism | Management |
|---|---|---|
| Pain | Expected post-procedure — tissue inflammation, nerve irritation | Analgesia; normal to have pain and pulling tightness of the treated vein [2] |
| Bruising / ecchymosis | Disruption of venous tributaries; haematoma in the stripping tract | Self-limiting; compression helps |
| Haematoma formation [1] | Blood accumulates in the surgical bed after ligation/stripping | Evacuation if large; compression; usually resolves |
| Wound infection [1] | Especially groin incisions (warm, moist environment) | Antibiotics; wound care |
This is one of the most important specific complications to know for exams:
| Nerve | At Risk During | Territory | Clinical Presentation |
|---|---|---|---|
| Saphenous nerve | GSV stripping — especially below the knee (close proximity of nerve and vein in distal calf) [1] | Sensory to medial leg and medial foot [2] | Pain or numbness along medial aspect of calf [1] |
| Sural nerve | SSV stripping [1] | Sensory to posterolateral leg and lateral foot [2] | Pain or numbness in posterolateral leg and lateral foot [1] |
- This is precisely why GSV stripping is limited to the thigh only — extending below the knee significantly increases saphenous nerve injury risk without improving symptomatic relief [1]
- Both nerves are purely sensory, so the deficit is numbness/paraesthesia rather than motor weakness
- Occurs along the course of excised veins or in residual varicosities [1]
- Caused by endothelial damage and blood stasis in residual vein segments after treatment
- Self-limited and treated conservatively with compression stockings [1]
- NSAIDs reduce the incidence and severity (particularly after thermal ablation) [1]
- Complication of dissection/manipulation of venous structures [1]
- Risk is inherent because you are operating within the venous system — thermal energy, mechanical disruption, and blood stasis all activate coagulation
- Thromboprophylaxis should be given in high-risk individuals [1] — those with prior VTE, thrombophilia, malignancy, obesity, immobility
- Detection: Post-operative duplex USG at 2–3 days can screen for early DVT [2]
- Suspect if: Excessive pain with swelling post-operatively → urgent duplex
- Specific to EVLA and RFA
- Occurs when the vein being treated is too superficial (< 1 cm from the skin surface) or when tumescent anaesthesia is inadequately placed — the thermal energy conducts through to the skin
- This is why surgical treatment is preferred over endovenous treatment for superficial veins (< 1 cm deep) [2]
- Prevention: Adequate tumescent anaesthesia (acts as a heat sink and pushes the vein deeper)
- Hyperpigmentation along the treated vein — from haemosiderin deposition after sclerosant-induced vein damage and trapped blood
- Also occurs with non-thermal methods (MOCA, cyanoacrylate) due to extravasation of sclerosant or inflammatory reaction [2]
- Usually fades over months but can be permanent in some cases
- Rare but possible reaction to sclerosant agents (especially STS)
- Can range from minor skin rash to anaphylaxis
- Always have resuscitation equipment available when performing sclerotherapy
This is arguably the most important long-term complication:
- Recurrence rate is approximately 30% [2]
- More common in SSV than GSV territory [2]
- Causes of recurrence [2]:
- Neovascularisation — new small veins grow across the ligated junction (especially at the groin), re-establishing reflux. This is a biological response to surgical disruption.
- Reflux in residual axial vein — incomplete treatment of the trunk saphenous vein
- New junctional reflux — development of reflux at a previously competent junction
- Inadequate initial surgery — failure to identify and treat all sources of reflux (e.g., missed perforator incompetence, untreated tributary)
- Management of recurrent varicose veins: Repeat duplex USG to map the recurrence → tailored re-intervention (usually endovenous or sclerotherapy rather than redo surgery, as adhesions from prior surgery make dissection difficult)
Even conservative management has complications worth knowing:
| Complication | Mechanism | Prevention |
|---|---|---|
| Pressure necrosis | Excessive pressure over bony prominences or incorrect application | Proper fitting, patient education, adequate padding |
| Contact dermatitis | Skin sensitivity to stocking material | Hypoallergenic stockings, skin care |
| Fungal infection | Warm, moist environment under the stocking | Good foot hygiene, antifungal powder |
| Tourniquet effect | Stocking rolls down and creates a circumferential constriction band | Proper length selection, patient education |
| Tissue ischaemia (if applied without ABPI check) | Compression on an ischaemic limb further reduces perfusion pressure | Always check ABPI before compression — absolute C/I if < 0.4 [2] |
High Yield Summary
Disease complications follow the CEAP progression and are driven by sustained venous hypertension:
- C4a: Hyperpigmentation (haemosiderin from extravasated RBCs — permanent), venous eczema (inflammatory response to leaked proteins — risk of contact dermatitis)
- C4b: Lipodermatosclerosis (fibrosing panniculitis — "inverted champagne bottle" leg; acute LDS mimics cellulitis), atrophie blanche (avascular white scars prone to ulceration)
- C5/C6: Venous ulceration (gaiter area, painless unless infected with S. aureus; 50–70% heal with compression in 3 months)
- Marjolin's ulcer: SCC transformation in 2% of long-standing ulcers → 4-quadrant biopsy
- Bleeding: Controlled by elevation + direct pressure
- Superficial thrombophlebitis: Can propagate into deep system → DVT/PE
- Ankle contracture: From LDS fibrosis → impairs calf pump → vicious cycle
Treatment complications:
- Nerve injury: Saphenous nerve (GSV, especially below knee → medial calf numbness); sural nerve (SSV → posterolateral leg/lateral foot numbness)
- DVT: Thromboprophylaxis in high-risk patients; post-op duplex at 2–3 days
- Skin burns: Thermal ablation on superficial veins (< 1 cm deep) — use surgery instead
- Recurrence (~30%): Neovascularisation, incomplete treatment, residual reflux. More common in SSV.
- Surgery will NOT reverse existing skin changes — only prevents progression.
Active Recall - Complications of CVI and Varicose Veins
References
[1] Senior notes: felixlai.md (Chapter 13: Vascular System — Varicose Veins, pp. 953–961) [2] Senior notes: maxim.md (Section 7.3: Chronic Venous Insufficiency — Management and Complications, pp. 173–175) [3] Senior notes: maxim.md (Section 7.3: CVI clinical images and descriptions, p. 173) [6] Senior notes: maxim.md (Section 7.4: Lower extremity ulcers — Management of venous ulcers, pp. 174–175) [8] Senior notes: felixlai.md (Chapter 13: Vascular System — Chronic Venous Disease, pp. 944–949) [10] Senior notes: felixlai.md (DVT — Prognosis/Complications, p. 970)
High Yield Summary
Definition: Varicose veins = dilated, tortuous subcutaneous veins ≥ 3 mm with demonstrable reflux. CVI = oedema, skin changes, or ulceration from chronic venous dysfunction (CEAP C3–C6).
Core pathophysiology: Venous valve incompetence → reflux → sustained venous hypertension → capillary distension → leakage of RBCs, fluid, proteins → haemosiderin deposition, fibrin cuffs, WBC trapping → inflammation, tissue hypoxia → skin changes, fibrosis, and ulceration.
CEAP: C0 (no signs) → C1 (telangiectasia/reticular veins) → C2 (varicose veins) → C3 (oedema) → C4a (pigmentation/eczema) → C4b (LDS/atrophie blanche) → C4c (corona phlebectatica) → C5 (healed ulcer) → C6 (active ulcer). Plus E (aetiology), A (anatomy), P (pathophysiology).
Anatomy: GSV runs medially (SFJ at groin, saphenous nerve companion). SSV runs posteriorly in calf (SPJ at popliteal fossa, sural nerve companion). Perforators (Hunterian → Dodd → Boyd → Cockett → May) connect superficial to deep.
Risk factors: Female, age, obesity, family history, prolonged standing, pregnancy, previous DVT, increased abdominal pressure.
Primary (idiopathic, intrinsic wall weakness) vs. Secondary (DVT → post-thrombotic syndrome is the most important secondary cause).
Clinical features: Cosmetic concern, aching (worse standing, better elevation), heaviness, ankle swelling, night cramps, itching → skin changes (corona phlebectatica, pigmentation, eczema, LDS, atrophie blanche) → ulceration (medial gaiter area, painless unless infected).
Must check ABPI before compression — absolute CI if < 0.4.
Venous ulcer: Shallow, sloping edge, gaiter area, painless, haemosiderin-stained surrounding skin, pulses present.
Acute LDS mimics cellulitis — don't be fooled.
Marjolin's ulcer (SCC transformation) in 2% of long-standing venous ulcers.
High Yield Summary
Core differential for lower limb oedema: CVI, DVT, lymphoedema, cardiac failure, hypoalbuminaemia, lipodema, drug-induced (CCBs), dependency oedema. Use unilateral vs. bilateral and pitting vs. non-pitting to narrow it down.
Core differential for lower limb ulcer: Venous (gaiter area, shallow, painless, sloping edge), arterial (toes/heel, deep, punched-out, painful, absent pulses), neuropathic (plantar, painless, punched-out), pressure (bony prominences), malignant/Marjolin (2% of chronic venous ulcers → SCC).
Must-exclude diagnoses: DVT (before attributing swelling to CVI), PAD (before applying compression — check ABPI), Marjolin ulcer (4-quadrant biopsy for any non-healing chronic ulcer).
Acute LDS mimics cellulitis — medial lower leg, painful, hot, red, tender but in context of CVI and does NOT respond to antibiotics.
Lateral thigh varicosities → think Klippel-Trénaunay (congenital: VV + port wine stain + limb hypertrophy).
Saphena varix DDx: femoral hernia, inguinal lymphadenopathy, femoral artery aneurysm, psoas abscess.
Lymphoedema vs. CVI: Lymphoedema affects dorsum of foot, Stemmer sign positive, non-pitting in late stages, warty/thickened skin. CVI affects gaiter area, pitting, haemosiderin pigmentation.
High Yield Summary
Diagnosis of varicose veins requires visible dilated tortuous veins ≥ 3 mm in upright position PLUS demonstrable reflux (valve closure time > 0.5 s on duplex USG).
CEAP is the diagnostic framework: C = clinical inspection; E, A, P = require duplex USG to complete.
Duplex USG is the gold standard — it answers: Is there reflux? Where? Is the deep system competent? Is there DVT? Is the vein suitable for endovenous treatment?
ABPI is mandatory before compression — absolute contraindication if ABPI < 0.4. In diabetics with calcified arteries (ABPI > 1.3), use toe pressures instead.
Tourniquet test: No refilling below tourniquet = incompetence at tourniquet level. Rapid refilling despite tourniquet = incompetence below that level. Largely replaced by duplex but still examined.
Perthes' test assesses deep venous patency: tourniquet at SFJ + walking. If deep system is occluded → pain and swelling (superficial veins are the only outflow — do NOT ablate them).
DVT is a contraindication to varicose vein surgery — must always be excluded by duplex before any intervention.
Combined deep + superficial incompetence → conservative management only (surgery on superficial system would remove the patient's only functional outflow pathway).
Non-healing venous ulcer → 4-quadrant biopsy to exclude Marjolin's ulcer (SCC, 2%).
High Yield Summary
Treatment principles: Reduce venous hypertension → improve tissue O₂, decrease inflammation, decrease oedema.
Conservative (for ALL patients): Risk factor modification (avoid standing, weight loss, exercise), graduated compression stockings (at least 20 mmHg at ankle, C/I if ABPI < 0.4), venotonics (Daflon for oedema C3+).
Intervention indications: Documented superficial reflux (> 0.5 s on duplex) with symptoms, complications (C4+), bleeding, or recurrent phlebitis.
Contraindications: Pregnancy, acute DVT, combined deep + superficial incompetence (blood has no route back), severe PAD.
Endovenous treatment is first line: EVLA (preferred — higher success) or RFA (faster recovery, less pain). Both need tumescent anaesthesia. VenaSeal (non-thermal, no tumescent, no post-op stockings) is a newer alternative.
Surgery preferred if: veins superficial (< 1 cm deep), tortuous, or adhesions from recurrent phlebitis.
GSV surgery: Trendelenburg operation (SFJ flush ligation) + above-knee stripping + stab avulsion. Do NOT strip below knee (saphenous nerve injury).
SSV surgery: SPJ ligation + stripping (risk of sural nerve injury).
Venous ulcer management: 4-layer compression bandage (ABPI > 0.4), wound care, treat VV. 50–70% heal in 3 months. Non-healing → biopsy for Marjolin (2% SCC).
Surgery will NOT reverse skin changes — it prevents progression only. Recurrence rate ~30%.
Post-op: Early ambulation, compression stockings × 4 weeks, FU duplex 2–3 days, no driving × 1 week.
High Yield Summary
Disease complications follow the CEAP progression and are driven by sustained venous hypertension:
- C4a: Hyperpigmentation (haemosiderin from extravasated RBCs — permanent), venous eczema (inflammatory response to leaked proteins — risk of contact dermatitis)
- C4b: Lipodermatosclerosis (fibrosing panniculitis — "inverted champagne bottle" leg; acute LDS mimics cellulitis), atrophie blanche (avascular white scars prone to ulceration)
- C4c: Corona phlebectatica (malleolar flare) — fan-shaped ankle veins signalling advanced venous disease
- C5/C6: Venous ulceration (gaiter area, painless unless infected with S. aureus; 50–70% heal with compression in 3 months)
- Marjolin's ulcer: SCC transformation in 2% of long-standing ulcers → 4-quadrant biopsy
- Bleeding: Controlled by elevation + direct pressure
- Superficial thrombophlebitis: Can propagate into deep system → DVT/PE
- Ankle contracture: From LDS fibrosis → impairs calf pump → vicious cycle
Treatment complications:
- Nerve injury: Saphenous nerve (GSV, especially below knee → medial calf numbness); sural nerve (SSV → posterolateral leg/lateral foot numbness)
- DVT: Thromboprophylaxis in high-risk patients; post-op duplex at 2–3 days
- Skin burns: Thermal ablation on superficial veins (< 1 cm deep) — use surgery instead
- Recurrence (~30%): Neovascularisation, incomplete treatment, residual reflux. More common in SSV.
- Surgery will NOT reverse existing skin changes — only prevents progression.
Chronic Arterial Insufficiency
Chronic arterial insufficiency is a progressive narrowing or occlusion of the arterial lumen, most commonly due to atherosclerosis, resulting in inadequate blood flow to the distal tissues and manifesting as intermittent claudication, rest pain, and eventual tissue loss.
Venous Thromboembolism
Venous thromboembolism is a condition encompassing deep vein thrombosis and pulmonary embolism, caused by pathological blood clot formation within the venous system that can obstruct blood flow and impair cardiopulmonary function.