Diverticular Disease
Diverticular disease refers to the formation of abnormal mucosal outpouchings (diverticula) through the colonic wall, predominantly at sites of vascular penetration, encompassing a spectrum from asymptomatic diverticulosis to symptomatic diverticular disease and acute diverticulitis with potential complications such as perforation, abscess, or fistula formation.
1. Definition and Terminology
Let's start by getting the language right — this is a topic where imprecise terminology costs marks.
- Diverticulum (Latin: diverticulum = "a wayside shelter" or "turning aside") — a sac-like protrusion (outpouching) of a hollow viscus [1][2][3]
- Diverticulosis (coli) — the presence of multiple diverticula, which may be symptomatic or asymptomatic [2][3]
- Diverticular disease — clinically significant and symptomatic diverticulosis [2][3]. This umbrella term encompasses:
- Diverticulitis — inflammation of a diverticulum (caused by microperforation) [1][3]
- Acute vs. Chronic
- Uncomplicated vs. Complicated (abscess, fistula, bowel obstruction, perforation)
- Diverticular bleeding — painless massive PR bleeding due to rupture of vasa recta draped over the diverticular dome [2][3]
- Typically occurs in the ABSENCE of diverticulitis (the bleeding and inflammation are separate pathological processes)
- Self-limited in ~80% of patients
- Segmental Colitis Associated with Diverticula (SCAD) / Diverticular colitis — inflammation of the interdiverticular mucosa without involvement of diverticular orifices (resembles IBD histologically but is a distinct entity) [3]
- Symptomatic Uncomplicated Diverticular Disease (SUDD) — persistent abdominal pain attributed to diverticula without macroscopically overt colitis or diverticulitis; CT shows wall thickening without inflammatory changes [3]
- Diverticulitis — inflammation of a diverticulum (caused by microperforation) [1][3]
| Feature | True Diverticulum | False (Pseudo) Diverticulum |
|---|---|---|
| Layers involved | All layers of the intestinal wall (mucosa, submucosa, muscularis propria, serosa/adventitia) | Only mucosa and submucosa herniate through muscularis propria |
| Example | Right-sided colonic diverticula, Meckel's diverticulum | Left-sided colonic diverticula (the vast majority of "diverticular disease"), Zenker's diverticulum |
| Mechanism | Usually congenital | Usually acquired (pulsion type — pushed out by intraluminal pressure) |
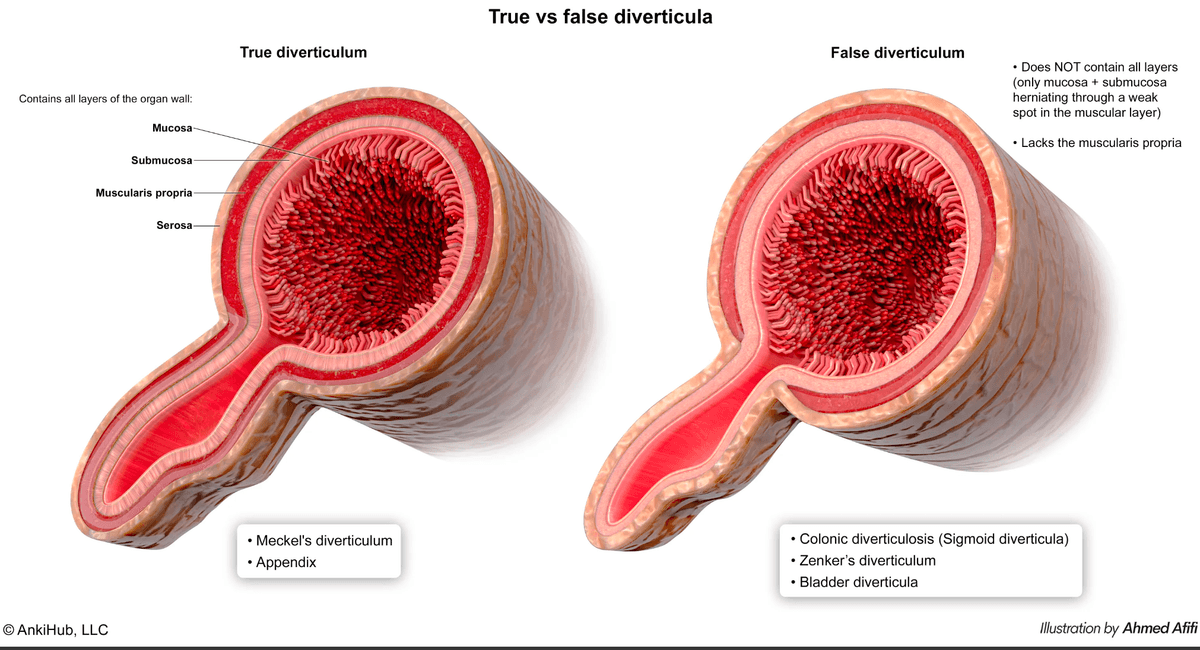
Right-sided diverticula are true diverticula (congenital); left-sided diverticula are false diverticula (acquired) [1]
- Meckel's diverticulum — true diverticulum arising from incomplete obliteration of the vitelline (omphalomesenteric) duct on the antimesenteric surface of the mid-to-distal ileum. Remember the "Rule of 2s": 2% prevalence, 2 feet from ileocaecal valve, 2 inches long, 2 types of ectopic tissue (gastric and pancreatic), presents by age 2 [3]
- Zenker's diverticulum — false diverticulum arising from Killian's triangle (area of weakness between the transverse fibres of the cricopharyngeus and the oblique fibres of the lower inferior constrictor muscle of the pharynx) [3]
Diverticular disease is common in the Western population [1][4]:
- Prevalence increases dramatically with age:
- Mean age of diagnosis of acute diverticulitis = 63 years [3]
- Symptomatic in about 20% of those with diverticulosis [1]
- Of those who develop diverticulitis, ~15-25% will develop complications
Regional Variation — This Is High Yield
| Feature | Western | Asian (including Hong Kong) |
|---|---|---|
| Predominant site | Left-sided (sigmoid colon) | Still predominantly left-sided, BUT the proportion of right-sided diverticulosis (caecum/ascending colon) is significantly higher [1][3][4] |
| Type | False (acquired) | Right-sided = True (congenital); Left-sided = False (acquired) |
| Clinical pitfall | Classic LLQ pain | Caecal diverticulitis mimicking appendicitis — Role of CT scan to differentiate [1] |
Hong Kong Context — Must Know
Understanding risk factors requires understanding the pathophysiology — it's all about wall weakness + increased intraluminal pressure.
| Risk Factor | Mechanism |
|---|---|
| Age (rare before 30) | Progressive degeneration of colonic wall connective tissue; reduced elastin and collagen cross-linking → weaker wall |
| Low-fibre diet | Low residue → smaller, harder stools → colon must generate higher intraluminal pressures to propel contents → pulsion diverticula [1][3] |
| Obesity | Increases intra-abdominal pressure; adipose tissue produces pro-inflammatory cytokines → increases risk of both diverticulitis and diverticular bleeding [3] |
| Fat and red meat intake | Alters gut microbiome, promotes intestinal inflammation [3] |
| Decreased physical activity / sedentary lifestyle | Reduces colonic motility → increased transit time → harder stools → higher pressures [3] |
| Constipation | Increased intraluminal pressure directly [4] |
| Smoking | Impairs mucosal blood flow and tissue healing; alters gut motility |
| NSAIDs | Disrupt mucosal barrier (inhibit prostaglandin synthesis → reduced mucosal blood flow, mucus and bicarbonate secretion) → promotes microperforation and bleeding [1][3][4] |
| Steroids | Immunosuppression impairs inflammatory response and healing; masks symptoms → delayed presentation |
| Opiates | Slow colonic transit → increased intraluminal pressure; constipation |
| Connective tissue diseases (Marfan syndrome, Ehlers-Danlos) | Inherent structural weakness of connective tissue in the colonic wall [4] |
Drugs to Remember
NSAIDs, steroids, and opiates — these three drug classes all worsen diverticular disease. NSAIDs increase bleeding and perforation risk; steroids mask inflammation and delay healing; opiates increase pressure through constipation. Tell patients with known diverticulosis to avoid NSAIDs and stimulant laxatives [4].
4. Anatomy and Function
To understand diverticular disease, you need to understand colonic wall anatomy and the concept of points of weakness.
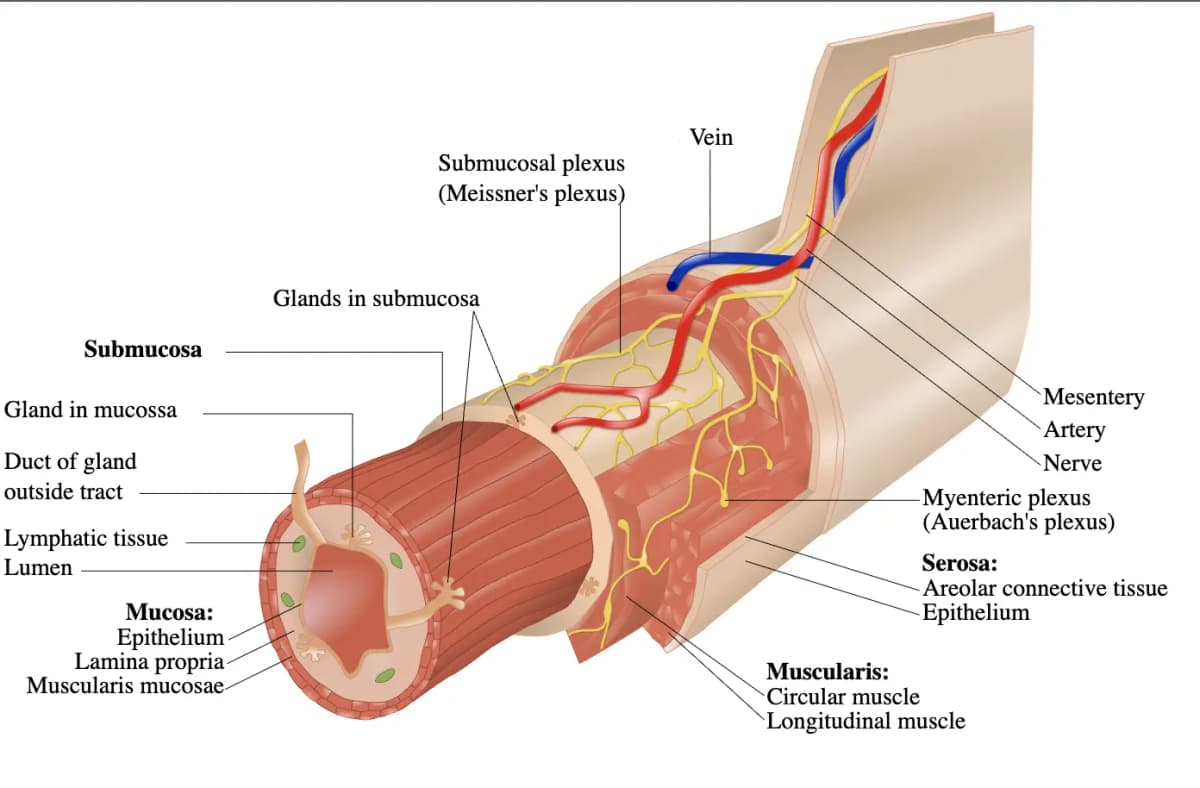
The colon has a unique muscular arrangement compared to the small bowel:
- Inner circular muscle layer — complete ring of smooth muscle
- Outer longitudinal muscle layer — NOT a complete layer; instead condensed into three longitudinal bands called taeniae coli (taenia mesocolica, taenia omentalis, taenia libera)
- Between the taeniae, the outer longitudinal muscle is either very thin or essentially absent → the intertaenial areas are inherently weak
Diverticula develop at well-defined points of weakness where the vasa recta (nutrient arteries) penetrate the circular muscle layer [1][2][3][4]:
- The vasa recta are small arteries that arise from the marginal artery, travel along the mesenteric side, and penetrate through the circular muscle to reach the submucosa and mucosa
- Where each vas rectum pierces the muscle, it creates a gap in the muscularis → a point of structural weakness
- Under increased intraluminal pressure, the mucosa and submucosa herniate through these gaps → forming false (pulsion) diverticula
Outpouchings of the bowel wall occur at the weakest point where vasa recta penetrate circular muscle [1][2]
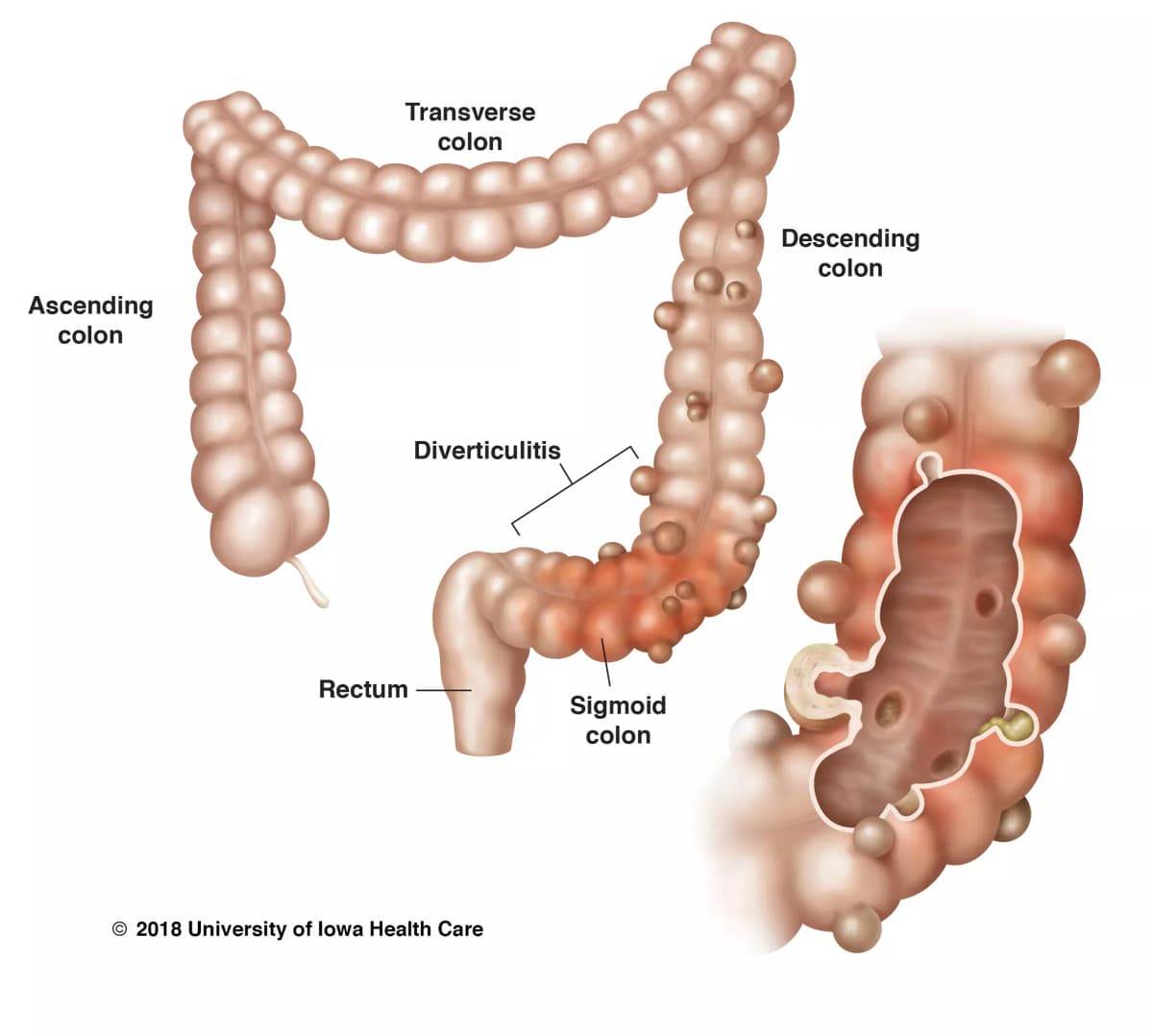
The sigmoid colon is the commonest site [1] because:
- Laplace's Law: Wall tension = (Pressure × Radius) / (2 × Wall thickness). The sigmoid has the narrowest calibre (smallest radius) of any colonic segment → for a given wall tension, it must generate the highest intraluminal pressure to propel contents [1][4]
- The sigmoid acts as a "high-pressure zone" especially during segmental non-propulsive contractions
- Stool is most solid in the sigmoid (water reabsorption is largely complete) → harder to propel → more pressure needed
The rectum is never affected because the outer longitudinal smooth muscle of the rectum encompasses the full circumference (no taeniae; complete longitudinal muscle coat) → no weak intertaenial zones → no points for herniation [4].
- Right-sided diverticula are congenital and true diverticula (involve all layers) [1]
- They occur predominantly in the caecum and ascending colon
- Mechanism is congenital wall weakness rather than acquired pulsion
- Right-sided colon has a thinner wall → a greater length of vasa recta is exposed to injury → right colon is usually the source of diverticular bleeding [3]
- Right-sided diverticula have wider necks and domes → expose more vasa recta to luminal injury [3]
5. Etiology and Pathophysiology
The fundamental equation is: wall weakness + increased intraluminal pressure = diverticulum
Acquired (left-sided): Low fibre diet → increased intraluminal pressure [1]:
- Low dietary fibre → smaller, harder stool boluses
- Colonic segmentation contractions generate higher pressures to propel stool
- Sigmoid has narrowest calibre → highest pressure (Laplace's law) [1][4]
- Mucosa and submucosa herniate through weak points where vasa recta penetrate the circular muscle
- Result: false diverticulum (only mucosa and submucosa)
Congenital (right-sided): Developmental weakness in the caecal/ascending colonic wall → true diverticulum (all layers) [1]
Diverticulitis is caused by microperforation [1]:
Two proposed mechanisms:
- Obstruction of the diverticular neck by a faecolith → stasis within the diverticulum → bacterial overgrowth → mucosal erosion → inflammation and focal necrosis → microperforation → pericolic inflammation [3][4]
- Direct mechanical erosion by inspissated faecal matter → increased diverticular pressure → microperforation [3]
The microperforation is initially small and walled off by pericolic fat and mesentery → localised pericolic inflammation (uncomplicated diverticulitis). If the perforation is larger or the host response is inadequate → abscess, free perforation, or peritonitis (complicated diverticulitis).
This is a beautifully logical sequence [3]:
- When a diverticulum herniates, it drags the penetrating vas rectum (the very vessel whose entry point created the weakness) over the dome of the diverticulum
- The blood vessel is now separated from the bowel lumen only by mucosa (no muscularis protection)
- The exposed vasa recta undergoes injury along its luminal aspect → eccentric intimal thickening and thinning of the media (asymmetric arterial remodelling)
- These changes create segmental weakness of the artery → rupture → arterial bleeding into the lumen
This explains why diverticular bleeding is typically brisk, painless, and arterial — it's not venous oozing; it's a ruptured remodelled artery.
Why right-sided bleeding is more common:
- Right-sided colon has a thinner wall [3]
- Right-sided diverticula have wider necks and domes → more vasa recta length is exposed to luminal injury [3]
- Therefore, right colon is usually the source of colonic diverticular bleeding even in Western populations where left-sided diverticula are more common [3]
Bleeding vs. Inflammation — They Don't Coexist
Diverticular bleeding typically occurs in the absence of diverticulitis. Why? Because the inflammatory process in diverticulitis causes fibrosis and obliteration of the vasa recta → the very vessels that would bleed are destroyed by the inflammation. So bleeding and inflammation are essentially mutually exclusive presentations [3].
- Altered colonic motility may be the underlying basis of symptoms — abnormal segmental contractions cause pain without overt inflammation [3]
- Visceral hypersensitivity — after an episode of diverticulitis, there is heightened pain perception related to:
- Increased neuropeptides in the colonic wall
- Alterations in enteric innervation (a form of "post-inflammatory IBS")
- Low-grade chronic mucosal inflammation (increased mast cells, lymphocytes) [3]
6. Classification
| Site | Type | Population | Anatomical Basis |
|---|---|---|---|
| Left-sided (sigmoid > descending) | False (acquired) | Western predominant | Highest intraluminal pressure; acquired wall weakness |
| Right-sided (caecum, ascending) | True (congenital) | Asian (including HK) — higher proportion | Congenital wall weakness |
This is the clinical staging system for complicated diverticulitis, specifically geared towards choosing the proper surgical procedure [3][4].
Note: Hinchey classification is NOT applicable in right-sided disease [4]
| Stage | Description | Mortality (%) | Treatment |
|---|---|---|---|
| I | Localised pericolic or mesenteric abscess | 0% | Conservative: IV antibiotics ± percutaneous drainage; bowel rest and monitoring. Can be treated as outpatient if stable |
| II | Distant abscess (walled-off pelvic / retroperitoneal abscess) | 5% | IV antibiotics + bowel rest + image-guided percutaneous drainage; possible surgical intervention |
| III | Generalised purulent (suppurative) peritonitis (abscess has ruptured, but bowel wall itself is intact) | 25% | IV antibiotics + bowel rest + Surgery (Hartmann's operation / one-stage resection) |
| IV | Generalised faecal peritonitis (bowel wall perforation) | 50% | IV antibiotics + bowel rest + Surgery (Hartmann's operation) |
Hinchey Classification — Exam Must-Know
You must be able to differentiate Stage III (purulent peritonitis from a ruptured abscess — the bowel itself is intact) from Stage IV (faecal peritonitis from a free bowel wall perforation — faeces are in the peritoneum). Stage IV has 50% mortality — this is a surgical catastrophe. The distinction dictates surgical approach and prognosis [3][4].
7. Clinical Features
7A. Symptoms
The classic presentation triad: lower abdominal pain + fever + leucocytosis [4]
| Symptom | Pathophysiological Basis |
|---|---|
| Lower abdominal pain | Microperforation → pericolic inflammation → visceral and somatic peritoneal irritation. Usually LLQ (sigmoid involvement in Western patients). May involve RLQ and suprapubic area due to: (a) redundant inflamed sigmoid colon lying in the pelvis/RLQ, or (b) right-sided caecal diverticulitis (common in Asians) [1][3][4] |
| Pain is constant and lasts several days prior to presentation | Unlike the colicky pain of obstruction; the constant nature reflects ongoing peritoneal inflammation rather than intermittent muscular spasm |
| Fever (usually low-grade) | Inflammatory response to microperforation and bacterial translocation → release of pyrogenic cytokines (IL-1, IL-6, TNF-α) acting on the hypothalamic thermoregulatory centre |
| Nausea and vomiting | Can result from: (a) reflex ileus — peritoneal inflammation triggers inhibitory sympathetic reflexes that reduce gut motility (paralytic ileus); (b) mechanical bowel obstruction if significant pericolic oedema or abscess compresses the lumen [3] |
| Change in bowel habit | Pericolic inflammation/oedema → luminal narrowing → constipation (more common) or diarrhoea (from mucosal irritation and altered motility) |
| Dysuria / urinary frequency | Inflamed sigmoid colon lies adjacent to the bladder → irritation of the bladder wall by contiguous inflammation |
| Symptom | Pathophysiological Basis |
|---|---|
| Painless massive PR (per rectal) bleeding | Rupture of vasa recta draped over the diverticular dome → arterial haemorrhage into bowel lumen. Painless because the bleeding mechanism does NOT involve inflammation (no microperforation, no peritoneal irritation) [3][4] |
| Typically bright red or maroon blood | Arterial origin; if right-sided bleeding → may be darker/maroon; if left-sided → bright red. Volume of bleeding usually means blood transits quickly regardless |
| Self-limiting in ~80% | Arterial spasm and clot formation at the site of rupture |
| Symptom | Pathophysiological Basis |
|---|---|
| Colicky abdominal pain relieved by defaecation | Altered segmental colonic motility → high-pressure contractions in the diverticular segment → visceral pain. Defaecation decompresses the colon → relief [4] |
| Change in bowel habit (CIBH) | Disordered motility → alternating constipation and diarrhoea (overlaps clinically with IBS) |
| Bloating | Dysmotility → gas trapping in colonic segments |
SUDD vs IBS — Clinical Overlap
SUDD can mimic IBS almost exactly (colicky pain, bloating, CIBH). The key difference is that SUDD occurs in the context of known diverticulosis on imaging. Some experts consider SUDD to be a form of "post-diverticulitis IBS." For exams, the distinguishing point is that SUDD patients typically have demonstrable diverticula on imaging and often a prior history of diverticulitis with persistent symptoms.
7B. Signs
| Sign | Pathophysiological Basis |
|---|---|
| Low-grade fever (37.5–38.5°C) | Localised infection/inflammation → moderate systemic inflammatory response |
| LLQ tenderness (or RLQ in right-sided disease) | Parietal peritoneal irritation by the adjacent inflamed diverticulum → localised somatic pain |
| Localised guarding | Reflex contraction of overlying abdominal wall muscles in response to peritoneal irritation (protective mechanism) |
| Palpable tender mass (occasionally) | Phlegmon (inflamed mass of oedematous colon + mesentery + omentum) walling off the microperforation |
| Reduced bowel sounds | Localised paralytic ileus due to peritoneal inflammation → sympathetic inhibition of peristalsis |
| Tachycardia | Systemic inflammatory response; also may indicate hypovolaemia if bleeding co-exists |
| Complication | Signs | Pathophysiological Basis |
|---|---|---|
| Abscess (pericolic, pelvic, psoas, hepatic) | Persistent fever and abdominal pain despite antibiotics ± tender mass on PR (digital rectal exam); swinging pyrexia; localised peritonism | Microperforation → walled-off collection of pus. Pericolic abscess may track to pelvis (pelvic abscess), along psoas muscle (psoas abscess), or rarely to liver via portal venous drainage [4] |
| Perforation → Peritonitis | Acute abdomen: diffuse rigidity ("board-like"), rebound tenderness, absent bowel sounds, generalised peritonitis; signs of sepsis (fever, tachycardia, hypotension) | Free perforation → faecal/purulent contamination of the peritoneal cavity → diffuse peritoneal inflammation. Hinchey III = purulent; Hinchey IV = faecal [4] |
| Fistula | Most common: colovesical fistula → recurrent dysuria, pneumaturia (air in urine), faecaluria (faeces in urine). Less common: colovaginal (vaginal passage of gas/faeces), coloenteric, colocutaneous | Inflamed diverticulum adheres to adjacent organ → erosion through both walls → abnormal communication. Colovesical is MC because the sigmoid lies directly on the bladder dome. More common in males (uterus acts as barrier in females) [4] |
| Intestinal obstruction | Obstipation, abdominal distension, vomiting, colicky pain; tinkling bowel sounds (mechanical) or absent bowel sounds (ileus) | LBO due to fibrosis and stricture (chronic repeated attacks → progressive fibrosis and luminal narrowing); SBO due to adhesion to inflamed bowel [4] |
| Haemorrhage | Haematochezia (fresh red blood PR), signs of hypovolaemia (tachycardia, hypotension, pallor) | Rupture of vasa recta (see above) — although this typically occurs separately from diverticulitis |
Colovesical Fistula — Classic Exam Vignette
A middle-aged man with known diverticular disease presents with recurrent UTIs, pneumaturia (air bubbles in urine), and faecaluria. This is colovesical fistula until proven otherwise. It's the most common fistula type in diverticular disease. The investigation of choice is CT colonography with water-soluble rectal contrast or CT abdomen/pelvis with contrast [4].
| Presentation | Key Features | Distinguishing Point |
|---|---|---|
| Asymptomatic diverticulosis | None; incidental finding | Found on colonoscopy/imaging for other reasons |
| SUDD | Colicky LLQ pain, bloating, CIBH | No fever, no leucocytosis, wall thickening on CT but no inflammation |
| Acute uncomplicated diverticulitis | LLQ pain (constant), low-grade fever, leucocytosis | Localised peritonism; CT: pericolic fat stranding, wall thickening |
| Complicated diverticulitis | Above + signs of abscess/perforation/fistula/obstruction | CT with Hinchey staging |
| Diverticular bleeding | Painless massive PR bleed | NO fever, NO abdominal pain, NO leucocytosis |
| SCAD | Bloody diarrhoea, LLQ pain | Colonoscopy: interdiverticular mucosal inflammation |
Understanding why specific symptoms occur requires knowing what's next to the sigmoid colon:
| Adjacent Structure | Clinical Consequence |
|---|---|
| Bladder | Dysuria, frequency (contiguous inflammation); colovesical fistula |
| Left ureter | Ureteric obstruction → hydronephrosis (rare) |
| Small bowel loops | Adhesion → SBO; coloenteric fistula |
| Uterus/vagina (females) | Colovaginal fistula (more common post-hysterectomy as the uterine barrier is removed) |
| Anterior abdominal wall | Colocutaneous fistula (rare) |
| Psoas muscle | Psoas abscess (from tracking of pericolic abscess) |
High Yield Summary
Definition: Diverticula = outpouchings of bowel wall; diverticulosis = presence of diverticula; diverticular disease = symptomatic diverticulosis (diverticulitis, bleeding, SUDD).
True vs False: Right-sided = true (congenital, all layers); Left-sided = false (acquired, mucosa + submucosa only).
Epidemiology: 60% prevalence by age 70; 80% asymptomatic; left-sided predominant in West; right-sided more common in Asia → caecal diverticulitis mimics appendicitis → CT is key.
Risk factors: Age, low-fibre diet, obesity, sedentary lifestyle, NSAIDs, steroids, opiates, connective tissue disease.
Pathogenesis: Wall weakness (vasa recta penetration points) + increased intraluminal pressure (Laplace's law, sigmoid narrowest calibre) → diverticula. Diverticulitis = faecolith obstruction → microperforation. Bleeding = vasa recta rupture (separate from inflammation).
Hinchey Classification (NOT for right-sided): I = pericolic abscess (0% mortality); II = pelvic abscess (5%); III = purulent peritonitis (25%); IV = faecal peritonitis (50%).
Clinical triad of diverticulitis: Lower abdominal pain + fever + leucocytosis. LLQ in West, RLQ in Asia.
Diverticular bleeding: Painless, massive, self-limiting (80%), right colon is the usual source.
Complications: Abscess, perforation/peritonitis, fistula (MC = colovesical → pneumaturia, faecaluria), obstruction (LBO from stricture, SBO from adhesion).
Rectum never affected: Full circumferential longitudinal muscle coat.
Active Recall - Diverticular Disease (Part 1: Definition to Clinical Features)
[1] Lecture slides: Diverticular diseases - Dr. J Tsang.pdf [2] Lecture slides: GC 195. Lower and diffuse abdominal pain RLQ problems; pelvic inflammatory disease; peritonitis and abdominal emergencies.pdf [3] Senior notes: felixlai.md (Diverticular disease section) [4] Senior notes: maxim.md (Diverticular disease section) [5] Diagram credit: university of • 2018 University of lowa Health Care [6] Diagram credit: Springer Link
Differential Diagnosis of Diverticular Disease
The differential diagnosis of diverticular disease depends entirely on which presentation you're dealing with. An elderly man with painless massive PR bleeding has a completely different DDx list from a middle-aged woman with LLQ pain and fever. So let's break this down by clinical scenario — the way you'd actually think on a ward round.
The key principle: diverticular disease is a mimic. It can look like cancer, appendicitis, IBD, or ischaemic colitis depending on the presentation. Your job is to systematically exclude dangerous diagnoses (especially colorectal cancer) before settling on diverticular disease as the answer.
A. Differential Diagnosis of Acute Diverticulitis
This is the scenario of lower abdominal pain + fever + leucocytosis — the classic triad [3][4]. The DDx here is essentially "what else causes localised lower abdominal pain with inflammation?"
- Why it's confusable: CRC and diverticulitis share remarkably similar features:
- Both cause bowel wall thickening on CT
- Both can present with change in bowel habit, abdominal pain, and even obstruction
- Both are diseases of the same age group (> 50 years)
- How to distinguish on CT:
- Diverticulitis: pericolonic and mesenteric fat stranding/inflammation, involvement of > 10 cm of colon, absence of enlarged pericolonic lymph nodes, visible diverticula in surrounding segments [3]
- CRC: shorter segment of wall thickening (typically < 10 cm), "shouldering" sign (abrupt transition), pericolonic lymphadenopathy, luminal irregularity/mass
- Critical point: CRC can only be excluded with colonoscopy after resolution of acute inflammation — standard practice is colonoscopy at 6–8 weeks post-recovery [3][5]
"Rule out malignancy" — colonoscopy at 6–8 weeks after acute diverticulitis is mandatory [5]
CRC vs Diverticulitis — The Exam Trap
Never diagnose "diverticulitis" and leave it at that. Up to 1–2% of patients diagnosed with acute diverticulitis on CT are subsequently found to have CRC on follow-up colonoscopy. The two conditions can even coexist. Always follow up with colonoscopy.
- Why it's confusable: Both cause RLQ pain + fever + leucocytosis. This is especially problematic in Asian populations where right-sided (caecal) diverticulitis is common [1][4]
- How to distinguish:
- Appendicitis: pain classically starts periumbilical (visceral afferent T10) then migrates to RLQ (somatic, parietal peritoneum) over 12–24 hours; anorexia is prominent; younger age group (MC 5–12 years) [4]
- Right-sided diverticulitis: pain is localised to RLQ from the outset (no migration); older age group; CT shows colonic wall thickening with diverticula, NOT a distended appendix
- CT scan is the key investigation to differentiate — it shows either a dilated inflamed appendix (appendicitis) or colonic wall thickening with pericolic fat stranding around a diverticulum (diverticulitis) [1][3]
Caecal diverticulitis mimicking appendicitis — Role of CT scan [1]
- Why it's confusable: IBD (especially Crohn's disease) can cause lower abdominal pain, fever, and even fistulae/strictures — complications shared with diverticular disease
- How to distinguish:
- IBD: diarrhoea rather than abdominal pain is the predominant symptom [3]; younger age of onset; extraintestinal manifestations (arthritis, uveitis, skin lesions); chronic relapsing course; Crohn's may show skip lesions, non-caseating granulomas; UC shows continuous mucosal inflammation from rectum proximally
- Diverticulitis: abdominal pain is the predominant symptom; fever and localised peritonism; CT shows pericolic fat stranding with diverticula
- Colonoscopy (after acute phase resolves) is definitive for distinguishing
- Why it's confusable: Infectious colitis (Salmonella, Shigella, Campylobacter, Yersinia, E. coli O157:H7, C. difficile) causes abdominal pain, fever, leucocytosis
- How to distinguish:
- Infectious colitis: diarrhoea (often bloody) rather than abdominal pain is the predominant symptom [3]; acute onset; exposure history (travel, contaminated food, recent antibiotics for C. difficile); stool culture/PCR positive
- Diverticulitis: pain predominates; diarrhoea is not the main feature; CT shows diverticula with pericolic changes
- Why it's confusable: Both occur in elderly patients with vascular risk factors; both cause lower abdominal pain
- How to distinguish:
- Ischaemic colitis: rapid onset of abdominal pain with haematochezia or bloody diarrhoea [3]; risk factors include advanced age, hypertension, DM, dehydration, AF, recent vascular surgery, laxative use, haemodialysis; "watershed" areas affected (splenic flexure, rectosigmoid junction)
- Diverticulitis: gradual onset of constant pain over days; fever and leucocytosis more prominent; bloody stools uncommon in uncomplicated diverticulitis
- CT: ischaemia shows segmental wall thickening with "thumbprinting" in a vascular distribution, ± pneumatosis; diverticulitis shows diverticula + fat stranding
These are especially important in women of reproductive age presenting with lower abdominal/pelvic pain:
| Condition | Distinguishing Features |
|---|---|
| Tubo-ovarian abscess (TOA) | History of PID; bilateral adnexal tenderness; cervical motion tenderness; purulent vaginal discharge; USS/CT shows complex adnexal mass |
| Ovarian torsion | Sudden onset severe unilateral pain; nausea/vomiting; Doppler USS shows absent/reduced ovarian blood flow |
| Ectopic pregnancy | Positive pregnancy test (β-hCG); amenorrhoea; vaginal bleeding; USS shows no intrauterine pregnancy ± adnexal mass/free fluid [3] |
| Ruptured ovarian cyst | Sudden onset pain, often during exercise/intercourse; USS shows free pelvic fluid ± collapsed cyst |
| PID | Recent onset pain worsening with coitus or menses; cervical motion tenderness; purulent endocervical discharge [2] |
Golden Rule in Women of Reproductive Age
Always do a pregnancy test (urine/serum β-hCG) in any woman of reproductive age presenting with lower abdominal pain. Ruptured ectopic pregnancy is a life-threatening emergency that must be excluded before anything else.
| Condition | Distinguishing Features |
|---|---|
| Cystitis / UTI | Dysuria, frequency, urgency; positive urine dipstick (nitrites, leucocyte esterase); urine culture positive. Note: diverticulitis can cause sterile pyuria from adjacent inflammation — don't be fooled [3] |
| Nephrolithiasis / ureteric colic | Severe colicky flank-to-groin pain; haematuria (micro or macro); restlessness (patient cannot lie still, unlike peritonitis where patient lies very still); CT KUB shows calculus |
- Similar presentation as acute appendicitis [2]
- Congenital remnant of omphalomesenteric duct located on small bowel, 2 feet from ileocaecal valve [3]
- Small bowel may migrate into RLQ and mimic appendicitis
- Diagnosis by CT scan [2]
- Incidental finding during appendicectomy [2]
- Treatment: antibiotics; diverticulectomy / small bowel resection [2]
This is the scenario of painless massive PR bleeding. The DDx here is "what else causes significant lower GI haemorrhage?"
From the lecture slides, the DDx of diverticular bleeding includes [5]:
- Angiodysplasia
- Severe colitis
- Rectal ulcer
- Small bowel bleeding
- UGIB
Let's expand on each:
| DDx | Key Features | How to Distinguish from Diverticular Bleeding |
|---|---|---|
| Angiodysplasia (most common cause of LGIB in age > 65) | Abnormal dilated submucosal AVM; painless haematochezia; venous bleeding (tends to be less massive than diverticular bleeding); mostly right-sided (caecum, ascending colon) [6] | Colonoscopy: cherry red spots; angiography: "mother-in-law phenomenon" (early filling, delayed emptying); often occult/chronic causing iron deficiency anaemia rather than massive acute bleed [6] |
| Haemorrhoids (most common in age < 50) | Fresh outlet-type blood (on toilet paper, dripping into bowl, separate from stool); painless unless thrombosed; perianal mass on examination | Blood is bright red, small volume, and clearly outlet-type — not mixed with stool. Digital rectal exam and proctoscopy diagnostic |
| Severe colitis (infectious/IBD/ischaemic) | Bloody diarrhoea with associated symptoms (fever, tenesmus, cramping pain); mucus in stool | Pain and diarrhoea are prominent — diverticular bleeding is painless. Stool cultures, colonoscopy distinguish |
| Rectal ulcer (solitary rectal ulcer syndrome) | Outlet-type bleeding, mucus discharge, tenesmus, sensation of incomplete evacuation | History of straining; rigid sigmoidoscopy shows ulcer on anterior rectal wall 5–10 cm from anal verge |
| Small bowel bleeding | Obscure GI bleeding; may present as haematochezia if brisk; Meckel's diverticulum (especially in young), small bowel tumour, Crohn's | If colonoscopy and OGD negative → capsule endoscopy or CT enterography. Meckel's scan (Tc-99m pertechnetate) for ectopic gastric mucosa |
| UGIB (must not forget!) | Massive upper GI bleed can present as haematochezia (blood acts as cathartic and transits quickly); look for haemodynamic instability out of proportion to apparent blood loss | Always consider UGIB if haemodynamically unstable with PR bleed. NG tube aspirate may show blood/coffee-grounds. OGD is indicated |
| Colorectal cancer | Less commonly presents with massive acute bleed; more often chronic occult blood loss → iron deficiency anaemia; change in bowel habit, weight loss | Colonoscopy (after stabilisation) for definitive diagnosis |
Don't Forget UGIB!
About 10-15% of patients presenting with apparent lower GI bleeding (haematochezia) actually have an upper GI source. A massive peptic ulcer bleed, for instance, can transit so rapidly that blood arrives at the rectum still bright red. If the patient is haemodynamically unstable with PR bleeding, always consider OGD before assuming a lower GI source.
SUDD presents with colicky lower abdominal pain, change in bowel habit, bloating — essentially overlapping with functional bowel disorders:
| DDx | Key Distinguishing Features |
|---|---|
| Irritable Bowel Syndrome (IBS) | Rome IV criteria: recurrent abdominal pain ≥ 1 day/week for 3 months, related to defaecation, with change in stool frequency/form; no structural abnormality; diagnosis of exclusion. SUDD is distinguished by the presence of diverticula on imaging and often a prior history of diverticulitis [3] |
| Colorectal cancer | Constitutional symptoms (weight loss, anorexia); change in stool calibre; iron deficiency anaemia; family history; colonoscopy is definitive |
| IBD (mild) | Chronic diarrhoea predominant; extraintestinal features; elevated faecal calprotectin; colonoscopy with biopsy diagnostic |
| Lactose intolerance | Symptoms temporally related to dairy ingestion; bloating and diarrhoea; hydrogen breath test diagnostic |
| Coeliac disease | Chronic diarrhoea, steatorrhoea, iron/folate deficiency; positive anti-tTG/EMA antibodies; duodenal biopsy shows villous atrophy |
When diverticular disease presents as an acute abdomen with generalised peritonitis, the DDx is the surgical emergency list [4]:
| DDx | Key Distinguishing Features |
|---|---|
| Perforated peptic ulcer (PPU) | Sudden-onset epigastric pain → generalises; history of NSAID use/peptic ulcer disease; erect CXR shows pneumoperitoneum; Valentino's sign — gastric contents tracking down the right paracolic gutter causing RLQ pain mimicking appendicitis [4] |
| Perforated appendicitis | RLQ pain preceding generalised peritonitis; younger age group; CT shows perforated appendix |
| Ischaemic / infarcted bowel | Acute severe abdominal pain out of proportion to examination findings (early); AF or vascular risk factors; raised lactate; CT angiography shows mesenteric vessel occlusion |
| Sigmoid volvulus | Elderly, institutionalised patient; massive abdominal distension; "coffee bean" sign on AXR; CT shows "whirl sign" [6] |
| Strangulated hernia | Irreducible tender groin/incisional swelling; signs of obstruction and/or peritonitis |
| Perforated colorectal cancer | May be indistinguishable from perforated diverticulitis on initial CT; histology of resected specimen gives definitive answer |
This is particularly high-yield for Hong Kong exams given the higher prevalence of right-sided diverticular disease [1][2][4]:
The RLQ DDx (from lecture slides) [2][4]:
| Category | Conditions |
|---|---|
| Caecum/Right colon | Caecal diverticulitis, acute appendicitis, caecal/appendiceal tumour (lymphoma, carcinoid) |
| Terminal ileum | Crohn's disease, Meckel's diverticulitis, intestinal TB, Yersinia ileitis |
| Urological | Ureteric colic, testicular torsion, UTI |
| Gynaecological | Ovulation pain ("Mittelschmerz"), ovarian cyst complications (rupture/torsion), PID, ruptured ectopic pregnancy |
| Other | Mesenteric adenitis (in children), strangulated inguinal/femoral hernia, PPU with Valentino's sign |
CT abdomen with IV contrast is the diagnostic test of choice when differentiating these RLQ causes — it is the single most important investigation [1][2][5]
| Presentation of Diverticular Disease | Top DDx to Exclude | Key Investigation |
|---|---|---|
| Acute diverticulitis (LLQ/RLQ pain, fever, leucocytosis) | CRC, appendicitis, IBD, ischaemic colitis, gynaecological causes | CT abdomen/pelvis with contrast → colonoscopy at 6–8 weeks |
| Diverticular bleeding (painless massive PR bleed) | Angiodysplasia, CRC, haemorrhoids, colitis, UGIB | Colonoscopy → angiography if inconclusive |
| SUDD (colicky pain, CIBH) | IBS, CRC, IBD, lactose intolerance | Colonoscopy to exclude organic pathology |
| Complicated diverticulitis (acute abdomen) | PPU, perforated appendix, ischaemic bowel, volvulus | CT abdomen/pelvis; erect CXR (pneumoperitoneum) |
High Yield Summary
The single most important DDx across all presentations is colorectal cancer (CRC) — always exclude it. Colonoscopy at 6–8 weeks post-acute diverticulitis is mandatory.
Right-sided diverticulitis mimics acute appendicitis — CT abdomen is the key differentiator, especially in Asian populations including Hong Kong.
Diverticular bleeding DDx: angiodysplasia, severe colitis, rectal ulcer, small bowel bleeding, UGIB. Don't forget massive UGIB can present as haematochezia.
In women of reproductive age: always exclude ectopic pregnancy (β-hCG) and gynaecological causes (TOA, ovarian torsion, PID) before diagnosing diverticular disease.
Meckel's diverticulitis presents similarly to appendicitis; may be an incidental finding during appendicectomy; diagnosed by CT.
Ischaemic colitis has rapid onset + haematochezia (vs. gradual onset + constant pain in diverticulitis).
IBD and infectious colitis: diarrhoea predominates (vs. pain predominates in diverticulitis).
Active Recall - Differential Diagnosis of Diverticular Disease
References
[1] Lecture slides: Diverticular diseases - Dr. J Tsang.pdf [2] Lecture slides: GC 195. Lower and diffuse abdominal pain RLQ problems; pelvic inflammatory disease; peritonitis and abdominal emergencies.pdf [3] Senior notes: felixlai.md (Diverticular disease section) [4] Senior notes: maxim.md (Diverticular disease section) [5] Lecture slides: Diverticular diseases - Dr. J Tsang.pdf (p8, p10) [6] Senior notes: maxim.md (Angiodysplasia / Volvulus sections)
Diagnostic Criteria, Algorithm, and Investigations for Diverticular Disease
Unlike conditions such as rheumatic fever (Jones criteria) or SLE (ACR criteria), diverticular disease does not have formal validated diagnostic criteria with sensitivity/specificity scores. Instead, the diagnosis is clinico-radiological — you combine the clinical picture with imaging findings. Let me walk you through exactly how this works for each presentation.
1. Diagnostic Criteria by Presentation
The clinical diagnosis rests on the triad of lower abdominal pain + fever + leucocytosis [1][4], but the definitive diagnosis requires imaging:
| Component | What You're Looking For | Why |
|---|---|---|
| Clinical triad | Lower abdominal pain (LLQ or RLQ), fever, leucocytosis | Microperforation → localised pericolic inflammation → peritoneal irritation (pain), systemic inflammatory response (fever, leucocytosis) |
| CT abdomen + pelvis with IV contrast | Bowel wall thickening > 4 mm + pericolic fat stranding + visible diverticula | CT scan helps to confirm diagnosis and assess the severity [2] — it is both diagnostic AND prognostic (Hinchey staging) |
| Absence of other diagnoses | Must exclude CRC, appendicitis, IBD, gynaecological/urological causes | Diverticulitis is partly a diagnosis of exclusion in the acute setting; definitive exclusion of CRC requires colonoscopy later |
Diagnosis of uncomplicated diverticulitis: CT abdomen and pelvis with IV contrast [5]
Avoid colonoscopy in the acute setting [5]
Colonoscopy at 6–8 weeks to rule out malignancy [5]
Why avoid colonoscopy acutely? Because the inflammation is peridiverticular (outside the bowel wall). Air insufflation during colonoscopy risks converting a sealed microperforation into a free perforation — a catastrophe. The colonoscopy won't even show much diagnostically since the disease process is extraluminal [3].
- Clinical: painless massive PR bleeding in a patient with known or suspected diverticulosis
- Investigation of choice: colonoscopy [5] — both diagnostic (identify bleeding source) and therapeutic (haemostasis)
- No formal diagnostic criteria; diagnosis is made by visualising a bleeding diverticulum or stigmata of recent haemorrhage at a diverticulum on colonoscopy
- Clinical: colicky abdominal pain, altered bowel habit in a patient with known diverticulosis
- CT shows wall thickening in the absence of inflammatory changes (no fat stranding, no abscess) [3]
- Essentially a diagnosis of exclusion after ruling out diverticulitis, CRC, and IBD
Here is the systematic approach to a patient presenting with suspected diverticular disease, organised by clinical scenario:
The Two Phases of Diagnosis
Think of diagnosing diverticular disease in two phases:
- Acute phase: CT abdomen/pelvis with IV contrast → confirm diverticulitis, stage severity (Hinchey), guide immediate management. NO colonoscopy.
- Recovery phase (6–8 weeks later): Colonoscopy → definitively exclude CRC, assess for IBD/polyps, evaluate for strictures.
This two-phase approach is one of the most commonly tested concepts.
3. Investigation Modalities — Detailed Breakdown
| Investigation | Key Findings | Clinical Significance |
|---|---|---|
| Urinalysis [2][3] | Sterile pyuria | Adjacent sigmoid inflammation irritates the bladder wall → WBCs in urine without bacterial infection. Don't mistake this for UTI! [3] |
| Urine culture [3][4] | Presence of colonic flora (e.g., E. coli, Bacteroides) | Pathognomonic for colovesical fistula — bacteria from the colon have gained direct access to the urinary tract through the fistulous communication [3] |
| Pregnancy test [2] | Positive β-hCG | Excludes ectopic pregnancy in women of reproductive age — a critical differential for lower abdominal pain |
Blood tests: CBC D/C, LRFT, amylase, clotting profile, ABG, type and screen [2][4]
| Investigation | Key Findings | Why It's Done |
|---|---|---|
| CBC with differentials | Leucocytosis (raised WCC with neutrophilia) | Confirms systemic inflammatory response to infection/inflammation. Part of the diagnostic triad. Drop in Hb suggests bleeding [3][4] |
| CRP | Elevated | Non-specific inflammatory marker; useful for monitoring response to treatment. CRP > 200 mg/L has been associated with complicated diverticulitis |
| Electrolyte profile (LRFT) | Derangements in Na⁺, K⁺, urea, creatinine | Dehydration from reduced oral intake, vomiting, third-space losses; renal impairment from sepsis/hypovolaemia [3] |
| Serum amylase and lipase | Usually normal or mildly elevated | Primarily to exclude acute pancreatitis as a differential for upper/diffuse abdominal pain. Mild elevation can occur with any intra-abdominal inflammation [3] |
| LFT | Usually normal | Exclude hepatobiliary pathology; may be deranged if hepatic abscess develops from portal pyaemia |
| ABG and lactate [2] | Raised lactate, metabolic acidosis | Suggests tissue hypoperfusion — raises concern for ischaemic bowel, septic shock, or peritonitis with cardiovascular compromise |
| Clotting profile [2] | PT/INR, APTT | Essential pre-operatively and if patient is on anticoagulants (which increase bleeding risk in diverticular bleeding) |
| Type and screen / cross-match [2] | Blood group and antibody screen | Preparation for potential transfusion (especially in diverticular bleeding or if surgery anticipated) |
Imaging: Erect CXR, erect and supine AXR [2][3]
| Finding | Significance | Pathophysiological Basis |
|---|---|---|
| Free gas under diaphragm (pneumoperitoneum) on erect CXR | Perforation — surgical emergency | Free bowel perforation → intraluminal air escapes into peritoneal cavity → rises to collect under the diaphragm [3] |
| Air-fluid levels with bowel dilatation on AXR | Obstruction or paralytic ileus | Mechanical obstruction (stricture from chronic diverticulitis) → proximal accumulation of gas and fluid. Alternatively, peritoneal inflammation → reflex inhibition of peristalsis (paralytic ileus) [3] |
| Dilated bowel on AXR [4] | Obstruction | LBO from diverticular stricture (chronic fibrosis) or SBO from adhesion to inflamed segment |
| Soft tissue densities | Abscess | Collection of pus and inflammatory tissue creates an area of increased soft tissue density [3] |
Plain Films — Screening, Not Diagnostic
Erect CXR and AXR are quick, cheap screening tools done in the emergency department. They can identify life-threatening complications (perforation, obstruction) but they cannot confirm the diagnosis of diverticulitis. For that, you need CT.
Ultrasound can be useful as a first-line bedside investigation, especially when CT is not immediately available or to avoid radiation (e.g., young patients, pregnancy).
| Finding | Significance |
|---|---|
| Diverticula in surrounding segments | Confirms underlying diverticulosis [3] |
| Bowel wall thickening > 4 mm at point of maximal tenderness (segmental mural thickening) | Localised inflammation — hallmark of diverticulitis [3] |
| Hypoechoic peridiverticular inflammatory reaction | Pericolic inflammation/phlegmon [3] |
| Mural and peridiverticular abscess ± gas bubbles | Complicated diverticulitis with abscess formation [3] |
| Anechoic mass containing echogenic debris | Abscess [3] |
| Hypoechoic area with extraluminal air bubbles extending into bladder/vagina/abdominal wall | Fistula [3] |
| Ascites, diffuse peritoneal thickening, scattered loculated fluid collections | Perforation with peritonitis [3] |
Limitations: Operator-dependent; bowel gas obscures views; limited sensitivity for deep pelvic structures; cannot reliably stage severity (Hinchey).
E. CT Abdomen + Pelvis with IV Contrast — THE Gold Standard
This is the single most important investigation for acute diverticulitis. It does four things simultaneously [2][4][5]:
- Diagnostic: confirms the diagnosis
- Assesses complications: abscess, fistula, perforation, obstruction
- Aids treatment: guides percutaneous drainage of abscess
- Prognostic: enables Hinchey classification staging [4]
CT scan helps to confirm diagnosis and assess the severity [2]
| CT Finding | What It Represents | Why It Occurs |
|---|---|---|
| Colonic diverticula | Underlying diverticulosis | Outpouchings of mucosa/submucosa through the colonic wall |
| Localised bowel wall thickening > 4 mm | Mural oedema and inflammation | Microperforation → inflammatory infiltrate and oedema within the bowel wall |
| Increased soft tissue density in pericolonic fat (fat stranding) | Pericolic inflammation | Inflammatory exudate and oedema spread from the microperforation into the surrounding mesenteric fat — this is the hallmark CT sign of diverticulitis [3] |
| Complication | CT Findings | Explanation |
|---|---|---|
| Abscess | Fluid collection with surrounding inflammatory changes; centre may contain air, air-fluid levels, or low-attenuation necrotic debris | Walled-off collection of pus from contained microperforation. Air within the abscess comes from the bowel communication |
| Abscess size | 5 cm is the cut-off [4] | < 5 cm: likely to resolve with IV antibiotics alone. ≥ 5 cm: likely requires image-guided (CT-guided) percutaneous drainage |
| Fistula | Extracolonic air collections within organs other than bowel (e.g., air in bladder = colovesical fistula) | Inflammatory erosion through to adjacent organ creates abnormal communication; air/gas tracks from bowel into the other organ |
| Obstruction | Dilated loops of bowel with air-fluid levels in proximity to an area with pericolic fat stranding | Inflammatory oedema or chronic fibrotic stricture narrows the lumen → proximal bowel dilates |
| Perforation | Free intraperitoneal air in patient with peritonitis | Unsealed microperforation or macro-perforation → free air escapes into peritoneal cavity |
| Stage | CT Appearance | Management Implication |
|---|---|---|
| I | Small pericolic or mesenteric abscess ( < 5 cm) | IV antibiotics ± drainage |
| II | Larger distant abscess (pelvic, retroperitoneal) | IV antibiotics + CT-guided percutaneous drainage |
| III | Free fluid/gas without connection to bowel lumen; no faecal material in peritoneum | Surgery required (Hartmann's or primary resection-anastomosis) |
| IV | Free faecal matter and gas in peritoneal cavity; communication with bowel lumen visible | Emergency surgery (Hartmann's) |
Hinchey classification: note NOT applicable in right-sided disease [4]
Why Hinchey Doesn't Apply to Right-Sided Disease
The Hinchey classification was developed and validated for left-sided (sigmoid) diverticulitis with its specific anatomical relationships. Right-sided diverticula are congenital and true (involving all layers), have different natural history, and right-sided complicated diverticulitis is managed differently (typically right hemicolectomy rather than Hartmann's procedure). The staging system simply doesn't translate.
This is high-yield — you need to know this for exams:
| Feature | Diverticulitis | CRC |
|---|---|---|
| Length of involvement | > 10 cm (long segment) | < 10 cm (short segment) |
| Pericolonic fat stranding | Prominent (the hallmark feature) | Mild or absent |
| Pericolonic lymph nodes | Absent or small/reactive | Enlarged (suggesting malignant infiltration) |
| Surrounding diverticula | Present in adjacent colon | May or may not be present |
| Transition zone | Gradual thickening | Abrupt "shouldering" (sharp transition from normal to thickened bowel) |
| Luminal appearance | Smooth narrowing | Irregular, eccentric mass/luminal destruction |
Features suggestive of acute diverticulitis include presence of pericolonic and mesenteric inflammation, involvement of > 10 cm of colon, and absence of enlarged pericolonic lymph nodes [3]
The 1-2% Rule
Even with these distinguishing features, 1–2% of patients diagnosed as "uncomplicated diverticulitis" on CT will harbour an underlying CRC. With complicated diverticulitis, the rate of concurrent malignancy jumps to ~10-17% [5]. This is precisely why follow-up colonoscopy is non-negotiable.
From the lecture data showing studies of patients with uncomplicated vs complicated diverticulitis [5]:
| Disease Type | Malignancy Rate |
|---|---|
| Uncomplicated diverticulitis | ~0–1.1% (very low but not zero) |
| Complicated diverticulitis | ~13–17% (significantly higher!) |
| Colorectal polyps (on follow-up colonoscopy) | ~7–32% |
This data reinforces that colonoscopy at 6–8 weeks is essential, especially after complicated disease [5].
| Feature | Details |
|---|---|
| When to use | When you want to avoid radiation exposure (young patients, pregnant women, recurrent imaging needed) [3] |
| Findings | Same as CT: colonic diverticula, colonic wall thickening, pericolonic exudates and oedema [3] |
| Limitations | Longer scan time; less available in emergencies; more expensive; motion artefact |
| Advantage | Excellent soft tissue contrast; no ionising radiation; useful for characterising pelvic abscesses and fistulae |
G. Colonoscopy
Colonoscopy plays different roles depending on the clinical scenario:
Avoid colonoscopy in the acute setting [5]
- NO role in establishing the diagnosis of acute diverticulitis because the inflammation is peridiverticular (extraluminal) — colonoscopy only visualises the mucosal surface [3]
- Risk of perforation during air insufflation in an already weakened, inflamed bowel wall [4]
- Contraindication: acute diverticulitis [4]
Investigations for diverticulosis: barium enema / colonoscopy / CT colonography [5]
- Colonoscopy can directly visualise diverticula and simultaneously screen for polyps/CRC
- Often the investigation that incidentally discovers diverticulosis
- Especially useful for colovesical fistula [4] — water-soluble contrast instilled per rectum can be seen tracking into the bladder through the fistula
- Alternative to colonoscopy when:
- Colonoscope cannot reach the caecum (stricture, tortuous colon)
- Patient cannot tolerate colonoscopy
- Provides extraluminal information (unlike conventional colonoscopy)
- Cannot take biopsies — if a suspicious lesion is found, colonoscopy is still needed
- NOT recommended and relatively contraindicated in the acute setting [3]
- Risk of barium peritonitis if there is a perforation — barium is intensely irritant to the peritoneum and cannot be reabsorbed (unlike water-soluble contrast)
- Contrast enema and small bowel studies are extremely useful in defining the course of fistula in complicated diverticulitis [3]
- Largely superseded by CT colonography in modern practice
- Classic finding in diverticulosis: saw-tooth pattern of the colonic mucosa with outpouchings
- Indicated when colonoscopy cannot accurately localise the diverticular bleeding source [3]
- 3-vessel mesenteric angiogram: coeliac artery, SMA, IMA [3]
- Detects active bleeding at a rate of > 1 mL/min [3]
- Can show: contrast extravasation at the bleeding site
- Angiogram ± embolisation [5] — selective catheterisation and embolisation can control bleeding
- However, embolisation carries risk of bowel ischaemia/gangrene — must be done selectively by experienced interventional radiologists [3]
- Indicated when colonoscopy cannot accurately localise the diverticular bleeding source [3]
- More sensitive than angiography: detects slow intermittent bleeding at > 0.1 mL/min [3]
- Mechanism: patient's own RBCs are labelled with Tc-99m → reinjected → serial gamma camera images over 24 hours → localisation of tracer accumulation at the bleeding site
- Useful for intermittent bleeding that may not be active at the time of angiography
- Limitation: gives only approximate anatomical localisation (not precise enough for surgery alone — usually needs confirmatory angiography or colonoscopy)
This is a critical algorithm from the lectures [4][5]:
Localisation of bleeding: colonoscopy → angiography → on-table lavage and colonoscopy → subtotal colectomy and ileostomy [4]
80% of diverticular bleeding is self-limiting [1][5]. Rebleeding occurs in ~20–30% [7]
Treatment of diverticular bleeding: endoscopic vs surgical resection [7]
| Clinical Scenario | First-Line Investigation | Additional Investigations | What NOT to Do |
|---|---|---|---|
| Acute diverticulitis | CT abdomen + pelvis with IV contrast [2][5] | Bloods (CBC D/C, LRFT, amylase), urinalysis, erect CXR + AXR | Avoid colonoscopy [5]; avoid barium enema |
| Post-recovery from acute diverticulitis | Colonoscopy at 6–8 weeks [5] | CT colonography if colonoscopy incomplete | Don't skip this — rule out malignancy |
| Diverticular bleeding | Colonoscopy [5] | Mesenteric angiography, Tc-99m RBC scan, CT angiography | Don't assume it's lower GI — exclude UGIB if unstable |
| Asymptomatic diverticulosis | Colonoscopy / barium enema / CT colonography [5] | None specifically | No treatment needed if truly asymptomatic |
| Suspected colovesical fistula | CT colonography with water-soluble rectal contrast [4] | Urine culture (colonic flora), cystoscopy | Don't use barium (risk of barium peritonitis if free perforation) |
| Acute abdomen / suspected perforation | Erect CXR (pneumoperitoneum) → CT | Bloods including lactate, ABG | Don't delay resuscitation; don't do colonoscopy |
6. Physical Examination Findings (As Part of Diagnostic Workup)
| Finding | Significance |
|---|---|
| Tender abdominal mass | Phlegmon (inflamed mass of oedematous colon + mesentery + omentum) or peridiverticular abscess [3] |
| Peritoneal signs: rigidity, localised guarding, rebound tenderness | Localised peritonitis from pericolic inflammation; if generalised → perforation [3] |
| Absent bowel sounds | Paralytic ileus (peritoneal inflammation) or advanced obstruction |
| Hyperactive bowel sounds | Mechanical obstruction (stricture) |
| Finding | Significance |
|---|---|
| Mass or tenderness | Distal sigmoid abscess — the abscess has tracked into the pelvis and is palpable through the rectal wall [3] |
| Blood on glove | Suggests bleeding or mucosal involvement |
| Bogginess/fullness | Pelvic abscess or collection |
Investigations for acute abdomen [2]: Bedside tests: urinalysis, pregnancy test. Blood tests: blood count, renal and liver function, amylase, clotting profile, ABG, type and screen. Imaging: erect CXR, erect and supine AXR, USG, CT, contrast studies. Endoscopy: colonoscopy, upper endoscopy [2]
High Yield Summary
The diagnosis of acute diverticulitis is clinico-radiological: clinical triad (lower abdominal pain + fever + leucocytosis) confirmed by CT abdomen + pelvis with IV contrast (gold standard).
CT is diagnostic, assesses complications, aids treatment (guides drainage), and is prognostic (Hinchey staging).
Key CT findings: bowel wall thickening > 4 mm, pericolic fat stranding, visible diverticula. Complications: abscess (5 cm cut-off for drainage), fistula (extracolonic air in adjacent organs), obstruction (dilated loops), perforation (free air).
CT distinguishes diverticulitis from CRC: diverticulitis involves > 10 cm, has prominent fat stranding, no enlarged lymph nodes. CRC has short-segment involvement, shouldering, and lymphadenopathy.
Colonoscopy is CONTRAINDICATED acutely (risk of perforation). Colonoscopy at 6–8 weeks post-recovery is mandatory to exclude CRC — malignancy rate in complicated diverticulitis is ~10-17%.
Diverticular bleeding investigation: colonoscopy (first-line) → mesenteric angiography → on-table lavage and colonoscopy → subtotal colectomy if source not found.
Sterile pyuria on urinalysis = adjacent inflammation. Colonic flora on urine culture = colovesical fistula.
Hinchey classification is NOT applicable to right-sided disease.
Active Recall - Diagnosis and Investigations of Diverticular Disease
References
[1] Lecture slides: Diverticular diseases - Dr. J Tsang.pdf (p3, p4, p8) [2] Lecture slides: GC 195. Lower and diffuse abdominal pain RLQ problems; pelvic inflammatory disease; peritonitis and abdominal emergencies.pdf (p12, p18, p19) [3] Senior notes: felixlai.md (Diverticular disease section — Diagnosis) [4] Senior notes: maxim.md (Diverticular disease section — Investigations) [5] Lecture slides: Diverticular diseases - Dr. J Tsang.pdf (p5, p6, p7, p10, p11) [7] Lecture slides: GC 186. Lower and diffuse abdominal painfresh blood in stool.pdf (p9)
Management of Diverticular Disease
Management of diverticular disease is entirely dictated by which clinical entity you're dealing with — asymptomatic diverticulosis, uncomplicated diverticulitis, complicated diverticulitis (staged by Hinchey), diverticular bleeding, or chronic complications like fistula and stricture. Let me walk you through each systematically.
Management: Conservative [5]
The vast majority (~80%) of people with diverticulosis remain asymptomatic and need no medical or surgical treatment — just risk factor modification to prevent progression.
| Intervention | Rationale |
|---|---|
| High-fibre diet [4] | Increases stool bulk → reduces intraluminal pressure (the fundamental pathogenic mechanism) → fewer new diverticula form and existing diverticula are less likely to become symptomatic. Aim for 25–30 g fibre/day |
| Bulk laxatives (e.g., methylcellulose, psyllium/ispaghula husk) [4] | Hydrophilic agents that absorb water and swell → increase stool bulk → reduce colonic segmentation pressures. Unlike stimulant laxatives, these do NOT cause uncontrolled contractions |
| Weight reduction [4] | Obesity increases intra-abdominal pressure and promotes chronic inflammation |
| Avoid NSAIDs [4] | NSAIDs disrupt mucosal barrier (inhibit prostaglandin-mediated mucosal protection) → increase risk of microperforation and diverticular bleeding |
| Avoid stimulant laxatives [4] | Stimulant laxatives (e.g., senna, bisacodyl) cause forceful uncoordinated colonic contractions → increase intraluminal pressure → worsen diverticular disease. This is counterintuitive — patients think "laxatives help" but the wrong type makes things worse |
| Regular physical activity | Improves colonic motility and transit time, reducing intraluminal pressure |
Stimulant vs Bulk Laxatives — Know the Difference
Students commonly recommend "laxatives" generically. In diverticular disease, bulk-forming laxatives (methylcellulose, psyllium) are beneficial but stimulant laxatives (senna, bisacodyl) are harmful because they cause high-pressure uncoordinated contractions. Always specify the type.
Antispasmodics if colicky pain [4]:
- Mebeverine or hyoscine butylbromide — direct smooth muscle relaxants that reduce colonic spasm without affecting normal peristalsis
- Plus all the conservative measures above (high-fibre diet, bulk laxatives, weight loss)
- Some patients benefit from low-dose tricyclic antidepressants for visceral hypersensitivity (similar to IBS management)
4. Management of Uncomplicated Acute Diverticulitis
Treatment: IV antibiotics [5]
Colonoscopy at 6–8 weeks to rule out malignancy [5]
The goal is to control the infection from the microperforation with antibiotics and rest the bowel to allow healing.
The colonic flora involved in diverticulitis include Gram-negative aerobes (e.g., E. coli, Klebsiella) and anaerobes (e.g., Bacteroides fragilis). Antibiotic regimens must therefore cover both Gram-negatives AND anaerobes [4].
Who qualifies: immunocompetent, tolerating oral intake, no significant comorbidities, reliable follow-up, no CT evidence of complications (Hinchey 0 — simple diverticulitis without abscess).
| Regimen | Duration | Spectrum |
|---|---|---|
| Amoxicillin-clavulanate (Augmentin) | 7–10 days | Broad-spectrum: GN aerobes + anaerobes (clavulanate = β-lactamase inhibitor extending amoxicillin's spectrum) |
| Metronidazole + Co-trimoxazole (TMP-SMX) | 7–10 days | Metronidazole covers anaerobes; co-trimoxazole covers GN aerobes |
| Ciprofloxacin (+ metronidazole if needed) | 7–10 days | Fluoroquinolone with excellent GN cover; add metronidazole for anaerobic coverage |
| Moxifloxacin | 7–10 days | 4th-generation fluoroquinolone with inherent anaerobic coverage (no need to add metronidazole) |
Evolving Practice — Antibiotics for Uncomplicated Diverticulitis
Recent evidence (AVOD trial 2012, DIABOLO trial 2017) suggests that antibiotics may NOT be necessary for truly uncomplicated diverticulitis in immunocompetent patients without systemic signs. Some guidelines now recommend observation without antibiotics for mild uncomplicated cases. However, for exam purposes, the standard teaching remains antibiotics for 7–10 days unless the examiner specifically asks about latest evidence.
Who qualifies: unable to tolerate oral intake, significant comorbidities, immunocompromised, failed outpatient treatment, or CT shows early complications.
| Component | Details | Rationale |
|---|---|---|
| Bowel rest (NPO) | Nil by mouth | Reduces colonic motility and intraluminal pressure → allows the microperforation to seal; reduces ongoing bacterial contamination of the pericolic space |
| IV fluid resuscitation | Isotonic crystalloids (NS, Hartmann's) | Replace losses from reduced oral intake, vomiting, third-space fluid sequestration |
| IV antibiotics | Piperacillin-tazobactam (Tazocin) OR Metronidazole + Cephalosporin/Fluoroquinolone [3] | Piperacillin-tazobactam: ultra-broad spectrum covering GN aerobes, anaerobes, and many Gram-positives. Alternative: metronidazole (anaerobes) + ceftriaxone or ciprofloxacin (GN aerobes) |
| Analgesia | Paracetamol first-line; avoid opioids if possible | Opioids slow colonic transit → increase intraluminal pressure; but may be needed for severe pain |
| Monitoring | Clinical: pain, fever, abdominal exam, vitals; Bloods: WCC, CRP trending | Look for improvement within 48–72 hours; failure to improve suggests complication (abscess, perforation) |
After resolution: Colonoscopy at 6–8 weeks to rule out malignancy [5]
5. Management of Complicated Diverticulitis
Resuscitation with IVF + antibiotics. Percutaneous drainage for abscess. Consider emergency surgery [5]
Consider emergency surgery when [5]:
- Unresponsive to antibiotics
- Septic shock (high fever, tachycardia, hypotension, oliguria)
- Generalised peritonitis (Hinchey III and IV)
Additional indications [3]:
- Frank (free) perforation
- Colonic obstruction not amenable to conservative management
- Abscess failing non-operative intervention (CT-guided drainage)
| Hinchey Stage | Management | Rationale |
|---|---|---|
| I — Pericolic abscess | IV antibiotics ± CT-guided percutaneous drainage [4][5] | Small pericolic abscess ( < 5 cm) may resolve with antibiotics alone. Larger abscess ( ≥ 5 cm) requires drainage to achieve source control. CT-guided drainage avoids surgery in many patients |
| II — Distant abscess (pelvic/retroperitoneal) | IV antibiotics + CT-guided percutaneous drainage [4][5] | Distant abscess is too large and too far from the primary site to resolve with antibiotics alone; percutaneous drainage achieves source control and may serve as a "bridge" to interval elective surgery |
| III — Generalised purulent peritonitis | Emergency surgery [4][5] | Ruptured abscess has contaminated the peritoneal cavity → conservative management will not achieve source control → requires operative washout and resection |
| IV — Generalised faecal peritonitis | Emergency surgery (Hartmann's procedure) [4][5] | Free bowel perforation with faecal contamination → highest mortality (50%) → definitive surgical source control is mandatory |
If a patient on IV antibiotics ± drainage does not improve within 48–72 hours (persistent fever, worsening pain, rising WCC/CRP), you must:
- Repeat CT to reassess — look for enlarging abscess, new perforation, or missed diagnosis
- Escalate to surgery if the source is not controllable non-operatively
6. Surgical Treatment Options
| Feature | Details |
|---|---|
| Indication | Hinchey I or II diverticulitis (localised contamination) where the patient can tolerate preoperative bowel preparation and tissues are not too oedematous/inflamed [3] |
| What's done | Resection of the diseased colonic segment including the abscess, with immediate anastomosis (joining the two bowel ends) |
| Resection margins | Proximal: where colon becomes soft, uninflamed, and non-oedematous. It is NOT necessary to resect all diverticulum-bearing colon since diverticula in the transverse or descending colon rarely cause further symptoms [3]. Distal: upper 1/3 of the rectum (because the rectum is NEVER involved in diverticulitis — taeniae coli have fused by that point) [3] |
| Advantage | Single operation; no stoma; better quality of life |
| Risk | Anastomotic leak — higher risk if performed in contaminated/inflamed field |
Resection Margins — A Classic Exam Point
You do NOT need to resect every single diverticulum. The proximal margin is where the colon becomes soft and uninflamed. The distal margin must reach the upper rectum — inadequate distal margin is the most common cause of recurrent diverticulitis after resection [4]. This is because the diseased, high-pressure sigmoid colon must be completely removed; leaving even a short stump of sigmoid leads to recurrence.
The MOST commonly performed and preferred approach for emergency surgery [3]
| Feature | Details |
|---|---|
| Indication | Hinchey III or IV diverticulitis (diffuse contamination) [3][4]. Also used when anastomosis is too risky (haemodynamic instability, severe contamination, immunosuppression) |
| Stage I | Resection of the diseased colonic segment → creation of an end colostomy (proximal limb brought out as a stoma to divert the faecal stream) + creation of a rectal stump (Hartmann's pouch) by oversewing the distal rectum [3] |
| Stage II (reversal, typically 3–6 months later) | Intestinal continuity is re-established by a descending colorectostomy (takedown of colostomy and anastomosis to the rectal stump) [3] |
| Why 2-stage? | Primary anastomosis is contraindicated in Hinchey III-IV because excessive contamination and inflamed/oedematous tissues dramatically increase the risk of anastomotic leak [3][4] — an anastomotic leak in a septic patient with peritonitis would be catastrophic |
| Disadvantage | Stoma-related morbidity; reversal of Hartmann's is a technically challenging operation (adhesions, difficult pelvic dissection to find the rectal stump); up to 30-40% of Hartmann's procedures are never reversed |
Why is anastomotic leak so dangerous? An anastomotic leak means the joined bowel ends have separated → faecal matter leaks into the peritoneal cavity → peritonitis, sepsis, multi-organ failure. Risk factors for leak include ischaemia, tension, infection, malnutrition, steroids, and performing anastomosis in a contaminated field [4]. This is exactly why you DON'T do a primary anastomosis in Hinchey III-IV.
| Feature | Details |
|---|---|
| Indication | Hinchey III or IV in stable patients where the bowel is not excessively oedematous [3]; OR Hinchey I-II with relative contraindication to primary anastomosis alone |
| What's done | Resection + primary anastomosis (as in 1-stage) BUT with a proximal defunctioning loop ileostomy to divert the faecal stream away from the anastomosis → protects the anastomosis while it heals |
| Stage II | Reversal of the loop ileostomy (a technically simpler procedure than reversal of Hartmann's) [3] |
| Advantage over Hartmann's | Maintains bowel continuity from the outset; reversal of loop ileostomy is easier than takedown of a Hartmann's pouch [3] |
| Disadvantage | Only appropriate in stable patients; still requires a second operation |
Laparoscopic lavage — feasible [5]
| Feature | Details |
|---|---|
| Indication | Hinchey III (purulent peritonitis) — the bowel wall itself is intact (no free faecal perforation) [3][5] |
| What's done | Laparoscopic washout of the peritoneal cavity with warm saline + placement of drains. The diseased bowel segment is NOT resected |
| Rationale | In Hinchey III, the peritonitis is from a ruptured abscess (pus), not a free bowel perforation. The bowel wall is intact. So theoretically, washing out the pus and giving antibiotics may be sufficient without the morbidity of resection + stoma |
| Advantage | Avoids bowel resection and stoma; faster recovery; lower morbidity |
| Controversy | This approach remains controversial and requires additional prospective trials before formal recommendations [3]. The SCANDIV and LOLA trials showed higher re-intervention rates with lavage compared to resection. Current consensus: may be considered in selected cases (Hinchey III, stable patient) but NOT standard of care |
| Contraindication | Hinchey IV (faecal peritonitis) — you CANNOT just wash out faecal contamination without resecting the perforated bowel |
7. Elective (Interval) Colectomy
Interval colectomy — this is a planned sigmoid colectomy with primary anastomosis performed after resolution of the acute episode (typically 6–12 weeks later) [5].
| Indication | Rationale |
|---|---|
| Previous complicated diverticulitis | History of abscess, perforation, fistula, or obstruction indicates high-risk anatomy prone to recurrence and further complications [3][5] |
| Immunocompromised patients | Impaired immune response means complications are harder to manage conservatively; lower threshold for surgery. These patients may not mount the usual inflammatory "walling-off" response → higher risk of free perforation |
| Inability to exclude malignancy | If colonoscopy post-recovery cannot definitively exclude CRC (e.g., stricture preventing passage of scope, persistent mass), resection serves both therapeutic and diagnostic purposes [3] |
| Patients with complicated disease, aged > 50, female, the privately insured, and those at teaching hospitals [5] | Epidemiological data showing these groups are more likely to undergo and benefit from interval colectomy |
| Chronic fistula | Colovesical or colovaginal fistula will not close spontaneously — requires surgical resection |
| Chronic stricture causing obstruction | Fibrotic stricture will not resolve with antibiotics — needs resection |
Recurrent episodes of uncomplicated diverticulitis — this is NO LONGER an automatic indication for surgery [3]
"Outcomes of > 2 episodes of attacks are not worse" [5]
"85% do not recur after initial medical treatment" [5]
- Old teaching: after 2 episodes of uncomplicated diverticulitis, patients should undergo elective colectomy (the "2-strike rule") because it was believed the risk of complications increased with each recurrence
- Current evidence: this has been disproven. The risk of complications does NOT significantly increase with recurrent uncomplicated episodes. Most patients (85%) will not have a recurrence after successful medical treatment of their first episode [3][5]
- Current practice: decision for surgery is based on the severity of episodes and patient factors (complications, immunosuppression, inability to exclude malignancy), NOT simply the number of episodes
Recurrence rate: 10–30% in the first decade after initial attack [5]
Elective interval colectomy: not related to recurrence episodes [5]
The 2-Strike Rule Is Dead
This is a very commonly tested concept. The old "2 attacks = surgery" rule is outdated. Modern guidelines (AGA 2015, ASCRS 2020) recommend surgery based on disease severity and patient factors, not simply the number of episodes. Know this for your exam — it's a favourite trap question.
- Sigmoid colectomy with primary anastomosis (1-stage procedure)
- Can be performed laparoscopically (preferred — less morbidity, faster recovery, fewer adhesions)
- Same resection margin principles: proximal = soft uninflamed colon; distal = upper rectum
- No stoma needed (bowel is not inflamed/contaminated at the time of elective surgery)
8. Management of Specific Complications
| Size / Response | Management |
|---|---|
| Small ( < 5 cm) | IV antibiotics alone — likely to resolve [4] |
| Large ( ≥ 5 cm) | CT-guided percutaneous drainage + IV antibiotics [4][5] |
| Failed drainage / persistent sepsis | Emergency surgery (resection ± stoma) [3][5] |
Why CT-guided drainage works: inserting a drain directly into the abscess cavity under CT guidance achieves source control — the pus is evacuated, the bacterial load is dramatically reduced, and antibiotics can then sterilise the residual infection. This often converts what would have been an emergency operation into a controlled situation amenable to interval elective surgery.
- Colovesical fistula (most common): Resection of affected colon + omental pedicle interposition between bowel and bladder (to prevent recurrent fistulation) + synchronous repair of bladder (primary closure) [4]
- Colovaginal fistula: resection of affected colon + primary closure or repair of vaginal defect
- Coloenteric / colocutaneous fistula: resection of affected colon ± repair of secondary organ
- Management principle: control sepsis first (antibiotics, drainage), then definitive surgery — resection of the fistula-bearing colon with repair of the secondarily involved organ [3]
Fistula is usually managed at the index operation with resection of the affected segment of colon [3]
| Type | Mechanism | Management |
|---|---|---|
| Partial obstruction (acute) | Pericolonic inflammation/oedema or compression by abscess → luminal narrowing | Conservative: bowel rest, IV fluids, NG decompression, IV antibiotics → usually resolves with resolution of inflammation |
| Complete obstruction (chronic) | Recurrent diverticulitis → progressive fibrosis → stricture | May require endoscopic stenting as a bridge to surgery, or direct surgical resection. Hartmann's in emergency; primary anastomosis with on-table lavage if stable |
| SBO from adhesion | Small bowel adheres to inflamed sigmoid colon | Standard SBO management: drip and suck → surgical adhesiolysis if not resolving |
Emergency surgery — the management depends on Hinchey stage:
- Hinchey III: Hartmann's procedure OR primary anastomosis with defunctioning stoma OR laparoscopic lavage (in selected cases)
- Hinchey IV: Hartmann's procedure with on-table peritoneal lavage [4]
9. Management of Diverticular Bleeding
| Action | Details |
|---|---|
| IV access | Two large-bore (16G or 14G) peripheral cannulae |
| IV fluids | Rapid bolus of isotonic crystalloid (NS or Hartmann's) |
| Blood transfusion | Transfuse if Hb < 7 g/dL (low-risk) or < 9 g/dL (high-risk, e.g., elderly, IHD) [3] |
| Cross-match | Group and save; cross-match 4–6 units packed RBCs |
| Correct coagulopathy | FFP for coagulopathy; platelets if thrombocytopaenic; withhold anticoagulants/antiplatelets (weigh against thrombotic risk) [3] |
| Monitoring | Vital signs, urine output, cardiac monitoring |
Investigation: Colonoscopy. Management: Conservative → Endoscopic haemostasis → Angiogram ± embolisation [5]
| Step | Modality | Details |
|---|---|---|
| 1st line | Conservative [5] | 50% of diverticular bleeding stops spontaneously [4]. Observe with ongoing resuscitation |
| 2nd line | Colonoscopy with endoscopic haemostasis [5] | Identify the bleeding diverticulum and achieve haemostasis: adrenaline injection (1:10,000) (vasoconstriction — NOT used alone) + metallic clips or band ligation (mechanical compression of the bleeding vessel) [3][4] |
| 3rd line | Mesenteric angiography ± embolisation [5] | When colonoscopy fails to localise or control bleeding. Selective catheterisation of the bleeding artery → superselective embolisation (coils, gelfoam). Detects bleeding > 1 mL/min [3] |
| 4th line | On-table lavage with intraoperative colonoscopy | Bowel lavage through a caecostomy/appendicostomy during laparotomy → colonoscopy to identify bleeding source intraoperatively [4] |
| Last resort | Subtotal colectomy + ileostomy [4] | When the bleeding source cannot be identified despite all the above. Removing the entire colon eliminates the source regardless of location. Significant morbidity — reserved as a life-saving measure |
Localisation of bleeding: colonoscopy → angiography → on-table lavage and colonoscopy → subtotal colectomy and ileostomy [4]
| Indication | Rationale |
|---|---|
| Haemodynamically unstable despite adequate resuscitation | Ongoing arterial haemorrhage exceeding the body's compensatory capacity |
| Excessive blood transfusion > 6 units | Massive transfusion carries its own complications (hypothermia, coagulopathy, hyperkalaemia, citrate toxicity) — continued bleeding requiring this much blood warrants definitive surgical control |
| Frequent rebleeding or persistent bleeding | Endoscopic/angiographic measures have failed to achieve durable haemostasis |
Right-sided (caecal) diverticulitis deserves special mention because it is more common in Asian populations and is managed differently:
| Feature | Approach |
|---|---|
| Uncomplicated right-sided diverticulitis | Conservative management with IV antibiotics (same principles as left-sided) |
| Complicated / recurrent right-sided diverticulitis | Right hemicolectomy (NOT Hartmann's — Hinchey classification does not apply to right-sided disease) |
| Diagnostic challenge | CT abdomen to distinguish from acute appendicitis (see DDx section) |
| Scenario | Management |
|---|---|
| Asymptomatic diverticulosis | Conservative: high-fibre diet, bulk laxatives, weight reduction. Avoid NSAIDs and stimulant laxatives |
| SUDD | Conservative + antispasmodics for colicky pain |
| Uncomplicated diverticulitis (outpatient) | PO antibiotics 7–10 days (Augmentin, or metronidazole + co-trimoxazole/ciprofloxacin, or moxifloxacin) |
| Uncomplicated diverticulitis (inpatient) | IV antibiotics (pip-taz OR metronidazole + cephalosporin/fluoroquinolone) + bowel rest |
| Hinchey I | IV antibiotics ± CT-guided drainage |
| Hinchey II | IV antibiotics + CT-guided percutaneous drainage |
| Hinchey III | Emergency surgery: Hartmann's / primary anastomosis + defunctioning stoma / laparoscopic lavage |
| Hinchey IV | Emergency surgery: Hartmann's procedure |
| Diverticular bleeding | Resuscitate → conservative (50% self-limiting) → colonoscopy (endoscopic haemostasis) → angiography ± embolisation → surgery |
| Fistula | Elective resection of affected colon + repair of secondary organ |
| Stricture/obstruction | Elective resection if chronic; emergency surgery if acute complete obstruction |
| Interval colectomy | For complicated diverticulitis history, immunocompromised, inability to exclude malignancy. NOT for recurrent uncomplicated episodes |
High Yield Summary
Asymptomatic diverticulosis: conservative only — high-fibre diet, bulk laxatives (NOT stimulant laxatives), avoid NSAIDs, weight loss.
Uncomplicated diverticulitis: antibiotics covering GN aerobes + anaerobes (outpatient: Augmentin or metronidazole + ciprofloxacin; inpatient: piperacillin-tazobactam or metronidazole + cephalosporin). Colonoscopy at 6–8 weeks to exclude CRC.
Complicated diverticulitis by Hinchey stage: I–II = IV antibiotics + CT-guided drainage; III–IV = emergency surgery. Hartmann's procedure is the most commonly performed emergency operation (2-stage: resection + end colostomy → later reversal).
Primary anastomosis is contraindicated in Hinchey III–IV due to risk of anastomotic leak in the contaminated/inflamed field.
Laparoscopic lavage is feasible for Hinchey III but remains controversial.
Inadequate distal resection margin is the MC cause of recurrent diverticulitis post-surgery — always resect down to the upper rectum.
The "2-strike rule" is dead: recurrent uncomplicated diverticulitis alone is NOT an indication for surgery. 85% do not recur after initial medical treatment.
Diverticular bleeding: 80% self-limiting. Stepwise escalation: conservative → colonoscopy (clips/adrenaline) → angiography ± embolisation → on-table lavage → subtotal colectomy if source unidentifiable.
Indications for emergency surgery: free perforation, failed antibiotics, septic shock, generalised peritonitis (Hinchey III–IV), obstruction, abscess failing drainage. Indications for laparotomy in bleeding: haemodynamic instability despite resuscitation, > 6 units transfused, persistent/recurrent bleeding.
Active Recall - Management of Diverticular Disease
References
[1] Lecture slides: Diverticular diseases - Dr. J Tsang.pdf (p8) [2] Lecture slides: GC 195. Lower and diffuse abdominal pain RLQ problems; pelvic inflammatory disease; peritonitis and abdominal emergencies.pdf (p19) [3] Senior notes: felixlai.md (Diverticular disease section — Treatment) [4] Senior notes: maxim.md (Diverticular disease section — Management) [5] Lecture slides: Diverticular diseases - Dr. J Tsang.pdf (p6, p7, p10, p13, p14, p16)
Complications of Diverticular Disease
Understanding complications requires thinking about what happens when a microperforation in the colon wall goes wrong in different ways. Every complication traces back to the same fundamental event — a faecolith obstructs a diverticulum → bacterial overgrowth → mucosal erosion → microperforation — but the downstream consequences differ based on whether the perforation is walled off, tracks to an adjacent organ, causes luminal compromise, or ruptures freely into the peritoneum.
1. Abscess
- Occurs in ~17% of patients with acute diverticulitis [3]
- When a diverticulum microperforates, the body's initial response is to wall off the contamination. The pericolic mesentery, omentum, and fat wrap around the perforation site → creating a phlegmon (inflamed mass) [3]
- If the bacterial load overwhelms local defences, the phlegmon liquefies at its centre → a walled-off collection of pus forms = abscess
- The abscess may remain localised (pericolic, Hinchey I) or track to distant sites:
- Pelvic abscess (Hinchey II) — pus gravitates into the pelvis (the most dependent peritoneal space)
- Psoas abscess — pus tracks along the psoas muscle retroperitoneally (the sigmoid colon lies directly anterior to the left psoas)
- Pyogenic liver abscess — spread of infection through the portal circulation (mesenteric veins drain to the portal vein → liver) [3]. This is a rare but serious complication
- Should be suspected in patients with no improvement in abdominal pain or a persistent fever despite 3 days of antibiotic treatment [3]
- Swinging pyrexia (temperature spikes with intermittent defervescence — classic pattern of undrained abscess)
- Persistent fever and abdominal pain despite antibiotics ± tender mass on PR (pelvic abscess palpable on digital rectal examination) [4]
- Rising WCC and CRP despite treatment
- May present as a palpable tender abdominal mass (phlegmon or large abscess)
This is a practical clinical rule. Appropriately treated uncomplicated diverticulitis should show clinical improvement within 48–72 hours of IV antibiotics (trending down of fever, reducing pain, falling WCC). If there is no improvement by day 3, the antibiotic is either not penetrating the source (suggesting a walled-off collection that needs drainage) or there is a more serious complication.
- CT abdomen + pelvis with IV contrast — demonstrates abscess as a fluid collection with surrounding inflammatory changes containing air, air-fluid levels, or low-attenuation necrotic debris [3][4]
- Abscess size 5 cm is the cut-off: < 5 cm likely resolves with antibiotics alone; ≥ 5 cm requires CT-guided percutaneous drainage [4]
2. Fistula
- Inflammation from diverticulitis causes the inflamed sigmoid colon to adhere to an adjacent organ (bladder, vagina, small bowel, skin, uterus)
- The inflammatory process erodes through both the colonic wall and the wall of the adjacent organ → creating an abnormal communication (fistula = Latin fistula = "pipe" or "tube")
- Fistulae typically develop from a contained microperforation or small abscess that decompresses into the neighbouring structure rather than freely into the peritoneum
| Type | Frequency | Why? | Clinical Features |
|---|---|---|---|
| Colovesical fistula | Most common [3][4] | The sigmoid colon lies directly on the dome of the bladder — anatomical proximity. More common in males because in females the uterus interposes between sigmoid and bladder | Recurrent dysuria, pneumaturia (air bubbles in urine — pathognomonic), faecaluria (faecal particles in urine), recurrent polymicrobial UTIs [4]. Urine culture grows colonic flora (e.g., E. coli, Bacteroides) — essentially diagnostic [3] |
| Colovaginal fistula | Second most common [3] | Especially in post-hysterectomy patients — removal of the uterus eliminates the anatomical barrier between sigmoid and vagina [3] | Vaginal passage of faeces and flatus, foul-smelling vaginal discharge, recurrent vaginal infections |
| Coloenteric fistula | Uncommon [3] | Inflamed sigmoid adheres to adjacent small bowel loop | May be entirely asymptomatic or result in corrosive diarrhoea [3] — small bowel contents are diverted, and colonic bacteria contaminate the small bowel (bacterial overgrowth → malabsorption → diarrhoea) |
| Colocutaneous fistula | Uncommon [3] | Abscess tracks through the abdominal wall to the skin surface | Usually easy to identify — visible external opening with faecal discharge [3] |
- CT colonography with water-soluble rectal contrast — contrast injected rectally is seen tracking into the bladder/vagina/skin [4]
- Cystoscopy — for colovesical fistula: may show bullous oedema, erythema, or the fistula opening on the bladder dome
- Urine culture — growth of mixed colonic flora (multiple Gram-negatives + anaerobes) is essentially pathognomonic for colovesical fistula [3]
- Contrast enema — can delineate the fistula tract [3]
The management principle is: control sepsis first → then definitive surgical repair
- Control sepsis: IV antibiotics + drainage of any associated abscess
- Definitive surgery (usually elective):
- Resection of the affected segment of colon involved with diverticulitis, usually with a primary anastomosis [3]
- Simple repair of the secondarily involved organ — e.g., primary closure of bladder or vagina (may require flap depending on complexity) [3]
- Colovesical fistula: resection of affected colon + omental pedicle interposition between bowel and bladder (to prevent recurrent fistulation) + synchronous repair of bladder [4]
Fistula is usually managed at the index operation with resection of the affected segment of colon [3]
Omental Pedicle Interposition — Why?
After resecting the fistula-bearing colon and repairing the bladder, you place a pedicled flap of omentum between the bowel anastomosis and the bladder repair. The omentum is highly vascularised and has excellent healing properties — it physically separates the two suture lines and reduces the risk of the fistula recurring. The omentum is sometimes called the "policeman of the abdomen" because it migrates to sites of inflammation and promotes healing.
3. Obstruction
There are three distinct mechanisms by which diverticular disease causes intestinal obstruction [3]:
| Mechanism | Type | Pathophysiology |
|---|---|---|
| Acute pericolonic inflammation/oedema | Partial LBO (acute) | Active diverticulitis causes significant pericolic inflammation → the bowel wall becomes oedematous and thickened → relative luminal narrowing. Alternatively, a large pericolic abscess may externally compress the lumen [3] |
| Chronic fibrosis and stricture | Complete LBO (chronic) | Recurrent attacks of acute diverticulitis result in progressive fibrosis and scarring leading to formation of intestinal strictures [3]. Each episode deposits more collagen → progressive narrowing → eventually complete obstruction |
| Adhesions to inflamed bowel | SBO | Inflamed sigmoid colon causes adjacent small bowel loops to adhere to it → kinking or compression of the small bowel → SBO [4] |
| Paralytic ileus | Functional obstruction | Localised peritoneal irritation from pericolic inflammation → reflex sympathetic inhibition of peristalsis → functional obstruction without mechanical cause [3] |
Intestinal obstruction: LBO due to fibrosis and stricture, SBO due to adhesion to inflamed bowel [4]
- Cardinal features of intestinal obstruction (the "4 C's" — colicky pain, constipation, vomiting, and distension):
- Colicky abdominal pain — intermittent cramping as the bowel contracts against the obstruction
- Abdominal distension — proximal bowel dilates with gas and fluid
- Vomiting — initially bilious, late becomes faeculent in LBO
- Absolute constipation (obstipation) — no passage of flatus or stool
- Bowel sounds: hyperactive/tinkling (mechanical obstruction) → later absent (ileus or late obstruction with bowel fatigue)
- AXR: dilated bowel loops with air-fluid levels; in LBO look for dilated colon with no gas in the rectum [4]
- CT abdomen: identifies the transition point, distinguishes mechanical obstruction from pseudo-obstruction, evaluates for ischaemia
- Acute partial obstruction (from inflammation): usually resolves with conservative management (bowel rest, IV fluids, NG decompression, IV antibiotics to treat underlying diverticulitis)
- Complete obstruction from stricture: may require endoscopic stenting as a bridge to surgery or direct surgical resection
- Emergency: Hartmann's procedure if acute complete LBO with ischaemia/perforation signs
- Elective: sigmoid colectomy with primary anastomosis after resolution of acute episode — remove the strictured segment
4. Perforation and Peritonitis
Two mechanisms of free perforation [3]:
- Rupture of a diverticular abscess into the peritoneal cavity → the walled-off collection bursts → purulent peritonitis (Hinchey III)
- Rupture of an inflamed diverticulum with faecal contamination of the peritoneum → faecal peritonitis (Hinchey IV) — this is the most catastrophic outcome
Leads to generalised purulent or faecal peritonitis [3]
Severity ranges from diverticulitis to localised diverticular abscess to purulent peritonitis to faecal peritonitis [5]
| Feature | Pathophysiological Basis |
|---|---|
| Sudden severe abdominal pain | Peritoneal soiling → intense irritation of the parietal peritoneum → somatic pain (sharp, well-localised initially, then generalised) |
| Fever, tenderness and guarding [2] | Systemic inflammatory response to intraperitoneal contamination; reflex abdominal wall muscle contraction (guarding) to protect the inflamed peritoneum |
| Board-like rigidity | Severe generalised peritonitis → diffuse reflex contraction of all abdominal wall muscles → the abdomen becomes "hard as a board" |
| Rebound tenderness | Sudden release of pressure stretches the inflamed parietal peritoneum → sharp pain |
| Absent bowel sounds | Generalised peritoneal inflammation → complete cessation of peristalsis (generalised paralytic ileus) |
| Septic shock: high fever, tachycardia, hypotension, oliguria [5] | Massive systemic inflammatory response → vasodilation (↓SVR), capillary leak, third-spacing → distributive shock → impaired organ perfusion (oliguria = acute kidney injury, altered mental state = cerebral hypoperfusion) |
| Pneumoperitoneum on CXR | Free intraperitoneal air from bowel perforation |
Resuscitation with IVF + antibiotics. Percutaneous drainage for abscess. Consider emergency surgery [5]
Unresponsive to antibiotics, septic shock, generalised peritonitis (III and IV) → emergency surgery [5]
- Resuscitation: IV access, crystalloid fluid boluses, broad-spectrum IV antibiotics (piperacillin-tazobactam or metronidazole + cephalosporin), oxygen, urinary catheter, arterial line/central venous access if shocked
- Emergency surgery: Hartmann's procedure (resection + end colostomy + rectal stump closure) is the standard for Hinchey III–IV [4][5]. Primary anastomosis is contraindicated in the setting of diffuse contamination and inflammation due to high risk of anastomotic leak [4]
- On-table peritoneal lavage: copious warm saline irrigation of the peritoneal cavity to reduce bacterial load
5. Diverticular Bleeding
- When a diverticulum herniates, the vasa recta is draped over the dome → blood vessel is separated from the bowel lumen only by mucosa → eccentric intimal thickening and medial thinning → segmental arterial weakness → rupture into bowel lumen [3]
- Right colon is usually the source because right-sided diverticula have wider necks/domes and the colonic wall is thinner → more vasa recta length exposed to injury [3]
- Bleeding occurs in the ABSENCE of diverticulitis — the two processes are separate (inflammation causes fibrosis of vasa recta, which paradoxically protects against bleeding) [3]
- Common cause of severe GI bleeding [1]
- Intermittent bleeding [1]
- Painless massive PR bleeding — haematochezia (bright red to maroon blood per rectum)
- 80% self-limiting [1] — arterial spasm and clot formation at the rupture site
- Rebleeding rate ~20–30% [7]
- Can cause haemodynamic instability if blood loss is massive (tachycardia, hypotension, pallor, altered consciousness)
Conservative → Endoscopic haemostasis → Angiogram ± embolisation [1][5]
- Resuscitation: IV access, crystalloids, blood transfusion, correct coagulopathy
- 50% of bleeding stops spontaneously [4] → conservative observation with ongoing monitoring
- Colonoscopy: endoscopic haemostasis with adrenaline injection + metallic clips [3][4][5]
- Mesenteric angiography ± embolisation: when colonoscopy fails [3]
- On-table lavage + intraoperative colonoscopy: when angiography fails
- Subtotal colectomy + ileostomy: last resort when the bleeding source cannot be identified [4]
| Indication | Rationale |
|---|---|
| Haemodynamically unstable despite adequate resuscitation | Ongoing arterial haemorrhage exceeding compensatory capacity |
| Excessive blood transfusion > 6 units | Massive transfusion carries its own risks (hypothermia, coagulopathy, hyperkalaemia) |
| Frequent rebleeding or persistent bleeding | Endoscopic/angiographic measures have failed |
6. Complications of Surgical Treatment
When patients undergo surgery for diverticular disease (whether emergency Hartmann's or elective sigmoid colectomy), they face procedure-specific complications:
| Complication | Timing | Features | Management |
|---|---|---|---|
| Anastomotic bleeding | Early ( < 30 days) | PR bleeding, dropping Hb | Blood transfusion, correct coagulopathy; rarely requires re-operation |
| Anastomotic leak | Early ( < 30 days, typically day 5–7) | Suspect if any deviation from normal post-op course: pain, fever, tachycardia, prolonged ileus, feculent/purulent drainage [4] | Fluid resuscitation, broad-spectrum IV antibiotics, NPO. Minor leak: CT-guided percutaneous drainage. Major leak: re-laparotomy → takedown of anastomosis + proximal diversion stoma [4] |
| Anastomotic stricture | Late ( > 30 days) | Progressive narrowing → constipation, obstructive symptoms | Majority do not require intervention. If symptomatic: endoscopic balloon dilatation [3] |
Inadequate distal margin is the MC cause of recurrent diverticulitis after resection [4] — if you leave any sigmoid colon behind (rather than anastomosing to the upper rectum), the residual high-pressure sigmoid will develop recurrent diverticulitis
| Timing | Complication | Mechanism |
|---|---|---|
| Early ( < 30 days) | Stomal bleeding | Mucocutaneous junction trauma or mesenteric vessel injury |
| Stomal necrosis | Ischaemia of the exteriorised bowel from inadequate blood supply or excessive tension on the mesentery | |
| Stomal retraction | Tension on the mesentery pulls the stoma below skin level → poor appliance fitting → faecal leak and skin excoriation | |
| Mucocutaneous separation | Separation of the bowel from the surrounding skin sutures → peristomal wound | |
| Skin irritation/dermatitis | Effluent contact dermatitis — worse with ileostomy (high-output, alkaline enzymatic effluent) than colostomy | |
| Late ( > 30 days) | Parastomal hernia | Weakness of the abdominal wall around the stoma site → peritoneal sac + bowel herniates through the defect. Risk factors: end stoma, emergency surgery, obesity |
| Stomal prolapse | Intussusception of bowel through the stoma → visible protrusion. MC in loop transverse colostomy. Risk of ischaemia/necrosis | |
| Stomal stenosis | Scarring and fibrosis at the mucocutaneous junction → narrowing of the stoma opening → obstructive symptoms |
| Complication | Explanation |
|---|---|
| Rectal stump leak | The oversewn rectal stump may dehisce → pelvic abscess/sepsis. This is why some surgeons bring the distal end out as a mucous fistula rather than closing it intra-abdominally (particularly if the tissues are severely inflamed) |
| Rectal stump abscess | Infected haematoma or seroma at the closed rectal stump |
| Ureteric injury | The left ureter runs very close to the sigmoid colon mesentery → at risk during dissection, especially in emergency surgery with distorted anatomy |
| Non-reversal | Up to 30–40% of Hartmann's procedures are never reversed — due to patient comorbidities, adhesions, or patient preference. The patient lives with a permanent end colostomy |
While not strictly a "complication" of diverticulitis, SCAD is an important entity that can complicate the clinical picture:
- Pathophysiology: Chronic mucosal inflammation in the interdiverticular mucosa (between diverticula) — the diverticular orifices themselves are spared
- Why it occurs: Likely related to mucosal prolapse, altered microbiome, and chronic low-grade inflammation in diverticular segments; possibly a form of localised IBD
- Clinical features: Chronic bloody diarrhoea, LLQ pain — can mimic IBD
- Diagnosis: Colonoscopy with biopsy shows mucosal inflammation between diverticula with sparing of diverticular orifices
- Management: 5-ASA (mesalazine) ± topical steroids; rarely requires surgery. Usually self-limiting
| Outcome | Data |
|---|---|
| Recurrence after initial medical treatment | 85% do NOT recur [5] |
| Recurrence rate | 10–30% in the first decade after initial attack [5] |
| Outcomes of > 2 episodes | Not worse than single episode [5] — this is why the "2-strike rule" for surgery is obsolete |
| Risk of complicated disease on recurrence | Patients who present with uncomplicated diverticulitis on their first episode tend to present with uncomplicated disease on recurrence (the disease pattern is established early) |
| Mortality by Hinchey stage | I = 0%, II = 5%, III = 25%, IV = 50% [4] |
| Complication | Incidence / Frequency | Key Clinical Clue | Key Investigation | Management |
|---|---|---|---|---|
| Abscess | ~17% of acute diverticulitis | Persistent fever/pain despite 3 days antibiotics; tender mass on PR | CT: fluid collection with inflammatory surround | IV Abx ± CT-guided drainage; surgery if fails |
| Fistula (MC: colovesical) | Most common in males | Pneumaturia, faecaluria, recurrent UTI | CT colonography; urine culture (colonic flora) | Elective resection + repair of secondary organ + omental interposition |
| Obstruction | Variable | Colicky pain, distension, vomiting, constipation | CT: transition point, dilated proximal bowel | Conservative if acute/partial; surgery if complete or chronic stricture |
| Perforation / Peritonitis | Hinchey III–IV | Acute abdomen, rigidity, absent bowel sounds, septic shock | CXR: pneumoperitoneum; CT: free air/fluid | Emergency surgery (Hartmann's) |
| Diverticular Bleeding | ~15–55% of LGIB | Painless massive PR bleed, 80% self-limiting | Colonoscopy, angiography, Tc-RBC scan | Conservative → endoscopic → angiographic → surgical |
| Recurrence | 10–30% in first decade | Recurrent LLQ/RLQ pain with fever | CT | Same as initial episode; surgery only for complicated disease |
High Yield Summary
Abscess (17% of diverticulitis): suspect if no improvement after 3 days antibiotics. May cause pyogenic liver abscess via portal circulation. CT-guided drainage if ≥ 5 cm.
Fistula: MC = colovesical (pneumaturia, faecaluria, recurrent UTI) — more common in males. Colovaginal is second (especially post-hysterectomy). Management: resection of affected colon + repair of secondary organ + omental pedicle interposition.
Obstruction: LBO from chronic fibrotic stricture (recurrent diverticulitis → progressive fibrosis); SBO from adhesion to inflamed bowel; paralytic ileus from peritoneal irritation.
Perforation/Peritonitis: Hinchey III (purulent, abscess rupture, bowel intact) = 25% mortality; Hinchey IV (faecal, bowel wall perforation) = 50% mortality. Emergency Hartmann's procedure.
Diverticular bleeding: commonest cause of severe LGIB. Painless, arterial (vasa recta rupture), 80% self-limiting. Right colon is the usual source. Stepwise: conservative → colonoscopy → angiography → surgery.
Recurrence: 85% do not recur after initial medical treatment. 10–30% recurrence in the first decade. Outcomes after > 2 episodes are NOT worse — the "2-strike rule" is dead.
Inadequate distal resection margin is the MC cause of recurrent diverticulitis after surgery — always resect to the upper rectum.
Surgical complications: anastomotic leak (day 5–7, suspect if any post-op deviation), stoma complications (early: necrosis, retraction; late: parastomal hernia, prolapse), Hartmann's-specific (rectal stump leak, ureteric injury, 30–40% non-reversal rate).
Active Recall - Complications of Diverticular Disease
References
[1] Lecture slides: Diverticular diseases - Dr. J Tsang.pdf (p8, p13) [2] Lecture slides: GC 195. Lower and diffuse abdominal pain RLQ problems; pelvic inflammatory disease; peritonitis and abdominal emergencies.pdf (p19) [3] Senior notes: felixlai.md (Diverticular disease section — Complications, Treatment) [4] Senior notes: maxim.md (Diverticular disease section — Investigations, Management, Hartmann's operation) [5] Lecture slides: Diverticular diseases - Dr. J Tsang.pdf (p13, p16) [7] Lecture slides: GC 186. Lower and diffuse abdominal painfresh blood in stool.pdf (p9)
High Yield Summary
Definition: Diverticula = outpouchings of bowel wall; diverticulosis = presence of diverticula; diverticular disease = symptomatic diverticulosis (diverticulitis, bleeding, SUDD).
True vs False: Right-sided = true (congenital, all layers); Left-sided = false (acquired, mucosa + submucosa only).
Epidemiology: 60% prevalence by age 70; 80% asymptomatic; left-sided predominant in West; right-sided more common in Asia → caecal diverticulitis mimics appendicitis → CT is key.
Risk factors: Age, low-fibre diet, obesity, sedentary lifestyle, NSAIDs, steroids, opiates, connective tissue disease.
Pathogenesis: Wall weakness (vasa recta penetration points) + increased intraluminal pressure (Laplace's law, sigmoid narrowest calibre) → diverticula. Diverticulitis = faecolith obstruction → microperforation. Bleeding = vasa recta rupture (separate from inflammation).
Hinchey Classification (NOT for right-sided): I = pericolic abscess (0% mortality); II = pelvic abscess (5%); III = purulent peritonitis (25%); IV = faecal peritonitis (50%).
Clinical triad of diverticulitis: Lower abdominal pain + fever + leucocytosis. LLQ in West, RLQ in Asia.
Diverticular bleeding: Painless, massive, self-limiting (80%), right colon is the usual source.
Complications: Abscess, perforation/peritonitis, fistula (MC = colovesical → pneumaturia, faecaluria), obstruction (LBO from stricture, SBO from adhesion).
Rectum never affected: Full circumferential longitudinal muscle coat.
High Yield Summary
The single most important DDx across all presentations is colorectal cancer (CRC) — always exclude it. Colonoscopy at 6–8 weeks post-acute diverticulitis is mandatory.
Right-sided diverticulitis mimics acute appendicitis — CT abdomen is the key differentiator, especially in Asian populations including Hong Kong.
Diverticular bleeding DDx: angiodysplasia, severe colitis, rectal ulcer, small bowel bleeding, UGIB. Don't forget massive UGIB can present as haematochezia.
In women of reproductive age: always exclude ectopic pregnancy (β-hCG) and gynaecological causes (TOA, ovarian torsion, PID) before diagnosing diverticular disease.
Meckel's diverticulitis presents similarly to appendicitis; may be an incidental finding during appendicectomy; diagnosed by CT.
Ischaemic colitis has rapid onset + haematochezia (vs. gradual onset + constant pain in diverticulitis).
IBD and infectious colitis: diarrhoea predominates (vs. pain predominates in diverticulitis).
High Yield Summary
The diagnosis of acute diverticulitis is clinico-radiological: clinical triad (lower abdominal pain + fever + leucocytosis) confirmed by CT abdomen + pelvis with IV contrast (gold standard).
CT is diagnostic, assesses complications, aids treatment (guides drainage), and is prognostic (Hinchey staging).
Key CT findings: bowel wall thickening > 4 mm, pericolic fat stranding, visible diverticula. Complications: abscess (5 cm cut-off for drainage), fistula (extracolonic air in adjacent organs), obstruction (dilated loops), perforation (free air).
CT distinguishes diverticulitis from CRC: diverticulitis involves > 10 cm, has prominent fat stranding, no enlarged lymph nodes. CRC has short-segment involvement, shouldering, and lymphadenopathy.
Colonoscopy is CONTRAINDICATED acutely (risk of perforation). Colonoscopy at 6–8 weeks post-recovery is mandatory to exclude CRC — malignancy rate in complicated diverticulitis is ~10-17%.
Diverticular bleeding investigation: colonoscopy (first-line) → mesenteric angiography → on-table lavage and colonoscopy → subtotal colectomy if source not found.
Sterile pyuria on urinalysis = adjacent inflammation. Colonic flora on urine culture = colovesical fistula.
Hinchey classification is NOT applicable to right-sided disease.
High Yield Summary
Asymptomatic diverticulosis: conservative only — high-fibre diet, bulk laxatives (NOT stimulant laxatives), avoid NSAIDs, weight loss.
Uncomplicated diverticulitis: antibiotics covering GN aerobes + anaerobes (outpatient: Augmentin or metronidazole + ciprofloxacin; inpatient: piperacillin-tazobactam or metronidazole + cephalosporin). Colonoscopy at 6–8 weeks to exclude CRC.
Complicated diverticulitis by Hinchey stage: I–II = IV antibiotics + CT-guided drainage; III–IV = emergency surgery. Hartmann's procedure is the most commonly performed emergency operation (2-stage: resection + end colostomy → later reversal).
Primary anastomosis is contraindicated in Hinchey III–IV due to risk of anastomotic leak in the contaminated/inflamed field.
Laparoscopic lavage is feasible for Hinchey III but remains controversial.
Inadequate distal resection margin is the MC cause of recurrent diverticulitis post-surgery — always resect down to the upper rectum.
The "2-strike rule" is dead: recurrent uncomplicated diverticulitis alone is NOT an indication for surgery. 85% do not recur after initial medical treatment.
Diverticular bleeding: 80% self-limiting. Stepwise escalation: conservative → colonoscopy (clips/adrenaline) → angiography ± embolisation → on-table lavage → subtotal colectomy if source unidentifiable.
Indications for emergency surgery: free perforation, failed antibiotics, septic shock, generalised peritonitis (Hinchey III–IV), obstruction, abscess failing drainage. Indications for laparotomy in bleeding: haemodynamic instability despite resuscitation, > 6 units transfused, persistent/recurrent bleeding.
High Yield Summary
Abscess (17% of diverticulitis): suspect if no improvement after 3 days antibiotics. May cause pyogenic liver abscess via portal circulation. CT-guided drainage if ≥ 5 cm.
Fistula: MC = colovesical (pneumaturia, faecaluria, recurrent UTI) — more common in males. Colovaginal is second (especially post-hysterectomy). Management: resection of affected colon + repair of secondary organ + omental pedicle interposition.
Obstruction: LBO from chronic fibrotic stricture (recurrent diverticulitis → progressive fibrosis); SBO from adhesion to inflamed bowel; paralytic ileus from peritoneal irritation.
Perforation/Peritonitis: Hinchey III (purulent, abscess rupture, bowel intact) = 25% mortality; Hinchey IV (faecal, bowel wall perforation) = 50% mortality. Emergency Hartmann's procedure.
Diverticular bleeding: commonest cause of severe LGIB. Painless, arterial (vasa recta rupture), 80% self-limiting. Right colon is the usual source. Stepwise: conservative → colonoscopy → angiography → surgery.
Recurrence: 85% do not recur after initial medical treatment. 10–30% recurrence in the first decade. Outcomes after > 2 episodes are NOT worse — the "2-strike rule" is dead.
Inadequate distal resection margin is the MC cause of recurrent diverticulitis after surgery — always resect to the upper rectum.
Surgical complications: anastomotic leak (day 5–7, suspect if any post-op deviation), stoma complications (early: necrosis, retraction; late: parastomal hernia, prolapse), Hartmann's-specific (rectal stump leak, ureteric injury, 30–40% non-reversal rate).
YouTube Video Reference
Colorectal Cancer
Colorectal cancer is a malignant neoplasm arising from the epithelial lining of the colon or rectum, typically developing through an adenoma-to-carcinoma sequence.
Hemorrhoids
Hemorrhoids are dilated vascular cushions of the anal canal that become symptomatic when swollen, inflamed, or prolapsed, causing bleeding, pain, or pruritus.