Pancreatic Cancer
Pancreatic cancer is a highly aggressive malignancy most commonly arising from the exocrine ductal epithelium of the pancreas, often presenting late with obstructive jaundice, weight loss, and pain, carrying a poor prognosis.
Pancreatic cancer refers to malignant neoplasms arising from the pancreas. The overwhelming majority (> 95%) are exocrine tumours, and of those, > 85% are pancreatic ductal adenocarcinoma (PDAC) — the "classic" pancreatic cancer we worry about clinically [1][2]. The word itself is straightforward: "pancreatic" = of the pancreas (Greek pan = all, kreas = flesh/meat — so named because the gland is "all flesh" with no bone or cartilage), and "carcinoma" (Greek karkinos = crab) denotes an epithelial malignancy.
Unless otherwise specified, "pancreatic cancer" in clinical practice and in exams almost always refers to pancreatic ductal adenocarcinoma (PDAC).
Other exocrine histological subtypes (much rarer) include:
- Squamous cell carcinoma
- Acinar cell carcinoma
- Undifferentiated (anaplastic) carcinoma
- Pancreatoblastoma (rare, mainly paediatric)
- Adenosquamous carcinoma
Endocrine (neuroendocrine) pancreatic tumours (e.g., insulinoma, gastrinoma) account for < 5% of pancreatic malignancies and have a fundamentally different biology, treatment, and prognosis [1][2].
Periampullary cancers — a group of cancers arising around the ampulla of Vater — include pancreatic head cancer, ampullary carcinoma, distal cholangiocarcinoma, and duodenal carcinoma. They all present similarly (painless obstructive jaundice) but have different prognoses. Ampullary carcinoma has the best prognosis (5-year survival ~40–60%), while PDAC has the worst (~10%) [3].
High Yield Concept
Painless progressive obstructive jaundice is the hallmark presentation of pancreatic head cancer — it is the single most important clinical clue. The differential for painless jaundice with a palpable gallbladder (Courvoisier's sign) is essentially periampullary malignancy until proven otherwise [3][4].
2. Epidemiology
- Pancreatic cancer is the 7th leading cause of cancer death worldwide and one of the most lethal solid malignancies.
- Incidence is rising globally.
- 5-year overall survival remains dismal: ~10–12% across all stages (one of the lowest of any cancer).
- Median age at diagnosis: ~70 years — it is predominantly a disease of the elderly [1][2].
- Slight male predominance (M:F ≈ 1.3:1) [1].
- Pancreatic cancer is the 5th most common cause of cancer death in Hong Kong (2022 data from the Hong Kong Cancer Registry).
- Incidence has been steadily increasing, likely related to ageing population, rising obesity, and diabetes prevalence.
- Annual incidence: approximately 900–1000 new cases/year in Hong Kong.
- Because Hong Kong has a high prevalence of hepatitis B-related HCC and cholangiocarcinoma, pancreatic cancer must be distinguished from other hepatobiliary malignancies presenting with jaundice.
| Feature | Detail |
|---|---|
| Peak incidence | 60–80 years |
| Sex | Male > Female (1.3:1) |
| 5-year survival (all stages) | ~10–12% |
| 5-year survival (resected, node-negative) | 25–30% |
| 5-year survival (resected, node-positive) | ~10% |
| Median survival (unresectable locally advanced) | ~12 months |
| Median survival (metastatic) | ~6 months |
| % diagnosed at localized stage | Only ~8% |
| % diagnosed with distant metastases | ~53% (majority) |
The reason the prognosis is so poor is multifactorial:
- Late presentation — the retroperitoneal location means symptoms appear late.
- Aggressive biology — dense desmoplastic stroma, early perineural/vascular invasion, early micrometastases.
- Chemoresistance — the dense stroma acts as a drug delivery barrier.
Why is pancreatic cancer so deadly?
Think of it as "the perfect storm": located deep in the retroperitoneum (so symptoms come late), surrounded by major vessels (SMA, SMV, celiac axis, portal vein — so even small tumours become unresectable), biologically aggressive (early neural/lymphovascular invasion), and wrapped in dense fibrotic stroma (which shields tumour cells from chemotherapy and immune cells).
3. Risk Factors
| Risk Factor | Explanation |
|---|---|
| Advanced age | Cumulative somatic mutations over time; peak incidence 60–80 years |
| Male sex | Slight male predominance, possibly related to higher rates of smoking and alcohol use historically [1] |
| Non-O blood group (A, B, AB) | ABO blood group antigens are expressed on pancreatic ductal epithelium; non-O groups have ~30% increased risk. The mechanism is not fully elucidated but may relate to altered inflammatory/immune signaling via ABO glycosyltransferases |
| Family history (1st-degree relative) | 2-fold increased risk with one affected 1st-degree relative; risk increases further with more affected relatives |
| Hereditary cancer syndromes | See below |
| Race/Ethnicity | Higher incidence in Black populations (globally); in HK, this is less relevant |
Approximately 5–10% of pancreatic cancers have a hereditary component. Key syndromes:
| Syndrome | Gene | Key Associations |
|---|---|---|
| Hereditary breast-ovarian cancer (HBOC) | BRCA1, BRCA2 | BRCA2 carriers have ~3.5-fold increased risk of pancreatic cancer; BRCA1 has a smaller but real increase [5][6] |
| Lynch syndrome (HNPCC) | MMR genes (MLH1, MSH2, MSH6, PMS2) | Autosomal dominant; ↑ risk of colorectal, endometrial, ovarian, and pancreatic cancer |
| Peutz-Jeghers syndrome | STK11/LKB1 | ~130-fold increased risk of pancreatic cancer; mucocutaneous pigmentation + GI hamartomatous polyps |
| Familial atypical multiple mole melanoma (FAMMM) | CDKN2A (p16) | Multiple atypical naevi + melanoma + ↑ pancreatic cancer risk (13–22-fold) |
| Hereditary pancreatitis | PRSS1, SPINK1, CFTR | Recurrent pancreatitis from childhood → chronic pancreatitis → malignant transformation (~40% lifetime risk by age 70) |
| Li-Fraumeni syndrome | TP53 | Multiple cancers including pancreatic |
| Familial pancreatic cancer | PALB2, ATM, and others | ≥2 first-degree relatives with PDAC without an identified syndrome |
BRCA2 and Pancreatic Cancer
BRCA2 is the most common identifiable germline mutation in familial pancreatic cancer. This is clinically important because BRCA-mutated PDAC responds to platinum-based chemotherapy and PARP inhibitors (e.g., olaparib — maintenance after platinum-based chemo in metastatic disease, based on the POLO trial). The lecture slide on BRCA2 specifically notes: "Increased risk of prostate, laryngeal, bile duct, stomach, colon (minimal), melanoma and pancreatic cancers (~1.5–3 fold risk)" [5].
| Risk Factor | Mechanism / Explanation |
|---|---|
| Smoking | ~3× increased risk [2]; most important modifiable risk factor. Tobacco carcinogens (nitrosamines, polycyclic aromatic hydrocarbons) reach the pancreas via bloodstream and reflux into the pancreatic duct. Dose-dependent; risk decreases after cessation but takes ~10–20 years to normalize |
| Chronic pancreatitis | Chronic inflammation → repeated injury-repair cycles → accumulation of somatic mutations → malignant transformation. ~2% lifetime risk of pancreatic cancer in chronic pancreatitis patients [2][7] |
| Diabetes mellitus | Complex bidirectional relationship: (1) Long-standing T2DM is a modest risk factor (~1.5–2× risk), likely via insulin resistance/hyperinsulinemia promoting growth; (2) New-onset diabetes (within 1–3 years) can be the FIRST manifestation of occult pancreatic cancer — the tumour produces diabetogenic factors (e.g., adrenomedullin, S100A8 calcium-binding protein) that impair β-cell function [1] |
| Obesity | BMI > 30 increases risk by ~20–40%; central adiposity is particularly important. Mechanisms: chronic low-grade inflammation, insulin resistance, altered adipokine signaling |
| Physical inactivity | Related to obesity and insulin resistance pathway |
| Heavy alcohol use | Primarily through causing chronic pancreatitis; independent modest risk factor at very high consumption levels |
| Dietary factors | High saturated fat/protein, processed meat, low fruit/vegetable intake. Western-type diet increases risk |
| Pancreatic cysts (premalignant) | Intraductal papillary mucinous neoplasm (IPMN) is the most important neoplastic cyst with malignant potential: main-duct IPMN has ~60–70% risk of harbouring malignancy vs. branch-duct IPMN which is lower risk [7][8] |
Pancreatic cancer develops through a well-characterised stepwise progression:
- PanIN = Pancreatic Intraepithelial Neoplasia (the most common precursor lesion)
- PanIN-1: flat (1A) or papillary (1B) mucinous epithelium; KRAS mutation present in >90%
- PanIN-2: moderate dysplasia; p16/CDKN2A inactivation
- PanIN-3: carcinoma in situ; TP53 and SMAD4/DPC4 loss
- Other precursor lesions: IPMN and mucinous cystic neoplasm (MCN)
The 'Big Four' Genetic Drivers of PDAC
- KRAS (oncogene activation) — present in > 90% of PDAC, the earliest and most universal driver
- CDKN2A/p16 (tumour suppressor loss) — ~90%
- TP53 (tumour suppressor loss) — ~75%
- SMAD4/DPC4 (tumour suppressor loss) — ~55%; loss correlates with widespread metastatic disease
These accumulate in sequence during the PanIN → PDAC progression.
4. Anatomy and Function
Understanding the anatomy is absolutely critical for appreciating why pancreatic cancer presents the way it does and why surgery is so complex.
The pancreas is a retroperitoneal organ lying transversely across the posterior abdominal wall at the level of L1–L2. It is approximately 15–20 cm long and weighs ~80–100 g.
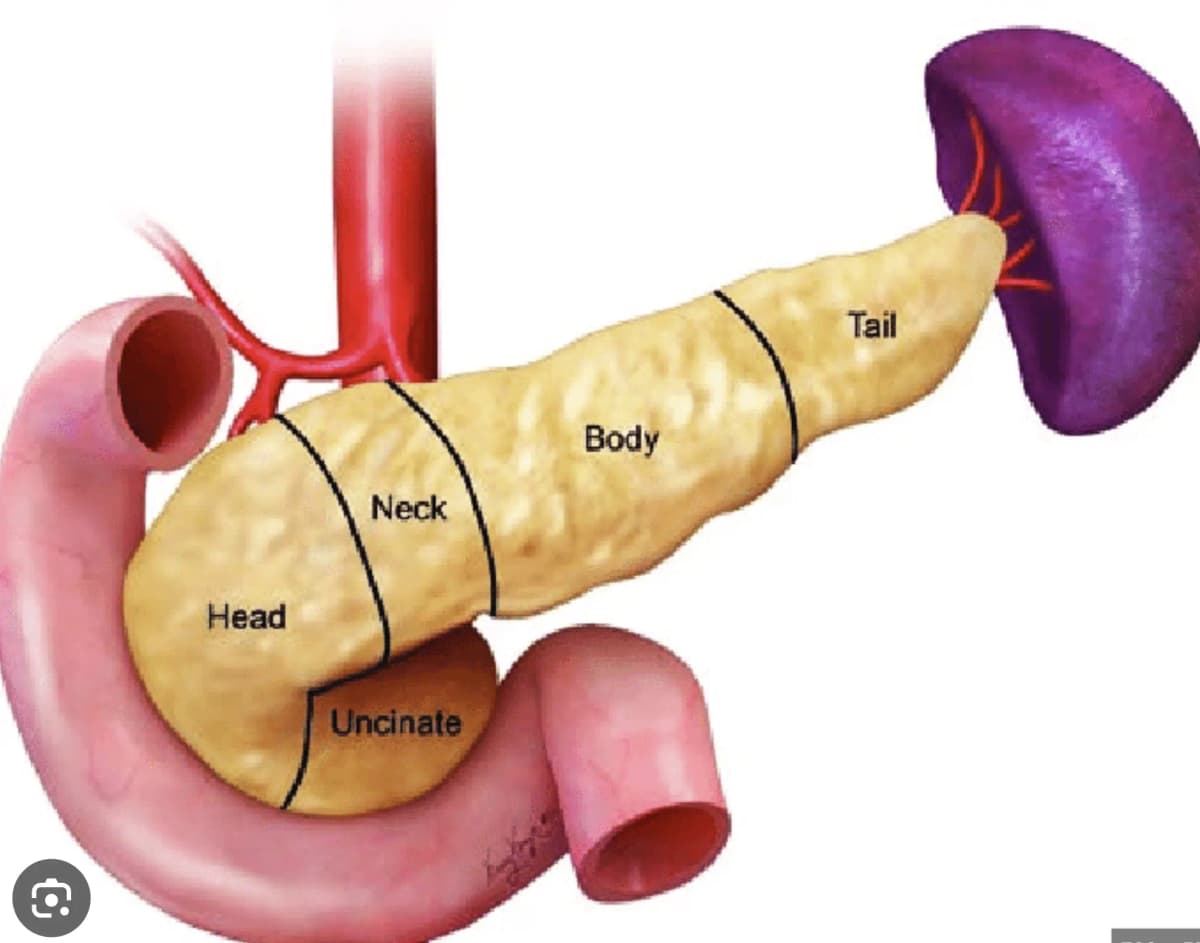
| Part | Location | Relations |
|---|---|---|
| Head | Nestled within the C-loop of the duodenum (D2) | Anterior: transverse colon, gastrocolic omentum. Posterior: IVC, right renal vein, right crus of diaphragm. The CBD runs through or behind the head of pancreas |
| Uncinate process | Hook-like projection from inferior head, passes behind SMA and SMV | This is why tumours here can encase the SMA early |
| Neck | Overlies SMA/SMV junction (portal vein formed here) | Narrowest portion; tumour here can compress the portal vein |
| Body | Crosses the aorta at L2, behind the stomach | Posterior: aorta, left crus, left adrenal, left kidney, splenic vein |
| Tail | Extends to the splenic hilum | Intimate relationship with splenic vessels; this is why distal pancreatectomy often requires splenectomy |
The relationship of the tumour to major vessels determines resectability — this is the single most important factor in surgical planning [3][4]:
- Superior Mesenteric Artery (SMA) — runs behind the neck/uncinate; involvement = usually unresectable
- Superior Mesenteric Vein (SMV) / Portal Vein (PV) — can be resected and reconstructed if involved < 180°
- Celiac trunk — involvement usually precludes resection
- Common Hepatic Artery (CHA) — limited involvement may be amenable to resection in borderline cases
- Splenic artery and vein — course along the superior and posterior border of the body/tail
- The main pancreatic duct (duct of Wirsung) runs the entire length of the pancreas and joins the CBD at the ampulla of Vater (hepatopancreatic ampulla), which opens into D2 via the major duodenal papilla.
- The accessory duct (duct of Santorini) drains the uncinate process and opens at the minor duodenal papilla.
- Head tumours compress the distal CBD and/or main pancreatic duct → "double duct sign" on imaging (simultaneous dilatation of both CBD and pancreatic duct, with abrupt cutoff at the head) [2][3].
| Anatomical relationship | Clinical consequence |
|---|---|
| CBD passes through/behind pancreatic head | Head tumours → early biliary obstruction → jaundice (this is why head tumours present earlier than body/tail tumours) |
| Pancreatic duct drains through head | Head tumours → pancreatic duct obstruction → exocrine insufficiency (steatorrhoea), acute pancreatitis |
| Retroperitoneal location | (1) Late presentation (no early peritoneal signs), (2) back pain from coeliac/splanchnic nerve plexus invasion |
| Proximity to SMA, celiac axis, PV/SMV | Even small tumours may be unresectable due to vascular encasement |
| Tail near splenic hilum | Tail tumours → splenic vein thrombosis → left-sided (sinistral) portal hypertension → gastric varices |
| Duodenal proximity | Head tumours → duodenal obstruction → gastric outlet obstruction (GOO) |
| Function | Component | Product | Clinical Implication When Lost |
|---|---|---|---|
| Exocrine (95% of parenchyma) | Acinar cells | Digestive enzymes: lipase, amylase, trypsinogen, chymotrypsinogen | Maldigestion → steatorrhoea, fat-soluble vitamin deficiency (A, D, E, K), weight loss |
| Exocrine | Ductal cells | Bicarbonate-rich fluid (neutralises gastric acid in duodenum) | Impaired neutralisation |
| Endocrine (5% — islets of Langerhans) | β-cells | Insulin | Diabetes mellitus |
| Endocrine | α-cells | Glucagon | Rare clinical consequence |
| Endocrine | δ-cells | Somatostatin | Rare clinical consequence |
| Endocrine | PP cells | Pancreatic polypeptide | Rare clinical consequence |
Remember
Exocrine insufficiency becomes clinically significant only when > 90% of exocrine function is lost. This is why steatorrhoea is a relatively late manifestation [7].
5. Etiology and Pathophysiology
PDAC arises from ductal epithelial cells of the pancreas (though some evidence suggests acinar cells can undergo acinar-to-ductal metaplasia as an initiating event).
Step-by-step pathogenesis:
-
Initiating mutation: KRAS (codon 12) — activating oncogene mutation present in > 90% of PDAC. KRAS is a GTPase molecular switch; the mutation locks it in the "ON" position → constitutive activation of RAS-RAF-MEK-ERK and PI3K-AKT-mTOR proliferative signalling pathways.
-
Tumour suppressor loss: Sequential inactivation of CDKN2A (p16 → loss of cell cycle G1 checkpoint), TP53 (loss of DNA damage response and apoptosis), and SMAD4/DPC4 (loss of TGF-β growth-inhibitory signalling).
-
Desmoplastic stromal reaction: A hallmark of PDAC. The tumour elicits a massive fibrotic/inflammatory stromal response (via pancreatic stellate cells) that:
- Creates a hypovascular, hypoxic microenvironment (tumour appears hypoattenuating/hypodense on CT because of poor blood supply — this is a key diagnostic feature) [3]
- Acts as a barrier to drug delivery (contributes to chemoresistance)
- Promotes immune evasion (excludes T-cells)
-
Perineural invasion: PDAC has a striking tropism for nerves (present in >80% of cases). Tumour cells invade perineural spaces of the splanchnic/coeliac nerve plexus → severe, unrelenting back pain.
-
Early vascular invasion and metastasis: Even small tumours demonstrate lymphovascular invasion. Common sites of distant metastasis:
| Factor | Explanation |
|---|---|
| Retroperitoneal location | Deep in the abdomen; no peritoneal irritation until very advanced |
| Body/tail tumours: no ductal obstruction | No jaundice or steatorrhoea → symptoms are only pain and weight loss → non-specific |
| Head tumours: earlier presentation (relative) | Compression of CBD → jaundice, but by the time jaundice appears, the tumour is often already involving peripancreatic vessels |
| Dense desmoplastic stroma | Masks the tumour on imaging (makes biopsy yield lower too) |
| Vague early symptoms | Epigastric discomfort, mild weight loss, new glucose intolerance — often attributed to other causes |
5.3 Specific Pathophysiology by Location
6. Classification
Exocrine tumours (> 95%):
- Ductal adenocarcinoma (85–90%) — the dominant type
- Adenosquamous carcinoma (~1–4%)
- Colloid (mucinous non-cystic) carcinoma
- Acinar cell carcinoma
- Undifferentiated carcinoma
- Undifferentiated carcinoma with osteoclast-like giant cells
- Pancreatoblastoma (paediatric)
- Solid pseudopapillary neoplasm (young women, indolent)
Endocrine (neuroendocrine) tumours (< 5%):
- Functional: insulinoma, gastrinoma, VIPoma, glucagonoma, somatostatinoma
- Non-functional PanNETs
Precursor lesions:
- PanIN (grades 1–3)
- IPMN (branch-duct vs. main-duct)
- MCN (mucinous cystic neoplasm)
| T Stage | Definition |
|---|---|
| T1 | Tumour ≤ 2 cm (T1a ≤ 0.5 cm, T1b > 0.5–1 cm, T1c > 1–2 cm) |
| T2 | Tumour > 2 cm but ≤ 4 cm |
| T3 | Tumour > 4 cm |
| T4 | Tumour involves celiac axis, SMA, and/or common hepatic artery (regardless of size) |
| N Stage | Definition |
|---|---|
| N0 | No regional lymph node metastasis |
| N1 | 1–3 positive regional lymph nodes |
| N2 | ≥ 4 positive regional lymph nodes |
| M Stage | Definition |
|---|---|
| M0 | No distant metastasis |
| M1 | Distant metastasis present |
| AJCC Stage | T | N | M | Approximate 5-Year Survival |
|---|---|---|---|---|
| IA | T1 | N0 | M0 | ~34% |
| IB | T2 | N0 | M0 | ~25% |
| IIA | T3 | N0 | M0 | ~15% |
| IIB | T1–T3 | N1 | M0 | ~10% |
| III | T1–T3 (N2) or T4 (any N) | N2 or any | M0 | ~3–5% |
| IV | Any T | Any N | M1 | < 3% |
This is arguably the most clinically important classification as it directly determines management [3][4]:
| Category | Definition | Management |
|---|---|---|
| Resectable | No arterial contact (SMA, celiac, CHA); no venous contact or ≤ 180° contact of SMV/PV without irregularity | Upfront surgery → adjuvant chemotherapy |
| Borderline resectable | Arterial: ≤ 180° contact with SMA or CHA (without extension to celiac axis); Venous: > 180° contact of SMV/PV, or ≤ 180° with irregular contour, or SMV/PV thrombosis if reconstruction feasible | Neoadjuvant chemotherapy ± CRT → restaging → surgery if response |
| Locally advanced (unresectable) | Arterial: > 180° contact with SMA or celiac; Venous: unreconstructable SMV/PV | Definitive chemotherapy ± radiation (palliative intent; conversion surgery in select responders) |
| Metastatic | Distant organ involvement | Palliative systemic chemotherapy |
Determining Resectability
A common exam mistake is thinking that "large tumour = unresectable." In reality, it is the relationship to major arteries (SMA, celiac axis, CHA) that determines resectability, NOT the tumour size. A 1.5 cm tumour encasing the SMA is unresectable, whereas a 5 cm tumour that does not contact major vessels may be resectable [3][4].
7. Clinical Features
The clinical presentation of pancreatic cancer depends critically on tumour location (head vs. body/tail) and stage (local vs. advanced/metastatic). The key teaching point is:
- Head tumours → present earlier (because of biliary obstruction causing jaundice)
- Body/tail tumours → present late (no biliary obstruction; only pain and constitutional symptoms)
"Pancreatic cancer is a great mimicker — it can present as back pain, new-onset diabetes, unexplained DVT, or depression before anyone thinks of the pancreas."
7.1 Symptoms
| Symptom | Location | Pathophysiological Basis |
|---|---|---|
| Painless progressive obstructive jaundice | Head | Tumour in the head compresses/invades the intrapancreatic portion of the common bile duct (CBD) → progressive obstruction → conjugated hyperbilirubinaemia → jaundice. It is painless because the obstruction is gradual (unlike gallstone impaction which causes colicky pain). This is the classic presentation [1][2][3][4] |
| Severe epigastric pain radiating to the back | Body/Tail (also head) | The pancreas sits on the retroperitoneal structures including the coeliac (solar) plexus and splanchnic nerves. Tumour growth posteriorly invades these nerve plexuses → deep, gnawing, relentless visceral pain radiating to the mid-back. Retroperitoneal infiltration is the key mechanism [1][2][3] |
| Weight loss / Anorexia | Any | Multifactorial: (1) Cancer cachexia (TNF-α, IL-6 mediated), (2) Exocrine insufficiency → maldigestion/malabsorption, (3) Biliary obstruction → reduced bile salts → fat malabsorption, (4) Anorexia from tumour-derived cytokines, (5) GOO if present |
| Symptom | Pathophysiological Basis |
|---|---|
| Pruritus | Bile salt deposition in the skin due to cholestasis. Bile salts activate itch receptors (TGR5 and possibly MRGPRX4 receptor) in cutaneous sensory nerve fibres. Can be extremely distressing and may precede clinical jaundice |
| Dark urine (tea/cola-coloured) | With CBD obstruction, conjugated bilirubin cannot be excreted into the gut. It backs up into the blood → is filtered by the kidneys (conjugated bilirubin is water-soluble) → dark urine [1] |
| Pale/clay-coloured stools (acholic stools) | Bilirubin cannot reach the gut → no bacterial conversion to stercobilinogen/stercobilin (which normally gives stool its brown colour) → pale, putty-like stools [1] |
| Steatorrhoea | Two mechanisms in head tumours: (1) Bile salt deficiency — obstruction of CBD prevents bile salts from reaching the duodenum → impaired fat emulsification, (2) Pancreatic lipase deficiency — obstruction of the pancreatic duct → loss of exocrine enzyme delivery → fat maldigestion → bulky, pale, foul-smelling, floating stools [1][2] |
| Symptom | Pathophysiological Basis |
|---|---|
| Steatorrhoea and maldigestion | Loss of exocrine pancreatic function (requires > 90% loss to become clinically apparent). Pancreatic duct obstruction by tumour → absence of lipase, amylase, proteases in the duodenum → fat and protein maldigestion |
| New-onset diabetes mellitus | Tumour destruction of islets of Langerhans → loss of β-cells → insulin deficiency. ALSO, tumour secretes diabetogenic factors (adrenomedullin, S100A8) that impair insulin secretion and signalling. New-onset DM in an elderly patient (especially with weight LOSS rather than gain) should raise suspicion for occult pancreatic cancer [1][2] |
New-Onset DM as a Red Flag
Glucose intolerance is present in ~80% and overt DM in ~50% of pancreatic cancer patients at diagnosis [1]. The typical T2DM patient gains weight; a patient with pancreatic cancer-related DM is LOSING weight. New-onset diabetes in a patient > 50 with unexplained weight loss = think pancreatic cancer.
| Symptom | Pathophysiological Basis |
|---|---|
| Nausea and vomiting | (1) Constitutional/cancer cachexia effect, (2) Gastric outlet obstruction (GOO) — tumour in pancreatic head/uncinate process invades or externally compresses the duodenum (D2/D3) [1][2] |
| Fatigue and weakness | Anaemia (chronic disease, malabsorption of iron/B12/folate), cancer cachexia, malnutrition |
| Acute pancreatitis | Tumour occluding the main pancreatic duct → upstream ductal hypertension → premature activation of pancreatic enzymes → acute pancreatitis. Unexplained acute pancreatitis in a patient > 50 without obvious cause (no gallstones, no alcohol) should prompt imaging to exclude pancreatic cancer [1][2] |
| Depression / Psychological disturbance | Pancreatic cancer has a notably high association with depression, even before diagnosis. The mechanism is unclear — possibly related to paraneoplastic neuropsychiatric effects, or cytokine-mediated central effects |
| Feature | Description |
|---|---|
| Site | Epigastric |
| Onset | Insidious (weeks to months); rarely acute (pancreatitis) |
| Character | Deep, gnawing, visceral quality |
| Radiation | To the sides and back (bilateral, band-like). Severe back pain suggests body/tail tumour invading coeliac/mesenteric plexus [1] |
| Associated symptoms | Jaundice, weight loss, anorexia |
| Time course | Present for 1–2 months at time of presentation; progressive |
| Exacerbating factors | Eating, lying supine, nighttime [1] |
| Relieving factors | Curled/fetal position, leaning forward (because this takes pressure off the retroperitoneal structures/coeliac plexus) [1] |
7.2 Signs
| Sign | Explanation |
|---|---|
| Jaundice (scleral icterus, skin) | Visible when serum bilirubin > 34–50 μmol/L. Best seen in sclerae (bilirubin has high affinity for elastin). Predominantly conjugated (direct) hyperbilirubinaemia in obstructive jaundice |
| Courvoisier's sign | Painless jaundice + palpable, distended gallbladder. Courvoisier's law states: "In the presence of obstructive jaundice, a palpable gallbladder is unlikely to be due to gallstones" — because chronic gallstone disease causes a fibrotic, non-distensible gallbladder. A malignant, gradual obstruction of the distal CBD allows the gallbladder to distend progressively [1][3][4] |
| Scratch marks (excoriations) | From intractable pruritus due to bile salt deposition in skin |
| Hepatomegaly | Cholestatic liver; back-pressure from biliary obstruction |
Courvoisier's Sign — Classic Exam Favourite
Courvoisier's sign: Painless jaundice + palpable, non-tender, distended gallbladder = malignant distal CBD obstruction until proven otherwise. The most common cause is pancreatic head cancer. Remember: gallstones cause a fibrotic, shrunken gallbladder that cannot distend, whereas a slowly growing tumour causes gradual, painless distension [3][4].
| Sign | Pathophysiology |
|---|---|
| Hepatomegaly (nodular/irregular) | Liver metastases — the liver is the most common site of distant spread |
| Ascites | Peritoneal carcinomatosis → malignant ascites (exudative, high protein, high LDH, may contain malignant cells on cytology) |
| Virchow's node (left supraclavicular lymphadenopathy) | Metastatic spread via thoracic duct → left supraclavicular (Virchow's) node. Named after Rudolf Virchow. Also called Troisier's sign [1] |
| Sister Mary Joseph's nodule | Palpable periumbilical mass — metastatic deposit at the umbilicus via peritoneal spread along the falciform ligament or direct seeding [1] |
| Blumer's shelf | Palpable mass on rectal exam (drop metastasis to the pouch of Douglas / rectovesical pouch) |
| Abdominal mass | Palpable epigastric mass = usually advanced disease [1] |
| Cachexia | Profound wasting — temporal wasting, loss of subcutaneous fat, muscle wasting |
| Manifestation | Mechanism |
|---|---|
| New-onset DM | Tumour-secreted diabetogenic factors + islet destruction [1] |
| Trousseau's syndrome (migratory superficial thrombophlebitis) | Tumour-elaborated procoagulants (tissue factor, cancer procoagulant — a cysteine protease that directly activates factor X) and platelet-aggregating factors create a hypercoagulable state. Manifests as migratory thrombophlebitis (different veins at different times) or DVT/PE. Armand Trousseau himself died of gastric cancer with this syndrome [1][2] |
| Pancreatic panniculitis | Erythematous subcutaneous nodular fat necrosis, typically on legs. Caused by systemic spillage of excess digestive pancreatic enzymes (especially lipase from acinar cell carcinoma) → autodigestion of subcutaneous fat [1] |
| Paraneoplastic pemphigoid | Autoimmune blistering skin disorder; rare [2] |
| Depression | Occurs with disproportionate frequency; mechanism unclear (cytokine-mediated?) |
| Feature | Pancreatic Head | Pancreatic Body/Tail |
|---|---|---|
| Frequency | ~70% | ~25–30% |
| Presenting symptom | Painless obstructive jaundice | Severe epigastric/back pain |
| Jaundice | Early and common | Late (only with liver mets or direct extension) |
| Courvoisier's sign | Yes | No |
| Steatorrhoea | Common (CBD + pancreatic duct obstruction) | Less common |
| Back pain | Present but may be less severe | Prominent — indicates coeliac/splanchnic plexus invasion [1] |
| GOO | Possible (D2 compression) | Rare |
| Diagnosis timing | Relatively earlier (jaundice prompts investigation) | Late — most are advanced/metastatic at presentation |
| Resectability | ~15–20% resectable at diagnosis | Rarely resectable |
| Operation | Pancreaticoduodenectomy (Whipple) [3][4] | Distal pancreatectomy ± splenectomy [1] |
| Aspect | Key Points |
|---|---|
| Definition | Malignant epithelial neoplasm of pancreas; > 85% PDAC |
| Epidemiology | 5th cause cancer death in HK; peak age 60–80; M > F; 5-yr survival ~10% |
| Location | 70% head, 15% body, 10% tail, 5–20% diffuse |
| Risk factors | Smoking (most important modifiable), chronic pancreatitis, DM, obesity, IPMN, BRCA2, Lynch, Peutz-Jeghers, FAMMM |
| Genetics | KRAS (> 90%), CDKN2A, TP53, SMAD4 |
| Head presentation | Painless obstructive jaundice, Courvoisier's sign, steatorrhoea, dark urine, pale stools |
| Body/tail presentation | Severe back pain, weight loss, late diagnosis |
| Metastasis sites | Liver > peritoneum > lung > bone |
| Paraneoplastic | New-onset DM, Trousseau syndrome, pancreatic panniculitis |
| Resectability | Determined by arterial involvement (SMA, celiac, CHA), not tumour size |
High Yield Summary
-
Pancreatic cancer ≈ PDAC (> 85%) — retroperitoneal, aggressive, dense desmoplastic stroma, poor prognosis (5-yr survival ~10%).
-
Painless progressive obstructive jaundice = hallmark of pancreatic head cancer; Courvoisier's sign = painless jaundice + palpable gallbladder.
-
Body/tail tumours present LATE with severe back pain (coeliac plexus invasion) and are rarely resectable.
-
Key risk factors: Smoking (~3× risk), chronic pancreatitis, DM (new-onset DM can be the first sign!), obesity, BRCA2 (most common hereditary gene), Lynch syndrome, Peutz-Jeghers, FAMMM, IPMN.
-
Genetic drivers: KRAS (> 90%), CDKN2A, TP53, SMAD4 — sequential accumulation through PanIN stages.
-
Resectability is determined by vascular involvement (SMA, celiac axis, CHA, SMV/PV), NOT tumour size.
-
Trousseau's syndrome (migratory superficial thrombophlebitis) = hypercoagulable paraneoplastic state; pancreatic panniculitis = subcutaneous fat necrosis from enzyme spillage.
-
New-onset DM in elderly patient + weight loss = suspect pancreatic cancer until proven otherwise.
-
Sites of metastasis: Liver (most common) > Peritoneum > Lung > Bone.
-
The "double duct sign" on imaging (dilated CBD + dilated pancreatic duct) is highly suggestive of pancreatic head malignancy.
Active Recall - Pancreatic Cancer (Definition to Clinical Features)
[1] Senior notes: felixlai.md (Pancreatic cancer section) [2] Senior notes: maxim.md (Pancreatic carcinoma section) [3] Lecture slides: Malignant biliary obstruction.pdf [4] Lecture slides: WCS 056 - Painless jaundice and epigastric mass - by Prof R Poon.ppt (1).pdf [5] Lecture slides: The Managment of breast cancer_Prof A Kwong 20_2_2020.pdf (p32 — BRCA2 lifetime risk) [6] Lecture slides: GC 202. Surgery may cure your cancer Surgical oncology.pdf [7] Senior notes: maxim.md (Chronic pancreatitis / Pancreatic cyst sections) [8] Senior notes: maxim.md (Pancreatic cyst — IPMN section)
Differential Diagnosis of Pancreatic Cancer
The differential diagnosis of pancreatic cancer is broad because the presenting features — epigastric pain, obstructive jaundice, weight loss, new-onset diabetes — are non-specific and shared by many hepatobiliary, pancreatic, and even extra-abdominal conditions [1]. The key principle taught in the lectures is:
"Painless progressive obstructive jaundice in elderly is malignant biliary obstruction until proven otherwise" [9]
The differential should be structured around two clinical axes:
- The presenting syndrome — Are we dealing with obstructive jaundice? Epigastric/back pain? A pancreatic mass? New-onset diabetes?
- The imaging appearance — Is the pancreatic lesion cystic or solid? [1]
This dual approach is how the senior notes frame it, and it makes clinical sense: you encounter the patient first (history/exam) then refine after imaging.
Framework 1: Differential by Presenting Syndrome
This is the most important differential list for exams. The causes can be organised by the anatomical level of obstruction and whether the obstruction is intraluminal, mural, or extramural [9][3].
The lecture slide explicitly lists the following cancers occurring along the biliary tract [3][4]:
- Cholangiocarcinoma (intrahepatic, perihilar/Klatskin tumour, distal)
- Carcinoma of the gallbladder
- Carcinoma of the head of pancreas
- Periampullary carcinoma (ampulla of Vater)
- Carcinoma of the duodenum
- Porta hepatis lymphadenopathy (metastatic)
| Location of Obstruction | Intraluminal | Mural | Extramural |
|---|---|---|---|
| Proximal / Hilar | Choledocholithiasis (migrated), RPC stones | Cholangiocarcinoma (Klatskin tumour) [3][4], PSC stricture | Porta hepatis lymphadenopathy [4], CA gallbladder invading CHD [3] |
| Mid-CBD | Gallstone (choledocholithiasis) | Cholangiocarcinoma (mid-duct) | Mirizzi syndrome (gallstone in cystic duct/Hartmann's pouch compressing CHD externally) |
| Distal CBD / Periampullary | Gallstone impacted at ampulla | Distal cholangiocarcinoma, ampullary carcinoma [3][4] | CA head of pancreas [3][4], CA duodenum [3][4], periampullary lymphadenopathy |
How to Differentiate Stone vs. Tumour on History
Stone = typically episodic pain (biliary colic), may have fever/rigors (cholangitis — Charcot's triad), fluctuating jaundice (stone ball-valves in and out of the ampulla), history of gallstones/biliary colic.
Tumour = painless, progressive, relentless jaundice (gradual obstruction, no intermittent relief), weight loss, palpable gallbladder (Courvoisier's sign), constitutional symptoms [9].
The lecture slide by Prof R Poon explicitly lists the pathology producing jaundice AND epigastric mass [4]:
- Hepatomegaly secondary to biliary obstruction (back-pressure → enlarged, smooth liver)
- Hepatomegaly due to metastases or HCC (nodular, hard liver)
- Lymph node metastases to the coeliac axis or porta hepatis
- Carcinoma of stomach with metastatic lymph node in the porta hepatis (gastric cancer → coeliac/portal LN → biliary obstruction)
- Distended stomach due to duodenal obstruction by tumour which also obstructs the bile duct (i.e., pancreatic head cancer causing both GOO and biliary obstruction simultaneously)
This is high yield because it reminds you that "jaundice + epigastric mass" is not exclusively pancreatic cancer — gastric cancer with portal lymphadenopathy, HCC, and even lymphoma can produce the same constellation.
| Condition | Distinguishing Features |
|---|---|
| Pancreatic cancer | Insidious onset, progressive weight loss, jaundice (if head), new-onset DM, relieved by leaning forward |
| Chronic pancreatitis | Difficult to distinguish from CA pancreas! [7] History of alcohol/recurrent acute pancreatitis, pancreatic calcifications on imaging, "chain of lakes" on MRCP, may have steatorrhoea triad |
| Acute pancreatitis | Acute onset, serum lipase/amylase > 3× ULN, obvious aetiology (gallstones, alcohol) |
| Peptic ulcer disease (posterior DU) | Posterior duodenal ulcer can erode into pancreas → back pain; meal-related, responds to PPI, positive H. pylori |
| Abdominal aortic aneurysm | Pulsatile epigastric mass, radiates to back, may be asymptomatic or present with rupture |
| Retroperitoneal lymphoma | Younger patient, B-symptoms, bulky retroperitoneal lymphadenopathy on CT |
| Condition | Clue |
|---|---|
| Pancreatic cancer | Most important to rule out; associated with obstructive jaundice, back pain |
| Chronic pancreatitis | Long alcohol history, pancreatic calcifications, exocrine insufficiency preceding endocrine insufficiency [7] |
| Type 1 DM (late-onset/LADA) | Autoantibodies (anti-GAD, anti-IA2), ketosis-prone, lean |
| Haemochromatosis | Bronze diabetes, liver disease, arthropathy, iron studies |
This is the framework explicitly provided in the senior notes [1]. When imaging shows a pancreatic mass, the first branch point is: is it cystic or solid?
| Imaging | Category | Differential Diagnosis | Key Differentiating Features |
|---|---|---|---|
| Cystic | Inflammatory fluid collections | Acute peripancreatic fluid collections (APFC) | Context of recent acute pancreatitis; < 4 weeks |
| Pancreatic pseudocyst | > 4 weeks after acute pancreatitis, encapsulated, no solid component, NO epithelial lining (hence "pseudo"), amylase-rich fluid | ||
| Acute necrotic collections (ANC) / Walled-off necrosis (WON) | Necrotising pancreatitis; heterogeneous content (fluid + necrotic debris) | ||
| Non-neoplastic | True cyst, retention cyst, mucinous non-neoplastic cyst, lymphoepithelial cyst | Usually incidental, no worrisome features | |
| Neoplastic | Serous cystic neoplasm (SCN) | Older women, microcystic/"honeycomb" pattern, central calcified scar, NO malignant potential → observe [8] | |
| Mucinous cystic neoplasm (MCN) | Perimenopausal women, body/tail, ovarian-type stroma, macrocystic, malignant potential [8] | ||
| Intraductal papillary mucinous neoplasm (IPMN) | Pancreatic head in old men; main-duct (high malignant risk → resect) vs. branch-duct (observe unless high-risk stigmata: > 4 cm, mural nodules, main duct > 10 mm) [8] | ||
| Solid | Non-neoplastic | Focal chronic pancreatitis | Very difficult to distinguish from pancreatic cancer! [7] History of alcohol, diffuse calcifications, "chain of lakes" duct, IgG4 may help |
| Autoimmune pancreatitis (AIP) | Type 1 = IgG4-related disease (diffuse "sausage-shaped" pancreas, multifocal biliary strictures, ↑ serum IgG4, responds dramatically to steroids); Type 2 = associated with IBD. Key DDx because it mimics cancer but is treated medically! | ||
| Solid pseudopapillary neoplasm | Young women (20–30s), large well-encapsulated mass with cystic degeneration, low malignant potential, excellent prognosis after resection | ||
| Neoplastic — Malignant | Pancreatic ductal adenocarcinoma (PDAC) | Hypoattenuating mass, double duct sign, vascular encasement, desmoplastic stroma | |
| Pancreatic neuroendocrine tumour (PanNET) | Hyperenhancing (hyperdense) on arterial phase CT (contrast with PDAC which is hypo-attenuating!) ± calcifications, chromogranin A positive, somatostatin receptor scintigraphy positive [10] | ||
| Lymphoma (pancreatic) | Rare, bulky mass, B-symptoms, responds to chemotherapy, biopsy essential | ||
| Metastasis to pancreas | Most common primary: renal cell carcinoma (RCC) [2], also lung, breast, melanoma; usually well-circumscribed, hypervascular, history of prior malignancy |
PDAC vs. PanNET on CT — A Classic Distinction
This is a common exam trap. PDAC appears hypoattenuating (hypodense) on CT because of its dense desmoplastic, hypovascular stroma. PanNETs appear hyperenhancing (hyperdense) on arterial phase because they are highly vascular. Also: PDAC = no calcifications, PanNET may have calcifications; PDAC = CA19-9 elevated, PanNET = chromogranin A elevated [10][2].
All tumours arising within 2 cm of the ampulla of Vater are termed periampullary cancers. They all present similarly (painless obstructive jaundice) and all require Whipple's procedure for curative resection, but they have different prognoses [2][3][4]:
| Tumour | Key Distinguishing Features | 5-Year Survival After Resection |
|---|---|---|
| CA head of pancreas | Dull aching pain radiating to back, new-onset DM [2]; hypoattenuating mass, double duct sign | ~10–25% |
| Distal cholangiocarcinoma | Elderly, cholestatic LFTs, may have PSC history [2] | ~25–40% |
| Ampulla of Vater carcinoma | Jaundice (may fluctuate due to tumour necrosis — intermittent obstruction), fat malabsorption; visible on duodenoscopy [2] | ~40–60% |
| Periampullary duodenal carcinoma | Rare, except in FAP (familial adenomatous polyposis); Thomas' sign: silver stool (obstructive jaundice → white stool + tumour ulceration → melena → combined appearance) [2] | ~50–60% |
Thomas' Sign
Thomas' sign = silver stool — an uncommon but pathognomonic finding of periampullary duodenal carcinoma. The "silver" colour arises from the combination of pale/clay stool (biliary obstruction) mixed with melaena (GI bleeding from tumour ulceration). White + black = silver [2].
This deserves special emphasis because chronic pancreatitis is notoriously difficult to distinguish from pancreatic cancer [7], and getting it wrong has serious consequences (unnecessary Whipple's for pancreatitis, or missed cancer treated as pancreatitis).
| Feature | Chronic Pancreatitis | Pancreatic Cancer |
|---|---|---|
| History | Long alcohol history, recurrent acute attacks | No prior pancreatic disease; smoking, new-onset DM |
| Pain pattern | Recurrent, may eventually become "burnt out" (painless) | Progressive, unrelenting |
| Calcifications | Diffuse pancreatic calcifications | Absent (usually) |
| Duct | "Chain of lakes" (diffuse alternating stricture-dilatation) | Single focal duct cutoff with upstream dilatation |
| Mass | May have focal inflammatory mass | Hypoattenuating mass with vascular encasement |
| CA 19-9 | May be mildly elevated (especially if cholangitis) | Usually markedly elevated (but not diagnostic) |
| IgG4 | Elevated in autoimmune pancreatitis (type 1) | Normal |
| Biopsy | May be needed (EUS-guided) to differentiate | Definitive; but not mandatory if resectable |
Autoimmune pancreatitis is the one condition you absolutely must exclude before committing to Whipple's, because it responds to steroids. The imaging can look identical to PDAC.
| Feature | AIP Type 1 (IgG4-related) | PDAC |
|---|---|---|
| Age/Sex | Middle-aged to elderly male | Elderly, M > F |
| Pancreatic imaging | "Sausage-shaped" diffuse enlargement, loss of lobularity, capsule-like rim | Focal hypoattenuating mass |
| Biliary strictures | Multifocal (intrahepatic + extrahepatic) — mimics PSC/cholangiocarcinoma | Single distal CBD stricture |
| Serum IgG4 | Elevated (> 2× ULN highly specific) | Normal |
| Other organ involvement | Salivary glands, retroperitoneum, kidneys (systemic IgG4-related disease) | None |
| Response to steroids | Dramatic response (diagnostic and therapeutic) | No response |
| EUS-FNA | Lymphoplasmacytic infiltrate, storiform fibrosis, obliterative phlebitis | Adenocarcinoma cells |
The lecture slide provides a comprehensive table of tumour markers [3]:
| Marker | Upper Normal | Sensitivity in Pancreatic Cancer | Non-Malignant Causes of Elevation | Key Point |
|---|---|---|---|---|
| AFP | 10 ng/ml | Low (not a pancreatic marker) | Hepatitis, cirrhosis, biliary obstruction | Useful to differentiate HCC from cholangioCA/PDAC |
| CEA | 5 ng/ml | 30–70% in pancreatic cancer | Smoking, liver disease, bowel diseases, peptic ulcer, pancreatitis, renal failure [3] | Not specific; primarily a CRC marker |
| CA 19-9 | 37 U/ml | 72–79% in pancreatic cancer | Benign biliary diseases, benign pancreatic diseases (cholangitis, gallstones, chronic pancreatitis) [3] | NOT sensitive or specific enough for diagnosis; best used for prognosis and monitoring treatment response/recurrence [1][2]. Requires Lewis blood group antigen expression (5–10% of population are Lewis-negative and will never elevate CA 19-9) |
| CA 125 | 35 U/ml | ~60% in pancreatic cancer | Benign pancreatic and liver disease [3] | Primarily an ovarian cancer marker |
| DUPAN-2 | 150 U/ml | ~70% in pancreatic/biliary cancer | Benign hepatobiliary diseases (hepatitis, cholelithiasis) [3] | Less commonly used clinically |
CA 19-9: Know Its Limitations
CA 19-9 is NOT a screening or diagnostic test for pancreatic cancer. It is elevated in ~75–80% of PDAC but also elevated in cholangitis, choledocholithiasis, chronic pancreatitis, and other GI malignancies. Conversely, 5–10% of the population are Lewis antigen-negative and will NEVER produce CA 19-9 regardless of tumour burden. Its main role is prognostic + monitoring treatment response and detecting recurrence after surgery [1][2][3].
| Clinical Scenario | Top Differentials to Consider |
|---|---|
| Painless obstructive jaundice + palpable GB | CA head of pancreas, distal cholangioCA, ampullary CA |
| Painless obstructive jaundice + hepatomegaly | HCC, liver metastases, proximal cholangioCA |
| Jaundice + epigastric mass | All causes listed by Prof Poon [4]: biliary obstruction with hepatomegaly, liver mets/HCC, coeliac/portal LN mets, gastric CA with LN mets, distended stomach from duodenal obstruction |
| Epigastric pain radiating to back + weight loss | PDAC (body/tail), chronic pancreatitis, AAA, retroperitoneal lymphoma |
| Pancreatic mass + new-onset DM | PDAC (most important to exclude), chronic pancreatitis |
| Solid hypoattenuating pancreatic mass | PDAC (most likely), focal chronic pancreatitis, AIP |
| Solid hyperenhancing pancreatic mass | PanNET, metastasis (RCC, melanoma) |
| Cystic pancreatic lesion | IPMN, MCN, SCN, pseudocyst, solid pseudopapillary tumour |
High Yield Summary — Differential Diagnosis
-
Painless progressive obstructive jaundice in elderly = malignant biliary obstruction until proven otherwise. Top DDx: CA head of pancreas, distal cholangioCA, ampullary CA, CA duodenum.
-
Periampullary cancers (within 2 cm of ampulla): pancreatic head, distal CBD, ampullary, duodenal — all present with painless jaundice but have very different prognoses (ampullary best, PDAC worst).
-
Chronic pancreatitis is notoriously difficult to distinguish from PDAC — look for diffuse calcifications, chain-of-lakes duct, alcohol history; may need biopsy.
-
Autoimmune pancreatitis (IgG4-related) mimics PDAC but responds dramatically to steroids — check IgG4, look for sausage-shaped pancreas and multiorgan IgG4 disease.
-
PDAC = hypoattenuating on CT; PanNET = hyperenhancing on arterial phase — a key imaging distinction.
-
CA 19-9 is NOT diagnostic — use for prognosis and monitoring. Lewis-negative patients (5–10%) will never elevate CA 19-9.
-
Thomas' sign (silver stool) = pathognomonic of periampullary duodenal carcinoma (white stool from obstruction + melaena from tumour ulceration).
-
Metastases to pancreas: most commonly from RCC, also lung, breast, melanoma — usually well-circumscribed and hypervascular.
Active Recall - Differential Diagnosis of Pancreatic Cancer
References
[1] Senior notes: felixlai.md (Pancreatic cancer section) [2] Senior notes: maxim.md (Pancreatic carcinoma section; Periampullary malignancy section) [3] Lecture slides: Malignant biliary obstruction.pdf (p5 — cancers along biliary tract; p8 — tumour markers table) [4] Lecture slides: WCS 056 - Painless jaundice and epigastric mass - by Prof R Poon.ppt (1).pdf (p24 — cancers along biliary tract; p32 — pathology producing jaundice and epigastric mass) [7] Senior notes: maxim.md (Chronic pancreatitis section) [8] Senior notes: maxim.md (Pancreatic cyst section) [9] Senior notes: maxim.md (Obstructive jaundice section) [10] Senior notes: maxim.md (Pancreatic neuroendocrine tumours section; Non-functioning pNET vs CA pancreas table)
Diagnostic Criteria, Algorithm, and Investigations for Pancreatic Cancer
Unlike acute pancreatitis (which has the classic 2-out-of-3 criteria) or autoimmune pancreatitis (which has the HISORt criteria), pancreatic ductal adenocarcinoma has no universally codified "diagnostic criteria" per se. Instead, the diagnosis is established through a sequential clinical-radiological-pathological approach:
- Clinical suspicion — based on symptoms (painless obstructive jaundice, back pain, weight loss, new-onset DM)
- Cross-sectional imaging — pancreatic protocol CT is the cornerstone
- Tissue diagnosis — required in certain scenarios but NOT mandatory if the tumour is potentially resectable [1][2]
The overarching principle: once you suspect pancreatic cancer, the primary goal of investigation is not just diagnosis but simultaneously determining resectability — because resectability directly dictates management.
Key Principle
The diagnosis and staging of pancreatic cancer are pursued in parallel, not sequentially. A pancreatic protocol CT scan simultaneously (a) identifies the mass, (b) characterises it, (c) assesses vascular involvement for resectability, and (d) screens for metastatic disease. You do not wait for a biopsy before staging [1][2][3].
The approach follows a logical sequence that mirrors real clinical thinking:
Step 1: Clinical suspicion → Baseline bloods
Step 2: Initial imaging (USG) → Pancreatic protocol CT
Step 3: Assess resectability on CT
Step 4: Tissue diagnosis (only if needed)
Step 5: Complete staging (CT TAP ± PET-CT, ± staging laparoscopy)
Investigations — Systematic Breakdown
The examination is not a mere formality — it actively contributes to diagnosis and staging.
| Examination | Finding | What It Tells You |
|---|---|---|
| General | Jaundice (scleral icterus) | Biliary obstruction — confirms the clinical suspicion |
| Cachexia (temporal wasting, muscle loss) | Advanced disease; poor nutritional status — impacts surgical fitness | |
| Lymphadenopathy | Virchow's node (left supraclavicular) = distant metastatic disease → Stage IV | |
| Abdomen | Scratch marks | Pruritus from cholestasis |
| Sister Mary Joseph's nodule (periumbilical) | Peritoneal carcinomatosis with spread via falciform ligament | |
| Hepatomegaly | Either cholestatic (smooth, non-tender) or metastatic (nodular, hard) | |
| Epigastric mass | Palpable pancreatic tumour = usually advanced | |
| Ascites | Peritoneal carcinomatosis or portal hypertension from PV invasion | |
| Courvoisier's sign | Painless jaundice with palpable gallbladder → points towards malignant biliary obstruction (MBO) [1][4][11] |
The lecture by Prof R Poon emphasises Courvoisier's law with its exceptions [4][11]:
Definition: "In painless jaundice, if the gallbladder is palpable, it is unlikely to be due to gallstones" — points towards malignant biliary obstruction.
Reason: Gallstones develop chronically → chronic cholecystitis → fibrosed/contracted GB that cannot distend. Malignant obstruction develops gradually in a previously normal GB → progressive distension from back-pressure.
Exceptions [11]:
- Double gallstones: one at CBD (causing jaundice) + another at cystic duct (causing mucocele → GB distension despite fibrosis)
- Recurrent pyogenic cholangitis (RPC): pathology is in the bile duct, not the GB → CBD obstruction without chronic cholecystitis → GB can still distend
Courvoisier's Law — Exceptions
Students often state Courvoisier's law as absolute. Remember the two exceptions: double gallstones (CBD + cystic duct) and RPC (bile duct pathology, not GB pathology). Also note that gallstones can sometimes be painless too — the law is about the palpable GB, not the pain [11].
| Investigation | Expected Finding in Pancreatic Cancer | Pathophysiological Basis |
|---|---|---|
| CBC with differentials | Anaemia (normocytic, of chronic disease); leukocytosis if concurrent biliary sepsis/cholangitis; thrombocytopenia to check before ERCP [1][11] | Chronic disease anaemia from cancer cachexia + malabsorption (iron, B12, folate) |
| Clotting profile (PT/INR) | Prolonged PT/INR | Vitamin K deficiency from obstructive jaundice — bile salts cannot reach the gut → fat-soluble vitamin (K) malabsorption → reduced hepatic synthesis of factors II, VII, IX, X. This MUST be corrected before any invasive procedure (give IV vitamin K) [1][11] |
| LFT | ↑ ALP and GGT (cholestatic pattern), ↑ conjugated (direct) bilirubin, albumin for nutritional status [1][2][11] | ALP is located on the canalicular membrane of hepatocytes; biliary obstruction causes bile backup → cholestasis → upregulation and leakage of ALP into blood. GGT confirms the ALP is of hepatobiliary origin (vs. bone). Conjugated bilirubin rises because it is formed normally in the liver but cannot be excreted into the bile |
| RFT | Hyponatraemia, hypokalaemia [1] | Secondary to vomiting (especially if GOO present), poor oral intake |
| Serum glucose / HbA1c | Hyperglycaemia / elevated HbA1c | New-onset DM is both a consequence AND early manifestation of pancreatic cancer. New-onset DM in an older adult should prompt screening for occult pancreatic cancer [1][2] |
| Serum amylase and lipase | May be elevated if acute pancreatitis present | Tumour occlusion of pancreatic duct → upstream ductal hypertension → premature enzyme activation → pancreatitis [1] |
| CA 19-9 | Elevated in ~75–80% of patients [1][2][3] | See detailed discussion below |
| CEA | Raised in 30–60% [2] | Non-specific; can be elevated in CRC, gastric, lung, breast cancers |
CA 19-9 — A Detailed Discussion
CA 19-9 (Carbohydrate Antigen 19-9) is a mucin-bound sialylated Lewis-a blood group antigen (a modified Lewis antigen). Understanding its properties is essential:
| Property | Detail |
|---|---|
| Upper normal limit | 37 U/ml [3] |
| Sensitivity in pancreatic cancer | 72–79% [3] |
| Specificity | Poor — elevated in many other conditions |
| NOT useful as a screening/diagnostic tool | Not sensitive and not specific enough to allow early diagnosis of CA pancreas [1][2] |
| Primary role | Prognostic marker + monitoring disease activity after surgery/chemotherapy. Serial monitoring of CA 19-9 predicts recurrence and long-term prognosis [1] |
| Lewis antigen requirement | Requires the presence of the Lewis blood group antigen to be expressed — approximately 5–10% of the population are Lewis-negative and will NEVER produce CA 19-9 regardless of tumour burden [1] |
| Non-malignant causes of elevation | Benign biliary diseases, benign pancreatic diseases (chronic pancreatitis, cholangitis, choledocholithiasis) [3] |
| Malignant causes (other than PDAC) | HCC, cholangioCA, CA gallbladder, gastric cancer, CRC, ovarian tumours [1][3] |
The lecture slide tumour marker table [3] also lists:
| Marker | Upper Normal | Key Cancer Association | Non-Malignant Causes |
|---|---|---|---|
| AFP | 10 ng/ml | HCC (70–90%), cholangioCA (10%) | Hepatitis, cirrhosis, biliary obstruction |
| CEA | 5 ng/ml | CRC (30–70%), gastric, pancreatic, lung, breast | Smoking, liver disease, bowel diseases, peptic ulcer, pancreatitis, renal failure |
| CA 19-9 | 37 U/ml | Pancreatic cancer (72–79%), biliary cancer (67–73%), gastric (42–62%), CRC (19–41%) | Benign biliary/pancreatic diseases |
| CA 125 | 35 U/ml | Ovarian (80%), pancreatic (60%) | Benign pancreatic and liver disease |
| DUPAN-2 | 150 U/ml | Pancreatic and biliary cancer (70%) | Benign hepatobiliary diseases (hepatitis, cholelithiasis) |
CA 19-9: What It Can and Cannot Do
CA 19-9 CANNOT diagnose pancreatic cancer — it is neither sensitive nor specific. It CAN: (1) Serve as a prognostic marker at diagnosis (very high levels suggest unresectability/metastatic disease), (2) Monitor treatment response (falling levels = good response; rising levels = recurrence/progression), (3) Help detect recurrence after curative resection via serial monitoring [1][2][3].
3. Radiological Investigations
| Aspect | Detail |
|---|---|
| Role | Initial imaging modality for any patient with suspected pancreatic cancer or obstructive jaundice [1][2][12] |
| Strengths | High sensitivity for detecting biliary tract dilatation (IHD and CBD), establishing level of obstruction, detecting pancreatic masses > 3 cm, non-invasive, no radiation, cheap, widely available |
| Limitations | Poor sensitivity for small tumours (< 3 cm), body/tail of pancreas often obscured by bowel gas and body habitus [1][12] |
| Typical findings | Focal hypoechoic hypovascular solid mass with irregular margins + dilatation of CBD [1] |
| Normal CBD size | CBD > 0.8 cm is pathological (rule of thumb: 0.1 cm per decade of age is the upper limit, e.g. 6 mm at age 60, 7 mm at age 70) [12] |
| What to assess | Pancreas (mass? duct dilatation?), biliary system (CBD dilatation, level of obstruction, stones?), GB (distended? contracted? stones?), liver (IHD dilatation, liver mets, abscess?) [12] |
This is the single most important investigation in the workup of pancreatic cancer [1][2][3].
What is "pancreatic protocol CT"?
It is a multidetector, dynamic, thin-sliced (≤ 3 mm), contrast-enhanced CT scan with three specific phases (triphasic) [1][2]:
| Phase | Timing After Contrast | What It Shows | Why It Matters |
|---|---|---|---|
| Arterial phase | ~25–30 seconds | Enhancement of celiac axis, SMA, and peripancreatic arteries | Assesses arterial involvement (SMA, celiac trunk, CHA encasement) → determines resectability [1] |
| Pancreatic (venous) phase | ~40–50 seconds | Maximum attenuation difference between the hypoattenuating tumour and normal enhancing pancreatic parenchyma | This is the phase where the tumour is most conspicuous — PDAC is hypovascular (dense desmoplastic stroma) so it does NOT enhance, while normal pancreas does → the tumour stands out as a dark (hypoattenuating) area [1][2] |
| Portal venous phase | ~70–80 seconds | Enhancement of SMV, splenic vein, and portal vein | Assesses venous involvement (SMV/PV encasement, thrombosis) → determines resectability [1] |
Typical CT findings of pancreatic cancer [1][2][4]:
| Finding | Explanation |
|---|---|
| Ill-defined hypoattenuating mass within the pancreas | The tumour is hypovascular (desmoplastic stroma prevents contrast enhancement) while normal parenchyma enhances brightly → tumour appears darker [1][2] |
| Double duct sign | Simultaneous dilatation of both the pancreatic duct AND CBD with abrupt cutoff at the pancreatic head — pathognomonic of pancreatic head malignancy [1][2][4]. This occurs because the tumour compresses both the intrapancreatic CBD and the main pancreatic duct where they converge at the head |
| Pancreatic duct cutoff | Abrupt termination of pancreatic duct at tumour site |
| Parenchymal atrophy | Upstream glandular atrophy from chronic duct obstruction |
| Contour abnormalities | Irregularity of the pancreatic contour at the site of tumour |
| Vascular encasement | Assessment of tumour contact/encasement of SMA, celiac trunk, hepatic artery, SMV, PV [2][3] |
| Liver metastases | Hypodense liver lesions |
| Ascites | Peritoneal carcinomatosis |
| Lymphadenopathy | Regional or distant nodes |
CT assessment of resectability — the criteria from the lecture [3]:
Criteria of Resectability:
- No distant metastases
- SMA and celiac axis not involved
- Patent superior mesenteric-portal venous confluence
- PV involvement is NOT an absolute contraindication — venous resection is appropriate to improve resectability and achieve R0 resection
- Significant morbidity and mortality
- Reasonable survival: median = 13 months, 5-year = 7%
Expanded NCCN resectability assessment:
| Category | Arterial Criteria | Venous Criteria |
|---|---|---|
| Resectable | No contact with SMA, celiac axis, or CHA | No SMV/PV contact, or ≤ 180° without vein contour irregularity |
| Borderline resectable | Tumour contact < 180° with SMA; CHA contact without extension to celiac axis | > 180° SMV/PV contact, or ≤ 180° with contour irregularity, or thrombosis if reconstructable [2][3] |
| Locally advanced (unresectable) | SMA/celiac trunk encasement > 180° | Unreconstructible SMV/PV due to tumour involvement or thrombus [2][3] |
| Metastatic | Any T, any vessels | Distant metastases present |
Portal Vein Involvement
PV involvement is NOT an absolute contraindication to surgery. Selected patients with limited PV/SMV involvement can undergo venous resection and reconstruction (segmental resection with primary anastomosis or interposition graft). This achieves R0 resection in borderline cases but carries significant morbidity. The lecture notes: median survival = 13 months, 5-year survival = 7% after venous resection [3].
| Aspect | Detail |
|---|---|
| Principle | High-frequency ultrasound transducer on the tip of an endoscope placed in the stomach/duodenum → generates high-resolution images of the pancreas from very close range (no bowel gas or body fat interference) |
| Role in diagnosis | Detects small pancreatic masses that could be missed by CT scan — used when there is high suspicion but no mass on CT [1] |
| EUS-guided tissue sampling | EUS-guided FNAC or biopsy is PREFERRED over percutaneous USG/CT-guided biopsy — less risk of tumour seeding because the needle traverses the GI wall (which will be resected in a Whipple's anyway) rather than crossing the peritoneal cavity [1][2] |
| When tissue diagnosis is NOT required | When suspicion of CA pancreas is HIGH and the tumour appears RESECTABLE on CT → proceed directly to surgery without preoperative biopsy [1][2]. Rationale: resection is both diagnostic and therapeutic; delaying surgery for biopsy provides no benefit and may worsen outcomes |
| When tissue diagnosis IS required | (1) Locally advanced/unresectable disease (need histology before committing to chemo), (2) Patient unfit for surgery, (3) Neoadjuvant therapy is contemplated, (4) CT failed to show typical features or an alternative diagnosis must be excluded (e.g., lymphoma, autoimmune pancreatitis), (5) Suspected secondary metastasis to pancreas [1][2] |
| EUS for chronic pancreatitis vs cancer | Preoperative biopsy is recommended if chronic pancreatitis or autoimmune pancreatitis is suspected since they can closely mimic pancreatic cancer — you do NOT want to do a Whipple's for AIP! [1] |
| Role of EUS in periampullary tumours | EUS helps acquire histological diagnosis of CA head of pancreas (which normally cannot be seen on OGD unless it has invaded through the duodenal wall). EUS has NO role in diagnosing CA ampulla of Vater and CA duodenum (these are visible on duodenoscopy and biopsied directly) [12] |
When NOT to Biopsy
A very common exam mistake: ordering EUS-biopsy for every pancreatic mass. If the tumour is RESECTABLE on CT and clinical suspicion is HIGH, proceed DIRECTLY to surgery. Biopsy delays treatment, risks tumour seeding, and does not change management — the resected specimen provides the definitive pathology [1][2].
| Aspect | Detail |
|---|---|
| Current role | Primarily THERAPEUTIC, not diagnostic — its main indication is biliary decompression via stent placement in patients with cholestasis from tumour obstruction [1] |
| Diagnostic capability | Highly sensitive for visualising the biliary tree and pancreatic ducts; can obtain brush cytology or forceps biopsy from the stricture site [1][2] |
| NOT all patients need preoperative biliary drainage | Not all patients with biliary obstruction from pancreatic cancer require decompression and stenting if the cancer is potentially resectable — routine preoperative biliary stenting in resectable cases increases infectious complications without clear survival benefit. It is reserved for: (a) severely jaundiced patients needing optimisation before surgery, (b) those with cholangitis, (c) delay to surgery > 2 weeks [1] |
| Complications | Post-ERCP pancreatitis, bleeding, cholangitis, perforation [1] |
| When to use | Symptomatic cholestasis requiring palliation, cholangitis, need for brush cytology when EUS is unavailable or non-diagnostic |
| Aspect | Detail |
|---|---|
| Principle | Non-contrast, T2-weighted MRI that highlights fluid-filled structures (bile and pancreatic ducts appear bright) [12] |
| Role | Superior in delineating the anatomy of the biliary tree especially when the system is not obstructed and there are no therapeutic indications for ERCP [1] |
| Advantage over ERCP | Non-invasive, no risk of pancreatitis/perforation, no sedation required |
| Limitation | NOT therapeutic (cannot stent, cannot biopsy) |
| When to use | Equivocal CT findings, need to clarify ductal anatomy, assessment of IPMN and cystic lesions, patients with mild LFT derangement where ERCP is not yet warranted [1][12] |
| Aspect | Detail |
|---|---|
| Current evidence | Data remains insufficient to conclude that PET or PET-CT provides useful information above that provided by contrast-enhanced CT [1] |
| Potential use | May help distinguish chronic pancreatitis from CA pancreas (PDAC is FDG-avid; chronic pancreatitis is usually not — but acute inflammation can cause false positives) [1] |
| Other use | Detecting occult distant metastases when CT is equivocal; staging when equivocal CT findings |
| Aspect | Detail |
|---|---|
| Current evidence | No evidence that MRI offers a significant diagnostic advantage over triple-phase MDCT. MRI currently provides essentially the same information as CT scan [1] |
| When preferred | Patients with contrast allergy (MRI uses gadolinium instead of iodinated contrast), renal impairment (gadolinium is safer in moderate CKD), pregnant patients, characterisation of indeterminate liver lesions (MRI with liver-specific contrast Primovist is superior for small liver lesions) [12] |
| Aspect | Detail |
|---|---|
| Purpose | General exploration of peritoneal surfaces to detect occult peritoneal metastases missed by CT — peritoneal deposits can be very small and are notoriously hard to see on CT [1][2] |
| Value | As CT quality has improved, the value of diagnostic laparoscopy has decreased [1]. However, it still has an important role in select cases |
| Indications [1] | - Tumours located in body or tail (higher rate of occult peritoneal mets) |
| - Large tumours > 4 cm | |
| - High CA 19-9 level | |
| - Equivocal findings of metastasis or ascites on CT scan | |
| - Before resection is attempted for body/tail lesions [1] |
| Sign | Modality | Meaning |
|---|---|---|
| Double duct sign | CT / MRCP | Simultaneous dilatation of CBD + pancreatic duct with cutoff at pancreatic head → highly suggestive of periampullary malignancy [1][2][4] |
| Hypoattenuating pancreatic mass | CT (pancreatic phase) | PDAC — dense desmoplastic stroma prevents contrast enhancement [1][2] |
| Pancreatic duct cutoff | CT / MRCP | Abrupt termination of duct at tumour site |
| Vascular encasement | CT (arterial + PV phases) | Determines resectability (SMA, celiac, CHA, SMV, PV) [2][3] |
| CBD dilatation > 0.8 cm | USG | Suggests distal obstruction [12] |
| Pancreatic duct dilatation > 3 mm | USG / CT | Suggests duct obstruction; in pancreatic head cancer, upstream dilatation |
| "Sausage-shaped" pancreas | CT | Autoimmune pancreatitis (important mimic!) |
| Diffuse calcifications | CT / AXR | Chronic pancreatitis (important mimic) [7] |
| Hyperenhancing mass | CT (arterial phase) | PanNET or metastasis (NOT PDAC) [10] |
This is one of the most tested concepts — when do you biopsy and when do you go straight to surgery?
Special Considerations
Why does this matter? Obstructive jaundice → bile salts cannot reach gut → fat malabsorption → vitamin K deficiency → reduced synthesis of coagulation factors II, VII, IX, X → prolonged PT/INR. Before any invasive procedure (ERCP, EUS-FNAC, surgery), you must:
This is a nuanced clinical question:
- Routine preoperative biliary stenting is NOT recommended for all patients — it increases infective complications (cholangitis, wound infection post-Whipple) without clear survival benefit
- Indications for preoperative drainage: (a) bilirubin > 250–300 μmol/L (severe jaundice impairs hepatic function and increases surgical risk), (b) cholangitis, (c) expected delay to surgery > 2–4 weeks, (d) neoadjuvant therapy planned (patient needs biliary decompression during chemo months) [1]
High Yield Summary — Diagnosis and Investigations
-
Pancreatic protocol CT (thin-sliced triphasic) is the GOLD STANDARD for diagnosis AND staging simultaneously.
-
Triphasic = arterial (arteries/resectability) + pancreatic/venous (tumour conspicuity) + portal venous (veins/resectability).
-
Classic CT finding: ill-defined hypoattenuating mass + double duct sign + vascular encasement.
-
Tissue diagnosis (biopsy) is NOT mandatory if the tumour is resectable — proceed to surgery. Biopsy is needed only for unresectable/metastatic disease, atypical features, neoadjuvant planning, or to exclude mimics.
-
EUS-guided FNAC is preferred over percutaneous biopsy (lower risk of peritoneal tumour seeding).
-
CA 19-9 is NOT diagnostic — it is prognostic and used for monitoring. Requires Lewis antigen expression.
-
Resectability criteria: No distant mets, SMA/celiac not encased > 180°, patent SMV-PV confluence (PV involvement is NOT an absolute contraindication if reconstructable).
-
Staging laparoscopy is indicated for body/tail tumours, large tumours > 4 cm, high CA 19-9, or equivocal CT findings.
-
Courvoisier's sign: Painless jaundice + palpable GB → malignant biliary obstruction. Exceptions: double gallstones, RPC.
-
Correct coagulopathy (IV vitamin K) before any invasive procedure in jaundiced patients.
Active Recall - Diagnosis and Investigations of Pancreatic Cancer
References
[1] Senior notes: felixlai.md (Pancreatic cancer — Diagnosis section) [2] Senior notes: maxim.md (Pancreatic carcinoma — Investigations, Staging, Resectability sections) [3] Lecture slides: Malignant biliary obstruction.pdf (p8 — tumour markers table; p23 — criteria of resectability) [4] Lecture slides: WCS 056 - Painless jaundice and epigastric mass - by Prof R Poon.ppt (1).pdf (p41 — CT showing pancreatic head mass and duct dilatation) [7] Senior notes: maxim.md (Chronic pancreatitis section) [10] Senior notes: maxim.md (Non-functioning pNET vs CA pancreas table) [11] Senior notes: felixlai.md (Malignant biliary obstruction — Courvoisier's law, biochemical tests) [12] Senior notes: maxim.md (HBP investigations — USG, EUS, MRCP, PTC, ERCP)
Management of Pancreatic Cancer
The management of pancreatic cancer is governed by two parallel assessments that must be made before any treatment decision [1][3][4]:
- Patient general status — Is the patient fit enough for major surgery? (age, comorbidities, nutrition, organ function)
- Tumour status — Is the tumour confined (resectable) or has it spread (unresectable/metastatic)?
The lecture slide by Prof R Poon elegantly summarises this decision framework [4]:
General status: good → laparotomy; bad → PTBD or endoprosthesis Tumour status: confined → laparotomy → radical resection if confined, bypass if spread; spread → PTBD or endoprosthesis
The lecture on MBO further distils the approach [3]:
MBO → Treat SEPSIS → (1) Assess tumour resectability, (2) Patient general fitness, (3) Liver function reserve → Resectable vs. Non-resectable → Resectable = Surgery; Non-resectable = Palliation
The single most critical teaching point: Surgical treatment is the ONLY potentially curative treatment for pancreatic cancer, but only 15–20% of patients are surgical candidates because the majority present with locally advanced or metastatic disease [1][2][4].
Before any surgery for pancreatic cancer, several issues must be addressed. These patients are high-risk because of the combination of cancer cachexia + obstructive jaundice + malnutrition + coagulopathy [1][11]:
| Issue | Problem | Intervention |
|---|---|---|
| Cancer cachexia → Malnutrition | Poor wound healing, immunosuppression, increased surgical risk | Nutritional support (enteral preferred: oral supplements, nasojejunal feeding) [1][11] |
| Liver derangement → Bleeding tendency | Vitamin K deficiency from bile salt malabsorption → ↓ factors II, VII, IX, X → prolonged PT/INR | IV Vitamin K (takes 24–48h) + FFP during surgery if needed [1][11] |
| Superimposed biliary infection | Cholangitis risk from biliary stasis | Antibiotic cover (e.g., Augmentin OR Cefuroxime + Metronidazole) [1][11][13] |
| Electrolyte abnormalities | Hyponatraemia, hypokalaemia from vomiting/poor intake | Correct preoperatively |
| Blood products | Major vascular surgery risk | Type and screen / crossmatch |
Preoperative Biliary Drainage — A Nuanced Decision
This is one of the most commonly tested management dilemmas:
| Aspect | Detail |
|---|---|
| Methods | ERCP with endoprosthesis (stenting) or PTBD [1][2] |
| Target | Serum bilirubin < 50 μmol/L [1][11] |
| Theoretically | Do NOT need to drain if no sepsis + early surgery can be offered within 1–2 weeks — preoperative biliary drainage increases risk of serious complications (cholangitis, pancreatitis, perforation) even in expert hands, while surgical-related complications are comparable without drainage [1][2][11] |
| Practically at QMH | Drain ALL patients since QMH cannot offer early surgery — Whipple operation has to wait 6–8 weeks, and the chance of biliary sepsis will be very high without drainage while waiting [1][11] |
| Stent choice | Plastic stent is preferred for preoperative drainage (cf. metal stent which induces inflammation → difficult removal in OT) [2]; Metallic stent (SEMS) is preferred if confirmed inoperable since it is more durable [1][13] |
| Advantages | Minimise cholangitis risk, relieve jaundice/pruritus, prevent cholestatic complications, allow time for neoadjuvant therapy [1][11] |
| Disadvantages | Increase interventions and costs, procedure-related complications (cholangitis, pancreatitis, bleeding, perforation, blocked stent) [1][11] |
| Indications for preop drainage | (1) Biliary sepsis/cholangitis, (2) Surgery cannot be arranged within 1–2 weeks, (3) Severe jaundice (bilirubin > 250–300 μmol/L), (4) Neoadjuvant therapy planned [1][2] |
Pre-op ERCP for biliary drainage: NOT routine, only if septic / OT cannot be arranged in 1–2 weeks. Plastic stent is preferred [2].
Preoperative Drainage — Theory vs. Practice
In exams, the "textbook" answer is: do NOT drain routinely if early surgery is possible (evidence shows drainage increases infections without improving outcomes). But the practical QMH answer is: drain ALL because surgical wait times are long (6–8 weeks) and the risk of biliary sepsis during this period is unacceptable [1][11]. Know both perspectives.
2. Curative Treatment — Surgical Resection
Principle: Upfront pancreatectomy (+ local lymphadenectomy) + adjuvant chemotherapy (ALL cases) ± RT [2].
The lecture slide explicitly states the criteria of resectability [3]:
Criteria of Resectability:
- No distant metastases
- SMA and celiac axis not involved
- Patent superior mesenteric-portal venous confluence
- PV involvement is NOT an absolute contraindication
- Venous resection is appropriate to improve resectability and achieve R0 resection
- Significant morbidity and mortality
- Reasonable survival: median = 13 months, 5-year = 7% [3]
Absolute contraindications to resection [2]:
| Contraindication | Reason |
|---|---|
| SMA / celiac trunk encasement > 180° | Cannot safely reconstruct; attempting resection = unacceptably high morbidity |
| Unreconstructible SMV / portal vein | No suitable vessel proximal and distal for interposition graft |
| Distant metastasis | Systemic disease — surgery does not improve survival |
Borderline resectable (may still be resectable after neoadjuvant therapy) [2]:
- Tumour contact < 180° with SMA (relative, not absolute contraindication)
- SMV/PV involvement but suitable vessel proximal and distal for interposition graft reconstruction
| Aspect | Detail |
|---|---|
| Purpose | No promise of resection until laparotomy/laparoscopy documents absence of spread [1][11] |
| Technique | General exploration of peritoneal surfaces; look for peritoneal nodules → send for frozen section to rule out malignancy if suspicious [1][11] |
| Indications | Body/tail tumours, large tumours > 4 cm, high CA 19-9, equivocal CT findings [1] |
| Intra-op USG | Used to rule out liver metastases not seen on preop imaging [2] |
| If metastases found | Surgery should be aborted → convert to palliative management [1] |
C. Whipple's Operation (Pancreaticoduodenectomy) — For Head/Uncinate Tumours
The lecture explicitly states: "Whipple operation for carcinoma of pancreas, distal CBD cholangiocarcinoma, CA duodenum and CA ampulla" [3].
Prof R Poon's slide: "Line of resection of pancreatic head cancer — Whipple operation or pancreaticoduodenectomy" [4].
| Structure Resected | Reason |
|---|---|
| Pancreatic head | Contains the tumour |
| Duodenum (D1–D4 or D2–D4) | Shares blood supply with pancreatic head (via pancreaticoduodenal arteries); cannot survive without pancreatic head blood supply |
| First 15 cm of jejunum | Distal to ligament of Treitz, included for oncological margin |
| Common bile duct | Runs through/behind pancreatic head; must be transected and reconstructed |
| Gallbladder + cystic duct | Removed with CBD |
| Partial gastrectomy (classic Whipple) OR preservation of pylorus (PPPD) | See below |
| Regional lymphadenectomy | Take at least 12 LN for accurate staging [2] — LN around SMA, para-aortic |
| Feature | PPPD (Standard, preferred) | Classic Whipple |
|---|---|---|
| What is preserved | Gastric antrum, pylorus, proximal 3–6 cm of duodenum [1][2] | Antrectomy + truncal vagotomy |
| When to use classic Whipple | — | Only when entire duodenum must be removed (e.g. FAP) or PPPD cannot achieve clear margin (tumour encroaches on D1/distal stomach) [2] |
| Survival/recurrence | No difference vs. classic Whipple [2] | Same |
| Operative advantage | Less blood loss, shorter operative time [2] | — |
| Dumping syndrome | Lower rate [1][2] | Higher (post-gastrectomy dumping) |
| Marginal ulceration | Lower rate [1][2] | Higher (mucosal erosion at GJ) |
| Bile reflux gastritis | Lower rate (difficult to manage) [1][2] | Higher |
| Delayed gastric emptying | Similar or slightly higher (controversial) [2] | Similar |
| Nutritional outcomes | Improved post-operative nutrition [1] | Poorer |
After resection, GI continuity is restored via Roux-en-Y reconstruction with three anastomoses (performed in this specific order) [2]:
| Anastomosis | Abbreviation | What It Connects | Key Points |
|---|---|---|---|
| 1. Pancreaticojejunostomy (PJ) | PJ | Pancreatic remnant → jejunum | Highest risk of leak (30%) due to digestive enzymes + small/soft duct [2]. Done FIRST because it is deepest in the operative field |
| 2. Choledochojejunostomy (CJ) | CJ | Remaining bile duct → jejunum | Restores biliary drainage |
| 3. Gastrojejunostomy (GJ) or Duodenojejunostomy (DJ) | GJ/DJ | Stomach/duodenal stump → jejunum | Restores alimentary continuity; DJ in PPPD, GJ in classic Whipple |
Why this order? The PJ is the deepest (most posterior) anastomosis — you do the deepest one first because it becomes inaccessible once the more superficial ones are done.
Why Is PJ Leak the Most Dangerous Complication?
The pancreatic remnant leaks activated digestive enzymes (lipase, trypsin, elastase) into the peritoneal cavity or retroperitoneum. These enzymes can: (1) Erode blood vessels → GDA pseudoaneurysm → catastrophic haemorrhage, (2) Cause portal/splenic vein thrombosis, (3) Create pancreatic fistula → dehydration, malnutrition, metabolic acidosis (loss of HCO₃⁻-rich pancreatic juice). Risk factors: high BMI, soft pancreas, narrow duct [2][14].
| Aspect | Detail |
|---|---|
| Indication | Lesions of the body or tail [1][2] |
| Procedure | Resection of pancreas lateral to SMV + splenectomy + local lymphadenectomy [2] |
| Why splenectomy? | The splenic artery and vein run intimately along the superior and posterior border of the pancreas body/tail; en-bloc removal provides oncological margin. Splenic vessel preservation is sometimes attempted (Warshaw technique) but not for cancer |
| Post-splenectomy care | Vaccination for encapsulated organisms (Streptococcus pneumoniae, Haemophilus influenzae type b, Neisseria meningitidis) — ideally ≥ 2 weeks before elective splenectomy or ASAP postop [2] |
| Staging laparoscopy first | In the rare patient with potentially resectable body/tail disease, laparoscopic exploration should be performed FIRST to rule out occult metastasis missed by CT [1] |
| Prognosis | Poor — most body/tail cancers are advanced at presentation; higher anastomotic leak rate compared to Whipple's [2] |
| Aspect | Detail |
|---|---|
| Indications | Multifocal tumour (e.g. main-duct IPMN) or when body/tail of pancreas is too inflamed to achieve a safe anastomosis with bowel [2] |
| Consequence | Complete exocrine and endocrine insufficiency → lifelong pancreatic enzyme replacement + insulin therapy (brittle diabetes) |
| Advantage | Eliminates risk of PJ leak (no pancreatic remnant to anastomose) |
Summary of surgery by tumour location — from the lecture [3]:
"Whipple operation for carcinoma of pancreas, distal CBD cholangiocarcinoma, CA duodenum and CA ampulla" "Radical cholecystectomy for CA gallbladder" "Major hepatectomy + caudate lobectomy together with confluence of hepatic ducts for Klatskin tumour" [3]
| Aspect | Detail |
|---|---|
| Indication | ALL resected CA pancreas — no exceptions [2] |
| Timing | Start within 12 weeks post-op [2] |
| Regimens | FOLFIRINOX (folinic acid + 5-FU + irinotecan + oxaliplatin) — preferred if fit (PRODIGE-24 trial showed superior OS); OR Gemcitabine + capecitabine × 6 months (ESPAC-4 trial) [1][2] |
| Rationale | Evidence suggests adjuvant therapy increases survival [1]. Even after R0 resection, micrometastatic disease is presumed present — adjuvant chemo targets these microscopic deposits |
| Benefit | Clear benefit to adjuvant therapy in CA pancreas [1]; mFOLFIRINOX increases median OS from ~35 months to ~54 months in selected patients (PRODIGE-24) |
Adjuvant Chemo Is Non-Negotiable
Every single patient who undergoes curative resection for pancreatic cancer should receive adjuvant chemotherapy. This is one of the strongest evidence-based recommendations in pancreatic surgery. Even node-negative patients benefit [2].
| Aspect | Detail |
|---|---|
| Goal | Downstage patients with borderline resectable disease to make R0 resection achievable [1] |
| Regimens | FOLFIRINOX or Gemcitabine + nab-paclitaxel ± chemoradiation |
| Duration | Typically 4–6 months → restage with CT → surgery if response/stable disease |
| Tissue diagnosis | Required before neoadjuvant therapy — EUS-guided biopsy [1][2] |
| Evidence | Growing evidence that neoadjuvant approach may be superior to upfront surgery even for resectable disease (PREOPANC-2, NEONAX trials), but current standard remains upfront surgery for clearly resectable tumours |
5. Palliative Treatment — For Unresectable / Metastatic Disease
The three pillars of palliation (from the lecture) [1][3]:
Palliative care:
- Treat sepsis
- Relieve obstruction (enteric / biliary)
- Pain control [3]
When you open the abdomen expecting to resect but find unresectable disease (occult mets/vascular invasion) [2]:
| Action | Purpose | Details |
|---|---|---|
| Double bypass surgery | Prevent future obstruction | Performed prophylactically because the patient is already open |
| → Gastric bypass: Gastroenterostomy | Relieve / prevent duodenal obstruction | Connects stomach to jejunum, bypassing the duodenum |
| → Biliary bypass: Choledochoenterostomy | Relieve jaundice | Connects CBD to jejunum, bypassing the distal obstruction |
| Transduodenal trucut biopsy | Obtain tissue for histological confirmation and guide chemotherapy | DDx includes lymphoma (which has completely different treatment) [2] |
| ± Celiac plexus block | Pain control | Inject alcohol/phenol into celiac plexus under direct vision while abdomen is open [2] |
Why not choledochoduodenostomy? Choledochoduodenostomy is NOT advised because of the proximity of the duodenum to the tumour — the tumour will eventually grow into and obstruct the anastomosis [1].
Scenario B: Tumour Found Unresectable on Imaging (Never Goes to OR)
| Action | Details |
|---|---|
| ERCP stenting (SEMS preferred) | Biliary stent ± duodenal stent to relieve jaundice and GOO without surgery [2] |
| PTBD if ERCP fails or is contraindicated | External or external-internal drainage [1][2] |
| Systemic chemotherapy | First obtain EUS-guided biopsy for tissue diagnosis (must exclude lymphoma) [2] |
| Chemotherapy regimens | FOLFIRINOX (folinic acid + 5-FU + irinotecan + oxaliplatin) if fit; Gemcitabine + nab-paclitaxel if borderline fit; Gemcitabine monotherapy if poor PS [1][2] |
ERCP with endoprosthesis is ALWAYS 1st line regardless of the level of obstruction especially for periampullary carcinoma [13], except:
| ERCP Contraindication | Then Use PTBD |
|---|---|
| Structural upper GI abnormalities (oesophageal diverticulum, stricture, paraesophageal hernia) | PTBD |
| Gastric surgery (Billroth II, Roux-en-Y — altered anatomy makes endoscopic access to ampulla impossible) | PTBD |
| Multiple stenting required / difficulty reaching intrahepatic bile ducts | PTBD |
| Failed ERCP | PTBD |
ERCP is preferred over PTBD because [13]:
- PTBD is technically more difficult
- PTBD has risk of bleeding from puncture of hepatic artery or portal vein (portal triad traversed during puncture)
- If bleeding occurs: stabilise → clamp PTBD catheter → cholangiogram via catheter to identify location → remove catheter slowly to control bleeding → do NOT remove immediately (converts to free haemoperitoneum) [13]
| Stent Type | When to Use | Properties |
|---|---|---|
| Plastic stent | Preoperative drainage (temporary, removable) | Cheaper but shorter patency (~3 months), tends to occlude with sludge |
| Self-expandable metallic stent (SEMS) | Confirmed inoperable (long-term palliation) | Longer patency (~6–12 months), cannot be removed; uncovered stents preferred (lower risk of occluding branch bile ducts) [14] |
Stent complications [1][13][14]:
- Stent occlusion (sludge, tumour ingrowth, tumour overgrowth) → managed by sweeping or placing new stent
- Stent migration
- Cholangitis / Cholecystitis
| Type | Indication | Detail |
|---|---|---|
| Simple external PTBD | Short-term drainage to bridge to surgery | Catheter drains bile externally; prone to electrolyte and fluid loss due to bile output |
| External-internal PTBD | Long-term palliation | Catheter pushed past the obstruction and internalized → bile drains into duodenum |
| Symptom | Management | Mechanism |
|---|---|---|
| Pain | Narcotics (e.g. morphine) — WHO analgesic ladder; Celiac plexus neurolysis (block) — EUS-guided or CT-guided injection of alcohol/phenol into celiac plexus, destroys pain fibres; Short-course RT for local pain control [1][2] | Celiac plexus carries visceral pain afferents from the pancreas — chemical ablation interrupts pain transmission |
| Exocrine insufficiency | Pancreatic enzyme replacement therapy (PERT) — e.g. Creon (pancrelipase) taken with meals | Replaces missing lipase/protease/amylase for digestion |
| Endocrine insufficiency | OHA / insulin [2] | Replaces lost β-cell function |
| Nutritional support | Dietary counselling, oral supplements, NJ feeding if needed | Counteracts cachexia and malabsorption |
| Thromboembolic disease | Anticoagulation (LMWH) for Trousseau syndrome / VTE | Addresses hypercoagulable state |
| Pruritus | Cholestyramine (bile acid sequestrant), rifampicin, biliary drainage | Removes bile salts from skin/circulation |
| Setting | Regimen | Notes |
|---|---|---|
| Adjuvant (post-resection) | FOLFIRINOX (preferred if fit) or Gemcitabine + capecitabine × 6 months [2] | Start within 12 weeks postop |
| Neoadjuvant (borderline resectable) | FOLFIRINOX or Gemcitabine + nab-paclitaxel ± CRT | 4–6 months → restage |
| First-line palliative (fit, PS 0–1) | FOLFIRINOX [2] | Superior OS vs. gemcitabine alone; significant toxicity |
| First-line palliative (borderline fit) | Gemcitabine + nab-paclitaxel | Better tolerated than FOLFIRINOX |
| First-line palliative (poor PS) | Gemcitabine monotherapy [1] | Results in symptomatic improvement, improved pain control, performance status and weight gain [1] |
| BRCA-mutated PDAC (maintenance) | Olaparib (PARP inhibitor) | After ≥ 16 weeks of platinum-based chemo without progression (POLO trial) |
FOLFIRINOX Explained
FOLFIRINOX = FOLinic acid (leucovorin) + Fluorouracil (5-FU) + IRINotecan (topoisomerase I inhibitor) + OXaliplatin (platinum agent). This is the most active regimen for PDAC but carries significant toxicity (myelosuppression, diarrhoea, neuropathy). Reserved for fit patients with good performance status [2].
From the lecture by Prof R Poon [4]:
Long-term survival of pancreatic head cancer:
1-year 5-year After radical resection 66% 27% Palliative bypass 10% 0%
This starkly illustrates why resection is pursued so aggressively when possible — it is the only chance of meaningful long-term survival.
Additional survival data [1]:
- 5-year survival after pancreaticoduodenectomy, node-negative = 25–30%
- 5-year survival after pancreaticoduodenectomy, node-positive = ~10%
- Median survival for unresectable locally advanced = 12 months
- Median survival for metastatic disease = 6 months
| Timing | Complication | Detail |
|---|---|---|
| Early | Haemorrhage | Intraoperative vascular injury or postop GDA pseudoaneurysm erosion from PJ leak |
| Anastomotic leak | Risk: PJ (30%) > CJ > GJ [2]; PJ highest because of digestive enzymes + small/soft duct | |
| Pancreatic fistula | Drain output after postop D3 with amylase > 3× ULN [14]; classified by ISGPF: Biochemical leak (asymptomatic) → Grade B (persistent drainage > 3 weeks, infection, no organ failure) → Grade C (unstable, re-operation, organ failure) | |
| Delayed gastric emptying (common) | Especially in PPPD; mechanisms: injury to nerve of Latarjet, disrupted pacemaker cells, reduced CCK (high in duodenum) [2] | |
| Wound infection | Especially if preop biliary stenting (contaminated bile) | |
| Intra-abdominal abscess | From leak or infection | |
| Post-ERCP pancreatitis | If preop stenting performed | |
| Late | Exocrine insufficiency | Malabsorption and steatorrhoea → PERT [1] |
| Endocrine insufficiency | DM (16% new-onset) [2] → insulin/OHA | |
| Gastric stasis | Especially in PPPD patients [1] | |
| Marginal ulceration | Mucosal erosion at GJ (more common in classic Whipple) | |
| Dumping syndrome | More common in classic Whipple (removed pylorus) |
Pancreatic Fistula Management [14]
| Grade | Management |
|---|---|
| Biochemical leak | Maintain oral feeding, drain in situ for 3 weeks |
| Grade B (symptomatic) | NPO, NJ feeding, correct fluid and electrolytes, drain in situ, antibiotic prophylaxis, somatostatin analogue |
| Persistent/Grade C | Endoscopic transpapillary stent; surgical repair; embolization for bleeding |
| Stage | Treatment | Key Points |
|---|---|---|
| Resectable | Upfront surgery → Adjuvant chemo (ALL cases) | Whipple (head), distal pancreatectomy (body/tail); PPPD preferred; take ≥ 12 LN |
| Borderline resectable | Neoadjuvant chemo ± CRT → Restage → Surgery if response | FOLFIRINOX or Gem/nab-paclitaxel; tissue diagnosis required first |
| Locally advanced | Definitive chemo ± RT; palliative stenting | Conversion surgery in exceptional responders |
| Metastatic | Palliative chemo + symptom control | FOLFIRINOX (fit) or Gem-based; biliary/duodenal stenting; celiac plexus block |
| All stages | Symptom management: pain (opioids, celiac block), jaundice (stent), GOO (duodenal stent/GJ), exocrine insufficiency (PERT), DM (insulin) | Multidisciplinary team approach |
High Yield Summary — Management
-
Only 15–20% of patients are surgical candidates — surgery is the only potentially curative treatment.
-
Assessment framework: General status (fit/unfit) + Tumour status (confined/spread) → determines surgery vs. palliation.
-
Resectability criteria: No distant mets, SMA/celiac not involved, patent SMV-PV confluence. PV involvement is NOT an absolute contraindication (venous resection for R0: median 13 months, 5-year 7%).
-
Whipple operation: For head/periampullary tumours. PPPD preferred (less dumping, less marginal ulcer, less bile reflux, better nutrition). Triple anastomosis: PJ → CJ → GJ/DJ.
-
Adjuvant chemotherapy is given to ALL resected patients — FOLFIRINOX (preferred) or Gemcitabine + capecitabine × 6 months. Start within 12 weeks.
-
Preop biliary drainage: NOT routine if early surgery possible; practically at QMH: drain ALL (long wait times). Plastic stent preop; SEMS if confirmed inoperable.
-
Palliative triad: Treat sepsis + Relieve obstruction (biliary stent/bypass, duodenal stent/GJ) + Pain control (opioids, celiac plexus block).
-
Unresectable at laparotomy → Double bypass (GJ for GOO + choledochoenterostomy for jaundice) + biopsy + celiac plexus block.
-
ERCP stenting is 1st line for biliary palliation (over PTBD). SEMS preferred for palliation (longer patency). PTBD if ERCP fails.
-
PJ leak is the most feared complication of Whipple (30% risk) → can cause GDA pseudoaneurysm, haemorrhage, pancreatic fistula.
-
Long-term survival after radical resection: 1-year 66%, 5-year 27%. Palliative bypass: 1-year 10%, 5-year 0%.
Active Recall - Management of Pancreatic Cancer
References
[1] Senior notes: felixlai.md (Pancreatic cancer — Treatment section, Preoperative biliary drainage, Whipple operation, Distal pancreatectomy, Prognosis) [2] Senior notes: maxim.md (Pancreatic carcinoma — Curative treatment, Whipple operation, PPPD, Distal pancreatectomy, Adjuvant chemotherapy, Palliative treatment) [3] Lecture slides: Malignant biliary obstruction.pdf (p18 — MBO management framework; p21 — surgical operations by tumour type; p23 — criteria of resectability; p30 — palliative care) [4] Lecture slides: WCS 056 - Painless jaundice and epigastric mass - by Prof R Poon.ppt (1).pdf (p9 — Whipple line of resection; p54 — general status/tumour status flowchart; p76 — long-term survival data) [11] Senior notes: felixlai.md (Malignant biliary obstruction — Preoperative measures, Courvoisier's law, ERCP/PTBD section) [13] Senior notes: felixlai.md (MBO treatment — ERCP vs PTBD, stent types, palliative bypass, PTBD complications) [14] Senior notes: maxim.md (Pancreatic fistula — ISGPF classification, management; methods to reduce PJ leakage; stent types for cholangioCA)
Complications of Pancreatic Cancer
Complications of pancreatic cancer can be categorised into three broad groups: (A) complications of the disease itself (from tumour progression), (B) complications of treatment (surgical and non-surgical), and (C) causes of mortality. Understanding these from first principles is critical — every complication traces back to either the tumour's anatomical effects, its systemic biological impact, or the consequences of removing/manipulating vital structures.
A. Complications of the Disease (Untreated / Progressive Pancreatic Cancer)
These occur as the tumour grows locally, invades adjacent structures, metastasises, or exerts systemic paraneoplastic effects.
| Complication | Pathophysiology | Clinical Consequence |
|---|---|---|
| Progressive obstructive jaundice | Head tumour gradually compresses/invades the intrapancreatic CBD → complete biliary obstruction | Conjugated hyperbilirubinaemia → jaundice, pruritus, dark urine, pale stools. If untreated: coagulopathy (vitamin K malabsorption), malabsorption, malnutrition, and immune dysfunction [3] |
| Acute cholangitis [1] | Biliary stasis proximal to obstruction → bacterial colonisation of static bile (normally bile is sterile, but stasis allows ascending infection from duodenum) → suppurative infection of the biliary tree | Charcot's triad (fever/rigors, jaundice, RUQ pain) → can progress to Reynolds' pentad (+ hypotension + confusion) = biliary sepsis. Biliary sepsis is a leading cause of mortality in MBO [3][15] |
| Secondary biliary cirrhosis | Prolonged biliary obstruction → chronic cholestasis → periductal fibrosis → eventually cirrhosis | Rare (requires months–years of obstruction); liver failure in advanced cases |
Why Is Cholangitis Dangerous in Pancreatic Cancer?
In a normal biliary system, the sphincter of Oddi prevents reflux of duodenal bacteria into the bile duct. When a tumour obstructs the distal CBD, bile stagnates → bacteria ascend from the duodenum into the stagnant bile → multiply → cholangitis. If not treated urgently with antibiotics + biliary decompression (ERCP stenting or PTBD), this progresses to biliary sepsis — one of the three major causes of death in MBO [3][15].
| Complication | Pathophysiology | Clinical Feature |
|---|---|---|
| Acute pancreatitis [1] | Tumour occludes the main pancreatic duct → upstream ductal hypertension → premature activation of pancreatic enzymes (trypsinogen → trypsin) → autodigestion of pancreatic parenchyma | Acute epigastric pain radiating to back, ↑ amylase/lipase > 3× ULN. Unexplained pancreatitis in an elderly patient without obvious cause (no gallstones, no alcohol) should prompt imaging for occult pancreatic cancer |
| Exocrine insufficiency | Pancreatic duct obstruction → loss of exocrine enzyme delivery (lipase, amylase, proteases) to duodenum; clinically significant when > 90% function is lost | Steatorrhoea (bulky, pale, foul-smelling, floating stools), maldigestion, malabsorption, fat-soluble vitamin deficiency (A, D, E, K), weight loss |
| Endocrine insufficiency | Tumour destroys islets of Langerhans + secretes diabetogenic factors (adrenomedullin, S100A8) | New-onset DM — present in ~50% at diagnosis [1] |
| Complication | Pathophysiology | Presentation |
|---|---|---|
| Gastric outlet obstruction (GOO) | Head/uncinate tumour invades or externally compresses the duodenum (D2/D3) → mechanical obstruction of gastric outflow | Persistent vomiting (often non-bilious if obstruction above ampulla, bilious if below), abdominal distension, succession splash, dehydration, hypokalaemic hypochloraemic metabolic alkalosis (from loss of HCl in vomit), aspiration pneumonia risk [1][2] |
| GI bleeding | Tumour erosion into duodenal mucosa or peripancreatic vessels (GDA, splenic artery) | Melaena, haematemesis, iron-deficiency anaemia |
| Duodenal obstruction | Direct invasion | Similar to GOO; managed by duodenal stenting or gastrojejunostomy [2] |
| Complication | Pathophysiology | Clinical Feature |
|---|---|---|
| Venous thromboembolism (Trousseau syndrome) | Tumour-elaborated procoagulants (tissue factor, cancer procoagulant — a cysteine protease that directly activates factor X) + platelet-aggregating factors → hypercoagulable state | Migratory superficial thrombophlebitis, DVT, PE. ↑ Risk of both arterial and venous thromboembolic events [1] |
| Portal vein / SMV thrombosis | Direct tumour invasion or compression of PV/SMV | Portal hypertension → splenomegaly, ascites, variceal bleeding. Can cause mesenteric ischaemia (SMV thrombosis → compromise bowel perfusion) |
| Splenic vein thrombosis | Body/tail tumours directly invade or compress the splenic vein (runs along posterior/superior border of pancreatic body) | Left-sided (sinistral) portal hypertension → isolated gastric varices (NOT oesophageal) → risk of upper GI bleeding |
| GDA pseudoaneurysm | Pancreatic enzyme leak (from tumour erosion or post-op fistula) erodes into the GDA wall → weakening → pseudoaneurysm formation | Sentinel bleed → catastrophic intra-abdominal haemorrhage or UGIB. Three signs suggestive of pseudoaneurysm: unexplained GI bleeding, unexplained drop in Hb/Hct, sudden expansion of a pancreatic fluid collection [15] |
| Site | Complication | Pathophysiology |
|---|---|---|
| Liver (most common) | Hepatomegaly, liver failure, ascites, jaundice (from intrahepatic mets even without head tumour) | Tumour replaces functional hepatic parenchyma → synthetic failure (↓ albumin, ↓ clotting factors), portal hypertension |
| Peritoneum | Malignant ascites, bowel obstruction | Peritoneal carcinomatosis → exudative ascites (high protein, high LDH, positive cytology), serositis, and adhesions causing mechanical small bowel obstruction |
| Lung | Dyspnoea, cough, haemoptysis, pleural effusion | Haematogenous spread; malignant pleural effusion (exudative) |
| Bone | Pathological fractures, bone pain, hypercalcaemia | Osteolytic/osteoblastic metastases |
| Complication | Mechanism |
|---|---|
| Trousseau syndrome | Discussed above under vascular complications [1] |
| Pancreatic panniculitis | Systemic spillage of excess digestive pancreatic enzymes (especially lipase, particularly in acinar cell carcinoma variant) → autodigestion of subcutaneous fat → erythematous subcutaneous nodular fat necrosis, typically on legs [1] |
| Depression | Occurs with disproportionate frequency even before diagnosis; mechanism unclear (cytokine-mediated central effects, IL-6/TNF-α) |
| Complication | Mechanism |
|---|---|
| Cancer cachexia | Tumour-derived cytokines (TNF-α, IL-6, IL-1) → proteolysis-inducing factor → skeletal muscle wasting, adipose tissue loss, anorexia. Cancer cachexia is a leading cause of mortality in MBO [15][16] |
| Malnutrition | Combination of: (1) maldigestion/malabsorption (exocrine insufficiency + bile salt deficiency), (2) anorexia from cytokines, (3) GOO preventing adequate intake |
| Fat-soluble vitamin deficiency | Vitamin K → coagulopathy; Vitamin D → osteomalacia; Vitamin A → night blindness; Vitamin E → neuropathy |
B. Complications of Treatment
1. Whipple's Operation (Pancreaticoduodenectomy) — Specific Surgical Complications
This is one of the most technically demanding operations in surgery, with a perioperative mortality of 2–5% in high-volume centres and a morbidity rate of 30–50%.
| Complication | Incidence | Pathophysiology | Management |
|---|---|---|---|
| Pancreaticojejunostomy (PJ) leak | ~30% [2] | Highest leak risk of the three anastomoses because: (1) pancreatic enzymes actively digest the anastomosis, (2) the pancreatic duct is often small and soft (normal pancreas without upstream dilatation), (3) the parenchyma is friable. Leak of activated digestive enzymes causes local tissue destruction | Biochemical leak (asymptomatic): maintain oral feeding, drain in situ for 3 weeks. Symptomatic (Grade B): NPO, NJ feeding, correct fluids/electrolytes, drain in situ, antibiotics, somatostatin analogue. Grade C: re-operation, may require completion distal pancreatectomy [2][14] |
| Pancreatic fistula | Related to PJ leak | Definition: drain output of any volume after post-op day 3 with drain amylase > 3× ULN [2][14]. Risk factors: high BMI, soft pancreas, narrow duct [2] | As above (ISGPF classification — biochemical leak, Grade B, Grade C) [14] |
| GDA pseudoaneurysm | Rare but lethal | PJ leak → pancreatic enzymes (elastase) erode into GDA stump → pseudoaneurysm → rupture → catastrophic intra-abdominal haemorrhage or UGIB [2][14][15] | Angiography (diagnostic + therapeutic embolisation); if unstable → emergency re-laparotomy |
| Portal / splenic vein thrombosis | PJ leak → local inflammation → venous thrombosis [2][14] | Anticoagulation; monitor for mesenteric ischaemia | |
| Biliary anastomotic leak (CJ) | Less common than PJ | Bile leak from choledochojejunostomy → bile peritonitis | Percutaneous drainage ± re-operation |
| Delayed gastric emptying (DGE) | Common [1][2] | Especially in PPPD. Mechanisms: (1) Injury to nerve of Latarjet (anterior vagal branch supplying pylorus/antrum), (2) Disruption of duodenal pacemaker cells (interstitial cells of Cajal in the resected duodenum normally coordinate gastric emptying), (3) Reduced CCK (cholecystokinin — high concentration in duodenal mucosa, now resected) [2] | Prokinetics (metoclopramide, erythromycin), NJ feeding to maintain nutrition, usually self-resolving over weeks |
| Haemorrhage | Intra-operative vascular injury or post-op from anastomotic site / pseudoaneurysm | Re-operation or angiographic embolisation | |
| Pancreatitis | Manipulation of pancreatic remnant → inflammation | Supportive; usually mild | |
| Wound infection | Especially if preop biliary stenting → bile colonised with bacteria → contaminated operative field | The lecture slide notes: "Pre-op biliary stenting → bacterial contamination, inflammation, procedure-associated complications" [3] | |
| Pancreatic ascites | Pancreatic juice leaks into peritoneal cavity [14] | Drainage, somatostatin analogue | |
| Multi-organ failure | SIRS from pancreatic enzyme spillage → MOF (kidneys, lungs, bowels) | ICU support [1] |
The Dreaded PJ Leak Cascade
The PJ leak is the most dangerous complication of Whipple's because it triggers a cascade: leak of pancreatic enzymes → erosion of GDA pseudoaneurysm → catastrophic haemorrhage, AND/OR → portal vein thrombosis → mesenteric ischaemia, AND/OR → pancreatic fistula → dehydration + metabolic acidosis (loss of HCO₃⁻-rich pancreatic juice). This is why surgeons place abdominal drains around the pancreatic and biliary anastomosis to monitor for leaks early [1][2].
Somatostatin analogue (e.g. octreotide) does NOT reduce the risk of PJ leak — it only reduces the volume of output in established fistulae [2].
Only proven method to reduce PJ leakage: high-volume centre with high case load [14].
| Complication | Pathophysiology | Management |
|---|---|---|
| Exocrine insufficiency → Malabsorption and steatorrhoea [1] | Loss of pancreatic head parenchyma → reduced enzyme production (though some function remains from body/tail remnant) | Pancreatic enzyme replacement therapy (PERT) — e.g. Creon (pancrelipase) taken with meals |
| Endocrine insufficiency → DM | Loss of islets of Langerhans in resected head; new-onset DM in ~16% [2] | OHA / insulin |
| Gastric stasis | Especially in PPPD (preserved pylorus, but loss of duodenal coordination) [1] | Prokinetics, dietary modification (small frequent meals) |
| Dumping syndrome | More common in classic Whipple (loss of pylorus → rapid gastric emptying of hyperosmolar contents into jejunum → fluid shifts → vasomotor symptoms) | Dietary modification (small meals, avoid simple sugars), rarely octreotide |
| Marginal ulceration | Mucosal erosion at the gastrojejunostomy (GJ) site — exposure of jejunal mucosa to acid without buffering by duodenal bicarbonate | PPI therapy |
| Bile reflux gastritis | Bile reflux through GJ into gastric remnant → chemical gastritis (difficult to manage) [2] | Sucralfate, cholestyramine; surgical revision rarely needed |
| Tumour recurrence | Micrometastatic disease despite R0 resection; most recurrences are distant (liver, peritoneum) | Adjuvant chemotherapy reduces risk; surveillance with CT + CA 19-9 |
The lecture slide on tissue loss after resection explicitly notes [16]:
"Just adequate resection → No diabetes mellitus, No steatorrhoea" "Excessive resection → Diabetes mellitus, Steatorrhoea"
This highlights that the extent of pancreatic resection directly determines the severity of metabolic consequences. The surgical principle is to remove enough for oncological clearance while preserving as much functional parenchyma as possible.
| Complication | Detail |
|---|---|
| Pancreatic fistula / anastomotic leak | Higher anastomotic leak rate compared to Whipple's [2] — the cut surface of the pancreatic body/neck is large and the stump closure is under tension |
| Post-splenectomy complications | Overwhelming post-splenectomy infection (OPSI): lifelong risk of fulminant sepsis from encapsulated organisms (Streptococcus pneumoniae, Haemophilus influenzae type b, Neisseria meningitidis) → vaccination required [2] |
| Post-splenectomy thrombocytosis | Loss of splenic sequestration → reactive thrombocytosis → risk of thrombosis |
| Endocrine/exocrine insufficiency | Variable — depends on extent of resection |
| Complication | Mechanism |
|---|---|
| Stent occlusion | Sludge, tumour ingrowth (through mesh of metallic stent), tumour overgrowth (tumour grows over ends of stent) [13] → recurrent jaundice. Managed by sweeping or placing new stent [14] |
| Stent migration | Stent moves distally into duodenum or proximally into bile duct [13] |
| Cholangitis / Cholecystitis | Bacterial contamination of obstructed bile; stent dysfunction → re-obstruction → cholangitis [13] |
| Post-ERCP pancreatitis | Traumatic instrumentation at the ampulla → papillary oedema → pancreatic duct obstruction → acute pancreatitis |
| Perforation | Sphincterotomy too deep, or scope-related duodenal perforation |
| Bleeding | Post-sphincterotomy |
The lecture slide on preoperative biliary drainage complications notes [3]:
"Pre-op biliary drainage has increased risk of serious complications — Pancreatitis (7%), cholangitis (26%), blocked stent (15%), bleeding (2%), perforation (2%)" "Surgery-related complications were comparable" "Routine pre-op biliary drainage in patients undergoing surgery for CA pancreas increases rate of complications"
| Complication | Mechanism |
|---|---|
| Haemobilia / bleeding | Puncture of hepatic artery or portal vein before reaching bile duct (portal triad) [13] |
| Electrolyte / fluid loss | External PTBD → bile output is lost externally → loss of bile salts, fluid, electrolytes (Na⁺, K⁺, HCO₃⁻) |
| Catheter dislodgement | Accidental removal → bile peritonitis |
| Bacteraemia | Needle traverses skin and liver → risk of introducing infection |
| Regimen | Key Toxicities |
|---|---|
| FOLFIRINOX | Myelosuppression (neutropaenia), diarrhoea, peripheral neuropathy (oxaliplatin — cumulative, dose-limiting), mucositis, fatigue. Significant toxicity — reserved for fit patients |
| Gemcitabine | Myelosuppression (thrombocytopaenia predominant), flu-like symptoms, hepatotoxicity, interstitial pneumonitis (rare) |
| Capecitabine | Hand-foot syndrome (palmar-plantar erythrodysaesthesia — capecitabine is preferentially activated in tumour tissue via thymidine phosphorylase, but also activates in palms/soles), diarrhoea, mucositis |
The lecture slide explicitly lists the three major causes of mortality [15]:
Cause of mortality in MBO:
- Biliary sepsis
- Cancer cachexia
- Liver failure
And from the surgical oncology lecture [16]:
Causes of mortality related to cancer:
- Cancer invasion of organ of origin, adjacent organs or distant sites leading to loss of organ function
- Cancer cachexia
- Examples: Oesophageal cancer, Pancreatic cancer, Liver cancer
| Cause of Death | Mechanism |
|---|---|
| Biliary sepsis | Biliary stasis → ascending cholangitis → overwhelming sepsis → septic shock → multi-organ failure. This is why biliary decompression (stenting/PTBD) is a priority in palliation [15] |
| Cancer cachexia | Progressive wasting driven by tumour-derived cytokines (TNF-α/cachectin, IL-6, IL-1, proteolysis-inducing factor) → loss of skeletal muscle and adipose tissue → immune dysfunction → death from infection or cardiac failure [15][16] |
| Liver failure | (1) Hepatic metastases replace functional liver parenchyma → synthetic failure, or (2) prolonged biliary obstruction → secondary biliary cirrhosis → hepatic decompensation [15] |
| Scenario | Survival |
|---|---|
| After radical resection: 1-year | 66% [4] |
| After radical resection: 5-year | 27% [4] |
| Palliative bypass: 1-year | 10% [4] |
| Palliative bypass: 5-year | 0% [4] |
| Node-negative resection: 5-year | 25–30% [1] |
| Node-positive resection: 5-year | ~10% [1] |
| Unresectable locally advanced: median | 12 months [1] |
| Metastatic disease: median | 6 months [1] |
| Diagnosed at localised stage | Only 8% [1] |
| Diagnosed with distant metastases | 53% (majority) [1] |
High Yield Summary — Complications
-
Disease complications: Acute cholangitis (biliary sepsis), acute pancreatitis, GOO, obstructive jaundice with coagulopathy/malnutrition, Trousseau syndrome (migratory thrombophlebitis), new-onset DM.
-
Three leading causes of death in MBO: Biliary sepsis, cancer cachexia, liver failure.
-
PJ leak (~30%) is the most feared complication of Whipple's — triggers cascade of GDA pseudoaneurysm, haemorrhage, PV thrombosis, pancreatic fistula.
-
Pancreatic fistula definition: Drain output after postop D3 with amylase > 3× ULN. Risk factors: high BMI, soft pancreas, narrow duct.
-
DGE in PPPD: Injury to nerve of Latarjet + disrupted pacemaker cells + reduced CCK.
-
Only proven method to reduce PJ leak: High-volume centre with high case load.
-
Preop biliary drainage increases complications: Pancreatitis 7%, cholangitis 26%, blocked stent 15% — but practically necessary at QMH due to long surgical wait times.
-
Post-splenectomy: Lifelong risk of OPSI from encapsulated organisms → vaccination essential.
-
Just adequate resection → no DM, no steatorrhoea; excessive resection → DM + steatorrhoea — balance oncological clearance with functional preservation.
-
Radical resection: 1-year 66%, 5-year 27%. Palliative bypass: 1-year 10%, 5-year 0%.
Active Recall - Complications of Pancreatic Cancer
References
[1] Senior notes: felixlai.md (Pancreatic cancer — Complications, Prognosis, Clinical manifestation sections) [2] Senior notes: maxim.md (Pancreatic carcinoma — Whipple complications, Distal pancreatectomy, Adjuvant chemotherapy, Palliative treatment sections) [3] Lecture slides: Malignant biliary obstruction.pdf (p24 — preop biliary drainage complications; p26 — drainage complication rates; p29 — causes of mortality in MBO) [4] Lecture slides: WCS 056 - Painless jaundice and epigastric mass - by Prof R Poon.ppt (1).pdf (p76 — long-term survival data) [13] Senior notes: felixlai.md (MBO treatment — ERCP stent complications, PTBD complications) [14] Senior notes: maxim.md (Pancreatic fistula — ISGPF classification, management, methods to reduce PJ leakage; stent complications) [15] Lecture slides: Malignant biliary obstruction.pdf (p29 — causes of mortality in MBO) [16] Lecture slides: GC 202. Surgery may cure your cancer Surgical oncology.pdf (p15 — causes of mortality related to cancer; p44 — adequate vs excessive resection)
High Yield Summary
-
Pancreatic cancer ≈ PDAC (> 85%) — retroperitoneal, aggressive, dense desmoplastic stroma, poor prognosis (5-yr survival ~10%).
-
Painless progressive obstructive jaundice = hallmark of pancreatic head cancer; Courvoisier's sign = painless jaundice + palpable gallbladder.
-
Body/tail tumours present LATE with severe back pain (coeliac plexus invasion) and are rarely resectable.
-
Key risk factors: Smoking (~3× risk), chronic pancreatitis, DM (new-onset DM can be the first sign!), obesity, BRCA2 (most common hereditary gene), Lynch syndrome, Peutz-Jeghers, FAMMM, IPMN.
-
Genetic drivers: KRAS (> 90%), CDKN2A, TP53, SMAD4 — sequential accumulation through PanIN stages.
-
Resectability is determined by vascular involvement (SMA, celiac axis, CHA, SMV/PV), NOT tumour size.
-
Trousseau's syndrome (migratory superficial thrombophlebitis) = hypercoagulable paraneoplastic state; pancreatic panniculitis = subcutaneous fat necrosis from enzyme spillage.
-
New-onset DM in elderly patient + weight loss = suspect pancreatic cancer until proven otherwise.
-
Sites of metastasis: Liver (most common) > Peritoneum > Lung > Bone.
-
The "double duct sign" on imaging (dilated CBD + dilated pancreatic duct) is highly suggestive of pancreatic head malignancy.
High Yield Summary — Differential Diagnosis
-
Painless progressive obstructive jaundice in elderly = malignant biliary obstruction until proven otherwise. Top DDx: CA head of pancreas, distal cholangioCA, ampullary CA, CA duodenum.
-
Periampullary cancers (within 2 cm of ampulla): pancreatic head, distal CBD, ampullary, duodenal — all present with painless jaundice but have very different prognoses (ampullary best, PDAC worst).
-
Chronic pancreatitis is notoriously difficult to distinguish from PDAC — look for diffuse calcifications, chain-of-lakes duct, alcohol history; may need biopsy.
-
Autoimmune pancreatitis (IgG4-related) mimics PDAC but responds dramatically to steroids — check IgG4, look for sausage-shaped pancreas and multiorgan IgG4 disease.
-
PDAC = hypoattenuating on CT; PanNET = hyperenhancing on arterial phase — a key imaging distinction.
-
CA 19-9 is NOT diagnostic — use for prognosis and monitoring. Lewis-negative patients (5–10%) will never elevate CA 19-9.
-
Thomas' sign (silver stool) = pathognomonic of periampullary duodenal carcinoma (white stool from obstruction + melaena from tumour ulceration).
-
Metastases to pancreas: most commonly from RCC, also lung, breast, melanoma — usually well-circumscribed and hypervascular.
High Yield Summary — Diagnosis and Investigations
-
Pancreatic protocol CT (thin-sliced triphasic) is the GOLD STANDARD for diagnosis AND staging simultaneously.
-
Triphasic = arterial (arteries/resectability) + pancreatic/venous (tumour conspicuity) + portal venous (veins/resectability).
-
Classic CT finding: ill-defined hypoattenuating mass + double duct sign + vascular encasement.
-
Tissue diagnosis (biopsy) is NOT mandatory if the tumour is resectable — proceed to surgery. Biopsy is needed only for unresectable/metastatic disease, atypical features, neoadjuvant planning, or to exclude mimics.
-
EUS-guided FNAC is preferred over percutaneous biopsy (lower risk of peritoneal tumour seeding).
-
CA 19-9 is NOT diagnostic — it is prognostic and used for monitoring. Requires Lewis antigen expression.
-
Resectability criteria: No distant mets, SMA/celiac not encased > 180°, patent SMV-PV confluence (PV involvement is NOT an absolute contraindication if reconstructable).
-
Staging laparoscopy is indicated for body/tail tumours, large tumours > 4 cm, high CA 19-9, or equivocal CT findings.
-
Courvoisier's sign: Painless jaundice + palpable GB → malignant biliary obstruction. Exceptions: double gallstones, RPC.
-
Correct coagulopathy (IV vitamin K) before any invasive procedure in jaundiced patients.
High Yield Summary — Management
-
Only 15–20% of patients are surgical candidates — surgery is the only potentially curative treatment.
-
Assessment framework: General status (fit/unfit) + Tumour status (confined/spread) → determines surgery vs. palliation.
-
Resectability criteria: No distant mets, SMA/celiac not involved, patent SMV-PV confluence. PV involvement is NOT an absolute contraindication (venous resection for R0: median 13 months, 5-year 7%).
-
Whipple operation: For head/periampullary tumours. PPPD preferred (less dumping, less marginal ulcer, less bile reflux, better nutrition). Triple anastomosis: PJ → CJ → GJ/DJ.
-
Adjuvant chemotherapy is given to ALL resected patients — FOLFIRINOX (preferred) or Gemcitabine + capecitabine × 6 months. Start within 12 weeks.
-
Preop biliary drainage: NOT routine if early surgery possible; practically at QMH: drain ALL (long wait times). Plastic stent preop; SEMS if confirmed inoperable.
-
Palliative triad: Treat sepsis + Relieve obstruction (biliary stent/bypass, duodenal stent/GJ) + Pain control (opioids, celiac plexus block).
-
Unresectable at laparotomy → Double bypass (GJ for GOO + choledochoenterostomy for jaundice) + biopsy + celiac plexus block.
-
ERCP stenting is 1st line for biliary palliation (over PTBD). SEMS preferred for palliation (longer patency). PTBD if ERCP fails.
-
PJ leak is the most feared complication of Whipple (30% risk) → can cause GDA pseudoaneurysm, haemorrhage, pancreatic fistula.
-
Long-term survival after radical resection: 1-year 66%, 5-year 27%. Palliative bypass: 1-year 10%, 5-year 0%.
High Yield Summary — Complications
-
Disease complications: Acute cholangitis (biliary sepsis), acute pancreatitis, GOO, obstructive jaundice with coagulopathy/malnutrition, Trousseau syndrome (migratory thrombophlebitis), new-onset DM.
-
Three leading causes of death in MBO: Biliary sepsis, cancer cachexia, liver failure.
-
PJ leak (~30%) is the most feared complication of Whipple's — triggers cascade of GDA pseudoaneurysm, haemorrhage, PV thrombosis, pancreatic fistula.
-
Pancreatic fistula definition: Drain output after postop D3 with amylase > 3× ULN. Risk factors: high BMI, soft pancreas, narrow duct.
-
DGE in PPPD: Injury to nerve of Latarjet + disrupted pacemaker cells + reduced CCK.
-
Only proven method to reduce PJ leak: High-volume centre with high case load.
-
Preop biliary drainage increases complications: Pancreatitis 7%, cholangitis 26%, blocked stent 15% — but practically necessary at QMH due to long surgical wait times.
-
Post-splenectomy: Lifelong risk of OPSI from encapsulated organisms → vaccination essential.
-
Just adequate resection → no DM, no steatorrhoea; excessive resection → DM + steatorrhoea — balance oncological clearance with functional preservation.
-
Radical resection: 1-year 66%, 5-year 27%. Palliative bypass: 1-year 10%, 5-year 0%.

Sketchy memory palace for Pancreatic Cancer
| No. | Visual Cue | Meaning |
|---|---|---|
| 1 | Aggressive weeds growing through concrete; four valves (KRAS, CDKN2A, TP53, SMAD4) on a rusted pipe. | - Pancreatic cancer ≈ PDAC (> 85%) — retroperitoneal, aggressive, dense desmoplastic stroma, poor prognosis (5-yr survival ~10%). - Genetic drivers: KRAS (> 90%), CDKN2A, TP53, SMAD4 — sequential accumulation through PanIN stages. |
| 2 | Leaking yellow pipes (jaundice); a 'Y' junction where both arms are swollen (CBD and pancreatic duct); a silent, bloated green tank. | - Painless progressive obstructive jaundice = hallmark of pancreatic head cancer; Courvoisier's sign = painless jaundice + palpable gallbladder. - The "double duct sign" on imaging (dilated CBD + dilated pancreatic duct) is highly suggestive of pancreatic head malignancy. - Courvoisier's sign: Painless jaundice + palpable GB → malignant biliary obstruction. Exceptions: double gallstones, RPC. |
| 3 | A spine-like scaffold crushed by a mass; a periscope scanning the floor for tiny specks. | - Body/tail tumours present LATE with severe back pain (coeliac plexus invasion) and are rarely resectable. - Staging laparoscopy is indicated for body/tail tumours, large tumours > 4 cm, high CA 19-9, or equivocal CT findings. |
| 4 | Smoking chimney; spilled sugar (DM); a thin, elderly man (weight loss) looking surprised by a needle. | - Key risk factors: Smoking (~3× risk), chronic pancreatitis, DM (new-onset DM can be the first sign!), obesity, BRCA2 (most common hereditary gene), Lynch syndrome, Peutz-Jeghers, FAMMM, IPMN. - New-onset DM in elderly patient + weight loss = suspect pancreatic cancer until proven otherwise. |
| 5 | Cables (arteries) wrapped by a tumor; a 180-degree protractor; a blue pipe (vein) being patched. | - Resectability is determined by vascular involvement (SMA, celiac axis, CHA, SMV/PV), NOT tumour size. - Resectability criteria: No distant mets, SMA/celiac not encased > 180°, patent SMV-PV confluence (PV involvement is NOT an absolute contraindication if reconstructable). - Resectability criteria: No distant mets, SMA/celiac not involved, patent SMV-PV confluence. PV involvement is NOT an absolute contraindication (venous resection for R0: median 13 months, 5-year 7%). |
| 6 | A moving snake on a leg diagram; red lumps (fat necrosis); a flashing yellow alarm. | - Trousseau's syndrome (migratory superficial thrombophlebitis) = hypercoagulable paraneoplastic state; pancreatic panniculitis = subcutaneous fat necrosis from enzyme spillage. - Disease complications: Acute cholangitis (biliary sepsis), acute pancreatitis, GOO, obstructive jaundice with coagulopathy/malnutrition, Trousseau syndrome (migratory thrombophlebitis), new-onset DM. |
| 7 | Shipping trucks labeled with organ names; a hazard board with three death icons. | - Sites of metastasis: Liver (most common) > Peritoneum > Lung > Bone. - Three leading causes of death in MBO: Biliary sepsis, cancer cachexia, liver failure. |
| 8 | Four converging pipes; silver-colored sludge (silver stool). | - Painless progressive obstructive jaundice in elderly = malignant biliary obstruction until proven otherwise. Top DDx: CA head of pancreas, distal cholangioCA, ampullary CA, CA duodenum. - Periampullary cancers (within 2 cm of ampulla): pancreatic head, distal CBD, ampullary, duodenal — all present with painless jaundice but have very different prognoses (ampullary best, PDAC worst). - Thomas' sign (silver stool) = pathognomonic of periampullary duodenal carcinoma (white stool from obstruction + melaena from tumour ulceration). |
| 9 | Chalky stones on a model; a sausage-shaped organ; a glowing bright bulb (NET) vs a dark one (PDAC). | - Chronic pancreatitis is notoriously difficult to distinguish from PDAC — look for diffuse calcifications, chain-of-lakes duct, alcohol history; may need biopsy. - Autoimmune pancreatitis (IgG4-related) mimics PDAC but responds dramatically to steroids — check IgG4, look for sausage-shaped pancreas and multiorgan IgG4 disease. - PDAC = hypoattenuating on CT; PanNET = hyperenhancing on arterial phase — a key imaging distinction. |
| 10 | A monitoring gauge; a battery labeled 'Lewis'. | - CA 19-9 is NOT diagnostic — use for prognosis and monitoring. Lewis-negative patients (5–10%) will never elevate CA 19-9. - CA 19-9 is NOT diagnostic — it is prognostic and used for monitoring. Requires Lewis antigen expression. |
| 11 | A kidney-shaped drone; small lung and breast icons attacking a central unit. | - Metastases to pancreas: most commonly from RCC, also lung, breast, melanoma — usually well-circumscribed and hypervascular. |
| 12 | A scanner with three distinct color rings (red, purple, blue); a dark spot within a bright organ. | - Pancreatic protocol CT (thin-sliced triphasic) is the GOLD STANDARD for diagnosis AND staging simultaneously. - Triphasic = arterial (arteries/resectability) + pancreatic/venous (tumour conspicuity) + portal venous (veins/resectability). - Classic CT finding: ill-defined hypoattenuating mass + double duct sign + vascular encasement. |
| 13 | A 'Stop' sign over a biopsy needle; a camera-scope (EUS) sampling an internal wall. | - Tissue diagnosis (biopsy) is NOT mandatory if the tumour is resectable — proceed to surgery. Biopsy is needed only for unresectable/metastatic disease, atypical features, neoadjuvant planning, or to exclude mimics. - EUS-guided FNAC is preferred over percutaneous biopsy (lower risk of peritoneal tumour seeding). |
| 14 | Orange oil syringe; a plastic straw (stent) getting dirty/clogged. | - Correct coagulopathy (IV vitamin K) before any invasive procedure in jaundiced patients. - Preop biliary drainage: NOT routine if early surgery possible; practically at QMH: drain ALL (long wait times). Plastic stent preop; SEMS if confirmed inoperable. - Preop biliary drainage increases complications: Pancreatitis 7%, cholangitis 26%, blocked stent 15% — but practically necessary at QMH due to long surgical wait times. |
| 15 | A gate labeled 20% capacity; a guard checking a 'Fit vs Unfit' checklist. | - Only 15–20% of patients are surgical candidates — surgery is the only potentially curative treatment. - Assessment framework: General status (fit/unfit) + Tumour status (confined/spread) → determines surgery vs. palliation. |
| 16 | A complex 3-way pipe connection; a snipped wire; a scale with grease and sugar. | - Whipple operation: For head/periampullary tumours. PPPD preferred (less dumping, less marginal ulcer, less bile reflux, better nutrition). Triple anastomosis: PJ → CJ → GJ/DJ. - DGE in PPPD: Injury to nerve of Latarjet + disrupted pacemaker cells + reduced CCK. - Just adequate resection → no DM, no steatorrhoea; excessive resection → DM + steatorrhoea — balance oncological clearance with functional preservation. |
| 17 | Six month calendars; medicine bags with 'F' and 'G' symbols. | - Adjuvant chemotherapy is given to ALL resected patients — FOLFIRINOX (preferred) or Gemcitabine + capecitabine × 6 months. Start within 12 weeks. |
| 18 | Metal spring stent; an 'extra' bypass pipe loop. | - Palliative triad: Treat sepsis + Relieve obstruction (biliary stent/bypass, duodenal stent/GJ) + Pain control (opioids, celiac plexus block). - Unresectable at laparotomy → Double bypass (GJ for GOO + choledochoenterostomy for jaundice) + biopsy + celiac plexus block. - ERCP stenting is 1st line for biliary palliation (over PTBD). SEMS preferred for palliation (longer patency). PTBD if ERCP fails. |
| 19 | A dripping pipe joint; a fire on a wire; a large group of workers holding a joint. | - PJ leak is the most feared complication of Whipple (30% risk) → can cause GDA pseudoaneurysm, haemorrhage, pancreatic fistula. - PJ leak (~30%) is the most feared complication of Whipple's — triggers cascade of GDA pseudoaneurysm, haemorrhage, PV thrombosis, pancreatic fistula. - Pancreatic fistula definition: Drain output after postop D3 with amylase > 3× ULN. Risk factors: high BMI, soft pancreas, narrow duct. - Only proven method to reduce PJ leak: High-volume centre with high case load. |
| 20 | A missing shield; technician handing out 'V' icons to defend against armored bugs. | - Post-splenectomy: Lifelong risk of OPSI from encapsulated organisms → vaccination essential. |
| 21 | Exit paths with hourglasses; 27% sand vs 0% sand at 5 years. | - Long-term survival after radical resection: 1-year 66%, 5-year 27%. Palliative bypass: 1-year 10%, 5-year 0%. - Radical resection: 1-year 66%, 5-year 27%. Palliative bypass: 1-year 10%, 5-year 0%. |
Mirizzi Syndrome
Mirizzi syndrome is the extrinsic compression of the common hepatic duct by an impacted gallstone in the cystic duct or Hartmann's pouch, causing obstructive jaundice.
Primary Biliary Cirrhosis
Primary biliary cirrhosis is a chronic autoimmune liver disease characterized by progressive destruction of intrahepatic bile ducts, leading to cholestasis, fibrosis, and eventually cirrhosis.