Ca Stomach
Gastric carcinoma is a malignant neoplasm arising from the epithelial lining of the stomach, most commonly an adenocarcinoma, associated with risk factors such as H. pylori infection, dietary nitrosamines, and chronic atrophic gastritis.
CA Stomach (Gastric Cancer)
Gastric cancer (CA stomach) refers to malignant neoplasms arising from the stomach wall. The overwhelming majority (~90%) are adenocarcinomas originating from the glandular epithelium of the gastric mucosa [1][2]. Other histological types include gastric lymphoma (~5%), gastrointestinal stromal tumours (GISTs), neuroendocrine tumours (carcinoid), and rarely, metastatic deposits from other primaries [2].
The word "carcinoma" comes from Greek karkinos (crab) + -oma (tumour) — the ancient Greeks thought cancers resembled a crab with its legs extending outward, much like tumour projections.
II. Epidemiology
- Gastric cancer is the 5th most common cancer worldwide and the 4th leading cause of cancer death globally (2022 GLOBOCAN data).
- There is a declining overall incidence trend globally — attributed to declining H. pylori prevalence (improved sanitation, eradication therapy), better food preservation (refrigeration replacing smoking/salting/pickling), and reduced smoking rates [1][2].
- However, there is an increasing trend of proximal/cardia gastric cancer in Western countries — thought to be related to rising obesity and gastro-oesophageal reflux disease (GORD) [2].
- Incidence: decreasing trend (6th incidence, 4th mortality), but increased in Asia (Japan: diet-related) [2].
- Geographic variation is striking: highest incidence in East Asia (Japan, South Korea, China), parts of South America, and Eastern Europe; lowest in North America, Northern Europe, and Africa.
- Why East Asia? High prevalence of H. pylori, dietary factors (pickled vegetables, high-salt diet, smoked fish), and possibly genetic susceptibility.
- Japan and South Korea have national screening programmes (endoscopy-based) → detect more early gastric cancers → better survival statistics.
| Feature | Intestinal Type | Diffuse Type |
|---|---|---|
| Age | Elderly | Younger patients |
| Sex | Male predominance | Female predominance (relatively) |
| Location | Distal stomach (antrum/body) | Proximal stomach |
| Trend | Declining (linked to declining H. pylori) | Relatively stable or increasing |
- Cell type: adenocarcinoma (90%) > lymphoma (5%) > GIST, metastasis [2]
- Site: distal stomach (antrum/pylorus) > cardia (increasing trend) > OGJ [2]
High Yield Exam Point
In Hong Kong, gastric cancer is the 6th most common cancer overall but ranks 4th-5th for cancer mortality — reflecting its typically late presentation and poor prognosis when detected at advanced stages. Most present as adenocarcinoma (~90%).
III. Anatomy and Function of the Stomach
Understanding the anatomy is crucial because it dictates the surgical approach, lymph node drainage (and hence staging), and explains patterns of spread.
The stomach is a J-shaped muscular organ divided into:
- Cardia — the region immediately surrounding the gastro-oesophageal junction (GOJ); narrow zone where oesophageal squamous epithelium transitions to gastric columnar epithelium.
- Fundus — the dome-shaped portion superior and lateral to the cardia, sitting against the left hemidiaphragm; acts as a gas reservoir.
- Body (corpus) — the largest region; contains the majority of parietal cells (HCl production) and chief cells (pepsinogen production).
- Antrum — the distal "prepyloric" portion; rich in G cells that secrete gastrin, which stimulates parietal cells.
- Pylorus — the sphincteric muscle controlling gastric emptying into the duodenum.
The lesser curvature (medial, shorter) and greater curvature (lateral, longer) are the two borders. The angular incisure (incisura angularis) is the notch on the lesser curvature that marks the transition from body to antrum — a common site for Type I gastric ulcers and also a common biopsy site for surveillance.
All derived from the coeliac trunk (axis):
Lesser curvature:
- Left gastric artery — directly from the coeliac trunk (largest contributor to gastric blood supply)
- Right gastric artery — from the common hepatic artery (or proper hepatic artery)
Greater curvature:
- Short gastric arteries — from the splenic artery (supply the fundus)
- Left gastro-omental (gastroepiploic) artery — from the splenic artery
- Right gastro-omental (gastroepiploic) artery — from the gastroduodenal artery
This rich anastomotic network means the stomach has excellent blood supply and can survive ligation of most of its arterial branches, which is why partial gastrectomy is feasible. However, the rich vascularity also means gastric tumours can bleed significantly.
Venous drainage mirrors the arterial supply and ultimately drains into the portal venous system → this explains why the liver is the most common site of haematogenous metastasis from gastric cancer.
- Left and right gastric veins → portal vein
- Short gastric veins and left gastro-omental vein → splenic vein
- Right gastro-omental vein → superior mesenteric vein
Gastric lymph nodes are classified into 16 stations (Japanese Gastric Cancer Association classification), grouped into tiers:
- N1 (perigastric): Stations 1–6 — along the lesser and greater curvatures
- N2 (regional): Stations 7–11 — along the named arteries (left gastric, common hepatic, coeliac, splenic artery, splenic hilum)
- N3 (distant): Stations 12–16 — para-aortic, retropancreatic, mesenteric root
The extent of lymphadenectomy during gastrectomy (D1 vs D2 vs D3) is defined by how many of these tiers are removed. D2 lymphadenectomy (removing N1 + N2 stations) is the standard of care in East Asia (including HK) for curative-intent surgery.
- Sympathetic: Greater splanchnic nerve (T5–T9 sympathetic trunk) → coeliac ganglion → postganglionic fibres [4]
- Parasympathetic:
The vagus nerve is critical because it stimulates gastric acid secretion (via direct acetylcholine on parietal cells and indirectly via gastrin release). This is why vagotomy was historically used for peptic ulcer disease. In gastric cancer surgery, the vagal trunks are inevitably divided during gastrectomy, contributing to post-operative dumping syndrome and altered gastric motility.
- Mucosa (epithelium + lamina propria + muscularis mucosae)
- Submucosa — contains Meissner's plexus, rich lymphatic and blood vessels
- Muscularis propria — inner oblique, middle circular, outer longitudinal; contains Auerbach's (myenteric) plexus
- Serosa (visceral peritoneum) — covers most of the stomach except the bare area posteriorly
The T-staging of gastric cancer is based on depth of invasion through these layers, which is why understanding them is essential.
Why Anatomy Matters for Gastric Cancer
- The rich lymphatic network in the submucosa explains why gastric cancer metastasises early to lymph nodes — even "early" gastric cancer (confined to mucosa/submucosa) can have lymph node metastasis in 5–20% of cases.
- Venous drainage to the portal system explains liver metastases as the predominant haematogenous spread.
- Peritoneal seeding is common because the serosa is breached in advanced tumours (T4a), allowing cancer cells to drop into the peritoneal cavity.
IV. Etiology and Risk Factors
Think of the risk factors in a logical framework: anything that causes chronic inflammation → atrophy → metaplasia → dysplasia → carcinoma (the Correa cascade, especially for intestinal-type gastric cancer).
A. Infection
- H. pylori is classified as a WHO Group 1 carcinogen [1]
- A microaerophilic Gram-negative spiral-shaped bacterium with strong urease activity [4]
- Urease hydrolyses urea → ammonia + CO₂ → ammonia neutralises gastric acid, creating a protective alkaline microenvironment for the bacterium
- Its spiral shape + flagella + mucolytic enzymes allow it to burrow through the mucus gel layer to reach the gastric surface epithelium [4]
- Mechanism of carcinogenesis (the Correa cascade):
- H. pylori colonises the antral mucosa → triggers chronic active gastritis
- Persistent inflammation → progressive destruction of gastric glands → atrophic gastritis
- Loss of specialised gastric epithelium → replacement by intestinal metaplasia (goblet cells appear — the stomach tries to "become" intestine)
- Intestinal metaplasia → dysplasia → intestinal-type adenocarcinoma
- This cascade takes decades — typically 20–40 years from initial infection to cancer
- H. pylori also produces virulence factors:
- CagA (cytotoxin-associated gene A) — injected into host cells via a type IV secretion system; disrupts cell signalling, promotes proliferation and inflammation. CagA-positive strains carry higher cancer risk.
- VacA (vacuolating cytotoxin A) — causes epithelial cell vacuolation and apoptosis
- H. pylori → chronic atrophic gastritis → intestinal metaplasia → body/distal CA (intestinal type) [2]
- Note: H. pylori is also linked to gastric MALT lymphoma (mucosa-associated lymphoid tissue) — eradication of H. pylori can cure early-stage gastric MALT lymphoma.
H. pylori and Gastric Cancer vs Duodenal Ulcer
This is a classic exam concept: H. pylori-related antral-predominant gastritis → increased acid secretion → duodenal ulcer (does NOT predispose to cancer). H. pylori-related pangastritis/corpus-predominant gastritis → atrophy → decreased acid secretion → gastric ulcer/gastric cancer. The pattern of gastritis determines the clinical outcome [4].
- EBV-associated gastric carcinomas have distinct molecular features (global DNA hypermethylation, PIK3CA mutations, PD-L1/L2 amplification)
- Tends to occur in the proximal stomach (cardia/body)
- Generally has a better prognosis than EBV-negative gastric cancer — possibly due to stronger immune response
- Associated with lymphoepithelioma-like carcinoma histology
B. Gastrointestinal Diseases (Pre-malignant Conditions)
- MOST common precursor for gastric cancer, particularly the intestinal subtype [3]
- Chronic inflammation → loss of specialised glandular tissue (parietal and chief cells) → mucosal atrophy
- Leads to hypochlorhydria/achlorhydria → compensatory hypergastrinaemia → mucosal proliferation → increased cancer risk
- Autoimmune destruction of parietal cells → atrophic gastritis (body-predominant) → achlorhydria + loss of intrinsic factor → vitamin B12 deficiency → megaloblastic anaemia
- The underlying autoimmune atrophic gastritis is the cancer risk factor (3× increased risk)
- Chronic atrophic gastritis: associated with pernicious anaemia and Menetrier's disease [2]
- Intestinal metaplasia = gastric epithelium replaced by intestinal-type epithelium (goblet cells)
- Represents a key step in the Correa cascade
- Dysplasia (low-grade → high-grade) is the immediate precursor to invasive carcinoma
- Patients with high-grade dysplasia should undergo endoscopic resection or close surveillance
- Resect ALL adenomas; examine for synchronous CA; follow-up OGD [2]
- Unlike hyperplastic/fundic gland polyps (low malignant potential), adenomatous polyps have significant dysplasia and malignant potential (~30–40% harbour carcinoma if > 2 cm)
- Rare condition with giant gastric rugal folds (hypertrophy of foveolar mucous cells), excessive mucus production, protein-losing enteropathy, and hypochlorhydria
- Carries a 5–10% risk of gastric adenocarcinoma
- Chronic gastric ulcers (especially those associated with H. pylori pangastritis) have malignant potential
- This is why all gastric ulcers must be biopsied and followed up endoscopically to exclude malignancy — unlike duodenal ulcers, which virtually never undergo malignant transformation
- Previous partial gastrectomy (> 20 years) [1]
- Allows reflux of bile causing chronic gastritis → reactive/chemical gastropathy → atrophy → metaplasia → carcinoma [3]
- Typically occurs at the gastric remnant, especially at the gastrojejunal anastomosis (stump carcinoma)
- Risk increases ≥15–20 years post-surgery
- Billroth II reconstruction carries higher risk than Billroth I (because of greater bile reflux)
Harmful dietary factors: [1]
- N-nitroso compounds — powerful carcinogens; formed from dietary nitrates/nitrites by bacterial conversion (especially in hypochlorhydric stomachs where bacteria colonise)
- Preserved, smoked, salted food — high in nitrates, nitrosamines, and salt, which damages gastric mucosa directly and promotes H. pylori colonisation
- Pickled food [3] — common in East Asian diets, contributing to the high incidence in this region
Protective dietary factors: [1]
- Trace elements (e.g. selenium) — antioxidant (selenoproteins like glutathione peroxidase neutralise reactive oxygen species)
- Vitamin C — antioxidant that also inhibits the formation of N-nitroso compounds in the stomach
- Fresh fruits and vegetables — source of antioxidants and fibre
Industrial/occupational exposures: [1]
- Dusty, high temperature, rubber, coal mining, metal processing, chromium production — occupational carcinogen exposure
- Smoking (11% attributable risk) [1] — nitrosamines in tobacco smoke; also impairs gastric mucosal defence
- Alcohol — damages gastric mucosa directly; may have synergistic effect with H. pylori and smoking [3]
- Obesity — particularly associated with cardia/GOJ gastric cancer; mechanism: increased intra-abdominal pressure → GORD → Barrett's → proximal cancer; also chronic low-grade inflammation, hyperinsulinaemia [3]
- Low socioeconomic status [3] — correlates with higher H. pylori prevalence, poorer diet, and limited access to healthcare
F. Hereditary/Familial Factors
- Autosomal dominant; mutation in the CDH1 gene encoding E-cadherin [1][2]
- E-cadherin is a transmembrane glycoprotein crucial for cell-cell adhesion in epithelial tissues; loss of E-cadherin → loss of intercellular adhesion → cells invade individually (hence "diffuse" type, signet ring cell histology)
- Carries a lifetime risk of ~70% for gastric cancer
- Prophylactic total gastrectomy should be considered in confirmed CDH1 mutation carriers [3]
- Also associated with increased risk of lobular breast carcinoma in women (lobular, not ductal — because lobular breast cancer also features loss of E-cadherin)
- APC gene mutation → hundreds to thousands of colonic polyps; also gastric fundic gland polyps and adenomas → small but increased gastric cancer risk
- Mismatch repair gene mutations (MLH1, MSH2, MSH6, PMS2) → microsatellite instability
- Increased risk of gastric cancer (especially intestinal type) in addition to colorectal, endometrial, ovarian, and other cancers
- STK11/LKB1 gene mutation → hamartomatous polyps throughout GI tract + mucocutaneous pigmentation
- Increased risk of gastric and other GI cancers
- First-degree relatives of gastric cancer patients have 2–3× increased risk
- Even without a defined hereditary syndrome
- Primary immunodeficiency → chronic gastric infection/inflammation → atrophic gastritis → increased gastric cancer risk
- Also associated with gastric lymphoma
Risk Factor Summary — Mnemonic: 'GASTRIC PAIN'
G — Genetics (HDGC/E-cadherin, FAP, HNPCC, Peutz-Jeghers)
A — Atrophic gastritis / Adenomatous polyps
S — Smoking / Smoked, Salted food
T — (prior gas)Trectomy
R — Reflux (bile reflux post-surgery)
I — Infection (H. pylori, EBV)
C — CVID
P — Pernicious anaemia / Pickled food
A — Alcohol
I — Industrial exposure
N — Nitrosamines / N-nitroso compounds
V. Pathophysiology
This is the classic multi-step model proposed by Pelayo Correa:
Why does this sequence happen?
- Chronic mucosal injury → repeated cycles of cell death and regeneration → increased cell turnover → greater chance of DNA replication errors
- Achlorhydria (from parietal cell loss) → bacterial overgrowth → increased nitrosamine production in the stomach
- Hypergastrinaemia (compensatory, from loss of acid feedback) → trophic effect on mucosal cells → promotes proliferation
- Accumulation of genetic mutations (TP53, APC, KRAS, microsatellite instability) drives progression through each stage
- Does not follow the Correa cascade
- Driven by loss of E-cadherin (CDH1 mutation — germline in HDGC, or somatic/epigenetic silencing in sporadic cases)
- E-cadherin loss → disrupted cell-cell adhesion → individual tumour cells infiltrate diffusely through the gastric wall (no glandular formation)
- Characterised by signet ring cells — tumour cells with large intracytoplasmic mucin vacuoles that push the nucleus to the periphery, giving a "signet ring" appearance
- More likely to invade transmurally and seed the peritoneum early
Modern molecular classification divides gastric cancer into 4 subtypes:
| Subtype | Key Features | Clinical Relevance |
|---|---|---|
| EBV-positive (~9%) | PIK3CA mutations, PD-L1/L2 amplification, DNA hypermethylation | May respond to immunotherapy (checkpoint inhibitors) |
| MSI-high (~22%) | Mismatch repair deficiency, hypermutation | Better prognosis; may respond to immunotherapy; associated with Lynch syndrome |
| Genomically stable (GS) (~20%) | CDH1 mutations, RHOA mutations; mostly diffuse type | Poor prognosis; limited targeted therapy options |
| Chromosomal instability (CIN) (~50%) | TP53 mutations, RTK-RAS amplification; mostly intestinal type | HER2 amplification → trastuzumab target |
Gastric cancer spreads by four routes:
- Direct invasion — into adjacent organs (pancreas, transverse colon, spleen, liver, diaphragm)
- Lymphatic spread — to perigastric, coeliac, para-aortic lymph nodes; most common route
- Haematogenous spread — via portal vein to liver (most common distant metastatic site); also lung, bone, brain (uncommon) [3]
- Transcoelomic (peritoneal) spread — once the tumour penetrates the serosa (T4a), cancer cells shed into the peritoneal cavity → peritoneal carcinomatosis, malignant ascites, Krukenberg tumour (bilateral ovarian metastases — signet ring cells implanting on the ovaries)
Spread to: liver / peritoneum / lymph nodes (common); brain / lung / ovary / bone (uncommon) [3]
Eponymous Metastatic Signs of Gastric Cancer
These are named after the doctors who described them and represent specific sites of metastasis:
- Virchow's node (Troisier's sign) — left supraclavicular lymph node (lymphatic drainage via thoracic duct)
- Sister Mary Joseph's nodule — periumbilical nodule (peritoneal spread along the falciform ligament)
- Krukenberg tumour — bilateral ovarian metastases (transcoelomic spread; characteristically signet ring cells)
- Blumer's shelf — palpable mass on digital rectal examination in the rectovesical/rectouterine pouch (pouch of Douglas) — dependent part of peritoneal cavity where cancer cells pool
- Irish's node — left axillary lymph node metastasis
VI. Classification
This is the most clinically useful histological classification:
| Feature | Intestinal Type | Diffuse Type |
|---|---|---|
| Differentiation | Well-differentiated, gland-forming | Undifferentiated, non-cohesive (signet ring cells) |
| Risk factors | All the above environmental/infectious factors | HDGC (E-cadherin mutation) |
| HER2 status | HER2 +ve in ~15% | HER2 -ve |
| Spread pattern | Haematogenous spread | Transmural (linitis plastica) and lymphatic spread |
| Demographics | Elderly male, distal stomach | Young female, proximal stomach |
| Prognosis | Better prognosis | Poorer prognosis |
| Precursor lesion | Correa cascade (atrophy → metaplasia → dysplasia) | No defined precursor cascade |
| Association | Declining incidence | Stable/increasing incidence |
Classifies the gross appearance of advanced gastric cancer:
| Borrmann Type | Description |
|---|---|
| Type I | Polypoid/fungating — well-circumscribed, protruding mass |
| Type II | Ulcerating with raised edges — resembles a volcano crater |
| Type III | Ulcerating with infiltration — ulcer with poorly defined margins infiltrating the wall |
| Type IV | Diffusely infiltrating — linitis plastica ("leather bottle stomach") |
- Aggressive form of poorly-differentiated diffuse-type gastric cancer
- Broad region of gastric wall is extensively infiltrated by malignancy resulting in a rigid, thickened stomach termed linitis plastica ("leather bottle" stomach)
- "Linitis" = from Latin linum (linen/flax); "plastica" = moulded — the stomach becomes stiff like starched linen
- Difficult to diagnose with upper endoscopy; barium swallow is superior [3]
- Poor prognosis: [3]
- Late presentation with advanced stage at diagnosis
- Potential for early spread with 1/3 of patients having metastatic disease to peritoneum (malignant ascites) at diagnosis
- Presence of microscopic disease at surgical margins due to its diffuse nature
Linitis Plastica — Why Endoscopy Misses It
A common pitfall: the mucosa may appear relatively normal in linitis plastica because the tumour grows in the submucosa/muscularis propria. Standard superficial mucosal biopsies grab only the superficial layer and can be falsely negative. If you suspect linitis plastica (e.g., stomach does not distend well on insufflation, thickened folds, reduced peristalsis), use deep "strip and bite" biopsies or consider endoscopic ultrasound (EUS) to assess wall thickness. Barium swallow may show the classic non-distensible "leather bottle" appearance [3].
| Feature | Early Gastric Cancer (EGC) | Advanced Gastric Cancer (AGC) |
|---|---|---|
| Definition | Confined to mucosa or submucosa (T1), regardless of lymph node status | Invades into or beyond muscularis propria (≥T2) |
| Lymph node metastasis | Present in 5–20% (higher if submucosal invasion) | Present in ~50–80% |
| 5-year survival | > 90% (with curative resection) | 20–30% overall |
| Treatment | May be amenable to endoscopic resection (EMR/ESD) if select criteria met | Surgical resection ± chemotherapy |
Note: "Early" here is a pathological definition referring to depth of invasion — NOT size or symptoms. An early gastric cancer can be quite large but still confined to the mucosa/submucosa.
T (Primary Tumour):
| Stage | Depth of Invasion |
|---|---|
| Tis | Carcinoma in situ (intraepithelial, no invasion of lamina propria) |
| T1a | Lamina propria or muscularis mucosae |
| T1b | Submucosa |
| T2 | Muscularis propria |
| T3 | Subserosa (penetrates subserosal connective tissue without involving serosa) |
| T4a | Perforates serosa (visceral peritoneum) |
| T4b | Invades adjacent structures (spleen, transverse colon, liver, diaphragm, pancreas, abdominal wall, adrenal gland, kidney, small intestine, retroperitoneum) |
N (Regional Lymph Nodes):
| Stage | Number of Regional LNs |
|---|---|
| N0 | 0 |
| N1 | 1–2 |
| N2 | 3–6 |
| N3a | 7–15 |
| N3b | ≥16 |
A minimum of 16 lymph nodes must be examined for adequate staging (this is why D2 lymphadenectomy is preferred).
M (Distant Metastasis):
- M0: No distant metastasis
- M1: Distant metastasis (including positive peritoneal cytology)
VII. Clinical Features
Gastric cancer is notoriously asymptomatic in early stages — this is the main reason why most cases outside Japan/Korea are diagnosed at an advanced stage. Symptoms develop as the tumour grows, obstructs, ulcerates, or metastasises.
A. Symptoms
- Mechanism: Tumour infiltrating the gastric wall → activation of visceral afferent pain fibres (transmitted via the greater splanchnic nerve T5–T9) → poorly localised epigastric pain
- May mimic peptic ulcer disease or dyspepsia — hence the importance of endoscopy in any patient with "red flag" dyspepsia
- Pain may radiate to the back if the tumour invades the pancreas (retroperitoneal, somatic pain)
- Mechanism: Multifactorial:
- Anorexia — cancer-related cytokines (TNF-α, IL-6) suppress appetite via hypothalamic signalling
- Cancer cachexia — tumour-mediated catabolism (increased basal metabolic rate, proteolysis, lipolysis)
- Mechanical obstruction — tumour at the cardia/pylorus reduces food intake
- Malabsorption — especially post-surgical or with extensive mucosal involvement
- Significant unintentional weight loss is a red flag ("alarm symptom") that mandates investigation [5]
- Mechanism:
- Gastric outlet obstruction (GOO): Tumour at the antrum/pylorus → physical obstruction of gastric emptying → distension of stomach → stimulates vomiting centre via vagal afferents
- GOO vomiting is characteristically projectile, non-bilious (obstruction is proximal to the ampulla of Vater), and contains undigested food eaten hours or even days earlier
- May develop a succussion splash (audible splash on shaking the abdomen) due to retained gastric contents
- Visible peristalsis may be observed in thin patients (stomach contracting against an obstructing tumour) [5]
- Can also occur due to:
- Direct stimulation of the chemoreceptor trigger zone by tumour-derived substances
- Raised intracranial pressure (if brain metastasis — rare)
- Mechanism: Tumour at the cardia or GOJ → progressive mechanical obstruction of the oesophagogastric junction
- Characteristically progressive — initially solids only, then liquids
- Consider in the differential of dysphagia alongside oesophageal carcinoma [6]
- Mechanism: Tumour bulk within the stomach reduces functional gastric capacity; in linitis plastica, the entire stomach wall is stiff and non-distensible → cannot accommodate a normal meal volume
- Due to gastric stasis (poor emptying), direct vagal stimulation by the tumour, or peritoneal irritation
- Mechanism: Tumour ulceration → erosion into gastric mucosal blood vessels → bleeding into the GI lumen
- Haematemesis = vomiting blood (if brisk, fresh red blood; if slow, "coffee-ground" vomitus — haemoglobin converted to haematin by gastric acid)
- Melaena = black, tarry, foul-smelling stools (blood digested by GI enzymes and bacteria during transit)
- Chronic occult blood loss is more common than massive haemorrhage → insidious iron deficiency anaemia
- Mechanism: Chronic occult GI blood loss → iron deficiency anaemia (microcytic, hypochromic)
- May be the presenting feature in some patients, especially those with early or submucosal tumours that ulcerate
- Mechanism: Malignant ascites (peritoneal carcinomatosis → increased peritoneal capillary permeability + lymphatic obstruction) or massive hepatomegaly from liver metastases
- Malaise, lethargy, fever — due to cancer-related systemic inflammatory response (elevated CRP, cytokines)
B. Signs
- Epigastric mass — palpable in advanced cases; may be firm, irregular, non-tender [7]
- A palpable epigastric mass in the setting of weight loss and anaemia is highly suspicious for gastric cancer [5]
- Succussion splash — audible splash >3 hours post-prandial suggests gastric outlet obstruction (retained gastric contents)
- Visible gastric peristalsis — in thin patients with GOO, waves of peristalsis may be visible on the anterior abdominal wall [5]
These are named eponymous signs that indicate advanced/metastatic disease — knowing them is high-yield:
| Sign | Description | Mechanism |
|---|---|---|
| Virchow's node (Troisier's sign) | Hard, non-tender, left supraclavicular lymph node | Lymphatic spread via thoracic duct, which drains into the left subclavian vein; the left supraclavicular fossa is the "sentinel" for intra-abdominal malignancy |
| Sister Mary Joseph's nodule | Periumbilical nodule | Peritoneal tumour deposits spread along the falciform ligament / umbilical folds to the umbilicus |
| Krukenberg tumour | Bilateral ovarian masses (on bimanual pelvic exam or imaging) | Transcoelomic spread; signet ring cells have tropism for ovarian stroma |
| Blumer's shelf | Hard, shelf-like mass palpable on digital rectal examination | Tumour deposits in the rectovesical/rectouterine pouch (pouch of Douglas — most dependent part of peritoneal cavity) |
| Irish's node | Left axillary lymphadenopathy | Lymphatic spread |
- Hepatomegaly — hard, nodular, irregular liver edge = liver metastases
- Ascites — shifting dullness, fluid thrill = peritoneal carcinomatosis or liver metastases with portal hypertension
- Jaundice — periampullary/porta hepatis lymph node metastases compressing the common bile duct, or extensive liver metastases [7]
- Pallor — anaemia from chronic blood loss or cancer cachexia
- Cachexia — temporal wasting, sunken cheeks, loss of subcutaneous fat and muscle bulk — cancer-related metabolic wasting
| Syndrome | Manifestation | Mechanism |
|---|---|---|
| Acanthosis nigricans | Velvety, dark hyperpigmentation in axillae, neck, groin | Tumour-secreted growth factors (e.g. TGF-α, IGF) stimulate keratinocyte and fibroblast proliferation |
| Trousseau's sign | Migratory superficial thrombophlebitis | Mucin-secreting adenocarcinoma releases procoagulant substances → hypercoagulable state |
| Leser-Trélat sign | Sudden eruption of multiple seborrhoeic keratoses | Tumour-secreted growth factors (TGF-α) |
| Dermatomyositis | Proximal muscle weakness + heliotrope rash | Autoimmune paraneoplastic process |
Alarm Symptoms ('Red Flags') for Gastric Cancer in Dyspeptic Patients
Any patient with dyspepsia plus the following features should undergo urgent upper endoscopy (OGD):
- Age > 55 with new-onset dyspepsia
- Unintentional weight loss
- Progressive dysphagia
- Persistent vomiting
- GI bleeding (haematemesis/melaena)
- Palpable abdominal mass
- Iron deficiency anaemia
- Family history of upper GI cancer
Do NOT just treat with a PPI and "see how it goes" in these patients — this delays diagnosis!
| Pathophysiological Process | Clinical Feature |
|---|---|
| Tumour infiltration of gastric wall | Epigastric pain |
| Cardia/GOJ obstruction | Dysphagia |
| Antrum/pylorus obstruction (GOO) | Projectile non-bilious vomiting, succussion splash |
| Reduced gastric capacity (linitis plastica) | Early satiety |
| Tumour ulceration → mucosal vessel erosion | Haematemesis, melaena, iron deficiency anaemia |
| Cancer cachexia (TNF-α, IL-6) | Weight loss, anorexia |
| Peritoneal carcinomatosis | Ascites, Blumer's shelf, Krukenberg tumour, Sister MJ nodule |
| Lymphatic dissemination | Virchow's node, Irish's node |
| Haematogenous spread (portal) | Hepatomegaly, jaundice |
| Procoagulant secretion | Trousseau's migratory thrombophlebitis |
| Growth factor secretion | Acanthosis nigricans, Leser-Trélat sign |
High Yield Summary
Definition: Gastric cancer = predominantly adenocarcinoma (90%) of the stomach; classified by Lauren into intestinal (well-differentiated, elderly male, distal, better prognosis) and diffuse (undifferentiated, young female, proximal, worse prognosis).
Epidemiology (HK): 6th most common cancer, 4th–5th mortality; M:F = 1.5:1; declining incidence overall but cardia cancers increasing.
Key Risk Factors: H. pylori (WHO Group 1 carcinogen — Correa cascade), EBV (10%), atrophic gastritis (MOST common precursor), pernicious anaemia, Menetrier's disease, adenomatous polyps, prior gastrectomy (>20 yrs, bile reflux), dietary nitrosamines/smoked/pickled/salted food, smoking, HDGC (E-cadherin/CDH1 mutation → prophylactic gastrectomy), FAP, HNPCC, CVID.
Protective: Fresh fruits/vegetables, vitamin C, selenium.
Pathophysiology: Intestinal type follows the Correa cascade (normal → chronic gastritis → atrophy → intestinal metaplasia → dysplasia → carcinoma). Diffuse type driven by E-cadherin loss → signet ring cells, linitis plastica.
Spread: Lymphatic (most common), haematogenous (liver > lung), transcoelomic (peritoneum, Krukenberg tumour), direct invasion.
Clinical Features: Often asymptomatic early. Alarm symptoms: weight loss, dysphagia, vomiting, GI bleed, epigastric mass, anaemia. Key metastatic signs: Virchow's node, Sister Mary Joseph's nodule, Krukenberg tumour, Blumer's shelf.
Linitis plastica: Diffuse type, leather bottle stomach, hard to biopsy endoscopically (submucosal infiltration), poor prognosis, 1/3 have peritoneal mets at diagnosis.
Active Recall - CA Stomach (Definition to Clinical Features)
[1] Lecture slides: GC 212. Weight loss and vomiting gastric cancer; abdominal imaging.pdf (p10–12) [2] Senior notes: maxim.md (Gastric cancer section) [3] Senior notes: felixlai.md (CA Stomach, pp. 400–402) [4] Senior notes: felixlai.md (PUD/Stomach anatomy, pp. 386–388) [5] Lecture slides: GC 212. Weight loss and vomiting gastric cancer; abdominal imaging.pdf (title/clinical content) [6] Lecture slides: GC 189. I can't swallow oesophageal cancer.pdf [7] Lecture slides: WCS 056 - Painless jaundice and epigastric mass - by Prof R Poon.ppt (1).pdf
Differential Diagnosis of CA Stomach
The differential diagnosis of gastric cancer is fundamentally about pattern recognition — you are presented with a patient who has some combination of dyspepsia, weight loss, vomiting, GI bleeding, anaemia, an epigastric mass, or dysphagia. The key question is: what else could produce this clinical picture?
The approach depends on the dominant presenting feature. Let me walk you through this systematically.
Gastric cancer is notoriously difficult to diagnose early [5]. The symptoms — epigastric discomfort, bloating, early satiety, nausea — are identical to benign conditions like functional dyspepsia and peptic ulcer disease, which are vastly more common. This is why alarm features (red flags) exist: they are the clinical "tripwires" that should shift your thinking from benign to potentially malignant.
The clinical presentation of benign gastric ulcer, early gastric cancer, and advanced gastric cancer can overlap significantly [5]. An OGD with biopsy is the only way to reliably distinguish them.
A. Differential Diagnosis by Presenting Syndrome
This is the most common presentation of gastric cancer, but dyspepsia affects ~25% of the population and is overwhelmingly benign [8].
| Differential | Key Distinguishing Features | Why It Mimics CA Stomach |
|---|---|---|
| Functional dyspepsia (60% of dyspepsia) | No structural cause on OGD; Rome IV criteria; symptoms > 6 months; no alarm features | Shares epigastric pain, early satiety, bloating, nausea [8] |
| Peptic ulcer disease (gastric/duodenal) | Epigastric pain related to meals; GU: precipitated by food; DU: relieved by food, worse at night; H. pylori or NSAID history | Epigastric pain, GI bleeding, weight loss (from food avoidance); gastric ulcers must ALWAYS be biopsied to exclude malignancy [4][8] |
| Gastro-oesophageal reflux disease (GERD) | Retrosternal burning (heartburn), regurgitation, worse on lying flat/bending; responds to PPI | Can cause epigastric discomfort; proximal gastric/cardia cancer may cause reflux-like symptoms [8] |
| Chronic pancreatitis | Epigastric pain radiating to the back; steatorrhoea; history of alcohol/recurrent pancreatitis; pancreatic calcifications on imaging | Epigastric pain, weight loss, anorexia [8] |
| Pancreatic cancer | Painless progressive obstructive jaundice (head); severe epigastric pain radiating to the back (body/tail); new-onset DM; weight loss [9][10] | Weight loss, epigastric mass, anorexia; may present identically to CA stomach — requires imaging (CT) to differentiate |
| Gastritis / Duodenitis | Often drug-induced (NSAIDs, alcohol) or stress-related; typically self-limited; diagnosed on OGD | Epigastric pain, nausea, GI bleeding [8] |
| Biliary colic / Cholecystitis | RUQ/epigastric pain, colicky, post-prandial (fatty food), Murphy's sign; USS shows gallstones | Epigastric pain post-prandially; referred epigastric pain |
The Golden Rule for Gastric Ulcers
Every gastric ulcer found on OGD must be biopsied (multiple biopsies from the ulcer margin) AND followed up with a repeat OGD at 6–8 weeks to confirm healing. Unlike duodenal ulcers (which virtually never become malignant), gastric ulcers can harbour carcinoma, and a malignant ulcer can look macroscopically identical to a benign one [4][8].
Gastric cancer accounts for a small proportion of UGIB — peptic ulcer disease is by far the most common cause [8][11].
| Differential | Key Distinguishing Features |
|---|---|
| Peptic ulcer disease (most common cause of UGIB) | 4 major risk factors: H. pylori, NSAIDs, stress, excess acid; episodic bleeding; visible vessel/clot on OGD [8][11] |
| Oesophagogastric varices | History of liver cirrhosis / portal hypertension; massive haematemesis; stigmata of chronic liver disease [8] |
| Erosive oesophagitis / oesophageal ulcers | GERD history; medications (bisphosphonates, tetracyclines); infections (HSV, Candida) [8] |
| Gastritis / Duodenitis | Drug/alcohol/stress-related; typically self-limited; mucosal inflammation on OGD [8] |
| Portal hypertensive gastropathy | Cirrhotic patients; friable mucosa with "snakeskin" or "mosaic" pattern on OGD; more commonly occult bleeding [8] |
| Mallory-Weiss syndrome | Longitudinal mucosal tear at GOJ preceded by forceful retching/vomiting; typically self-limited [8] |
| Dieulafoy's lesion | Dilated aberrant submucosal artery eroding overlying epithelium without primary ulcer; usually proximal stomach along lesser curvature; intermittent arterial spurting [8] |
| Gastric antral vascular ectasia (GAVE) | "Watermelon stomach" — longitudinal reddish stripes radiating from pylorus; associated with cirrhosis, autoimmune disease [8] |
| Angiodysplasia | Dilated tortuous submucosal vessels; more common in elderly; associated with aortic stenosis (Heyde's syndrome) [8] |
| Other upper GI malignancy | Oesophageal cancer, duodenal cancer — uncommon causes of UGIB; constitutional symptoms more prominent [8] |
GOO is malignant until proven otherwise — 80% malignant, 20% benign [2][12].
| Differential | Key Features |
|---|---|
| Malignant (80%) | |
| Gastric cancer (most common cause of GOO) | Progressive, non-bilious vomiting of undigested food; weight loss; epigastric mass [2][12] |
| Gastric lymphoma | Similar presentation; may have B symptoms (fever, night sweats, weight loss) [2] |
| Extrinsic compression: CA head of pancreas, CA ampulla of Vater, transverse colon/hepatic flexure, locally advanced cholangiocarcinoma/CA gallbladder | Jaundice may be prominent; distinct imaging findings [12] |
| Benign (20%) | |
| PUD-related pyloric stenosis (2nd most common cause) | Long history of PUD; chronic fibrotic scarring at pylorus [12] |
| Gastric volvulus | Acute presentation; associated with paraesophageal (rolling) hiatal hernia; Borchardt's triad (epigastric pain, retching, inability to pass NG tube) [12] |
| Foreign body / Bezoar / Bouveret syndrome | Bouveret = gallstone impaction in duodenum (gallstone ileus variant) [12] |
| SMA syndrome | Thin young patients; duodenal compression between SMA and aorta [12] |
| Chronic pancreatitis | Inflammatory exudate compressing duodenum [12] |
| Crohn's disease, Gastric TB | Chronic inflammatory stricturing [12] |
When gastric cancer involves the cardia or GOJ, the presentation overlaps with oesophageal cancer [6].
| Differential | Key Distinguishing Features |
|---|---|
| Oesophageal carcinoma (SCC or adenocarcinoma) | Progressive dysphagia (solids → liquids); weight loss; SCC: mid-oesophagus, smoking/alcohol; adenocarcinoma: distal oesophagus/GOJ, Barrett's [6] |
| Achalasia | Dysphagia to both solids AND liquids from onset; regurgitation of undigested food; bird's beak on barium swallow; diagnosed by high-resolution manometry [13] |
| Pseudoachalasia | Mimics achalasia but caused by CA cardia invading the oesophageal neural plexus (paraneoplastic); differentiate by OGD + EUS — look for mass [13] |
| Oesophageal stricture (peptic) | History of longstanding GERD; smooth, tapered narrowing on barium/OGD |
| Extrinsic compression | Mediastinal lymphadenopathy, lung cancer, aortic aneurysm |
Pseudoachalasia — A Dangerous Mimic
Pseudoachalasia can be caused by malignancy at the GOJ/cardia invading the oesophageal neural plexus directly, or as a paraneoplastic syndrome [13]. Clues that suggest pseudoachalasia over true achalasia: age > 60, rapid onset of dysphagia ( < 6 months), significant weight loss, and difficulty passing the endoscope through the GOJ. Always perform OGD (± EUS) before diagnosing achalasia to exclude malignancy [13].
An epigastric mass narrows the differential considerably, but you still need to consider non-gastric causes [5][14].
| Differential | Key Features |
|---|---|
| Gastric adenocarcinoma | Firm, irregular epigastric mass; associated with weight loss, anaemia, GI bleed [5] |
| Gastric lymphoma | May be indistinguishable from adenocarcinoma on examination; typically younger; B symptoms; OGD + biopsy with IHC needed [2] |
| GIST (gastrointestinal stromal tumour) | 50% in stomach (most common proximal stomach); usually incidental finding; mass with smooth margins and normal overlying mucosa on OGD; arises from muscularis propria (interstitial cells of Cajal); diagnosed by EUS + FNA; IHC: CD117 (c-KIT) positive [14] |
| Pancreatic cancer / pseudocyst | Mass may be palpable in the epigastrium; associated with jaundice (head), back pain (body/tail), weight loss [9][10] |
| Hepatomegaly (metastatic liver) | Hard, nodular, irregular liver edge extending into epigastrium; commonest site of metastasis from GI tract via portal venous circulation [15] |
| Omental cake | Hard, irregular mass across upper abdomen; peritoneal carcinomatosis (often from gastric, ovarian, or colonic primary) [2] |
| Gastric volvulus | Acute or chronic; tympanitic epigastric distension |
This is a useful conceptual framework (especially relevant for EUS assessment) [14]:
| Layer | Differential |
|---|---|
| Mucosa | Adenocarcinoma, gastrinoma, carcinoid, adenoma |
| Submucosa | Neuroendocrine tumour (NET), lymphoma, lipoma, ectopic pancreas |
| Muscularis propria | GIST (most common), leiomyoma, leiomyosarcoma, schwannoma, desmoid tumour |
| Serosa/Adventitia | Extrinsic compression (pancreas, spleen, lymph nodes) |
The following algorithm represents how to approach a patient whose presentation raises suspicion for gastric cancer:
| Feature | CA Stomach | Peptic Ulcer Disease | Gastric Lymphoma | GIST |
|---|---|---|---|---|
| Age | Older (intestinal) or younger (diffuse) | Any age | 50–60s | 50–70s |
| Symptoms | Progressive, alarm features | Episodic, meal-related | B symptoms possible | Often incidental |
| OGD appearance | Irregular ulcer, mass, rigid wall | Clean-based or cratered ulcer, smooth margins | Thickened folds, mass, ulceration | Smooth submucosal bulge, intact mucosa |
| Biopsy | Adenocarcinoma | Inflammatory, no dysplasia | Lymphoid tissue; IHC for B-cell markers | Spindle cells; CD117+, c-KIT mutation [14] |
| Key investigation | OGD + biopsy | OGD + biopsy + CLO test | OGD + deep biopsy + IHC | EUS + FNA [14] |
Gastric Lymphoma vs Adenocarcinoma
Gastric lymphoma (usually MALT lymphoma or diffuse large B-cell lymphoma) can present identically to adenocarcinoma on OGD. Key differences: lymphoma may show thickened gastric folds rather than a discrete mass, and it often responds to H. pylori eradication (early-stage MALT). Deep biopsies with immunohistochemistry (CD20, CD79a for B-cell markers) are essential — superficial biopsies may miss the lymphoid infiltrate in the lamina propria/submucosa [2][14].
When a patient presents with "epigastric pain + weight loss," think beyond the stomach:
- Pancreatic cancer — weight loss, back pain, jaundice; CT shows pancreatic mass [9][10]
- Hepatocellular carcinoma — risk factors (chronic hepatitis B/C, cirrhosis); AFP elevated; USS/CT shows liver mass
- Metastatic carcinoma to the liver — commoner than primary liver cancer; commonest site from GI tract via portal venous circulation (colorectal, stomach, pancreas); hepatomegaly ± symptoms from primary [15]
- Chronic mesenteric ischaemia — "intestinal angina"; post-prandial pain → food fear → weight loss; elderly with vascular risk factors
- Coeliac disease — weight loss, diarrhoea, iron deficiency anaemia; anti-tTG antibodies
- Metabolic causes of dyspepsia — hypercalcaemia, hyperkalaemia [8]
High Yield Summary — Differential Diagnosis of CA Stomach
- The DDx depends on the presenting syndrome: dyspepsia (functional dyspepsia, PUD, GERD, chronic pancreatitis, pancreatic cancer), UGIB (PUD most common, varices, Mallory-Weiss, Dieulafoy), GOO (malignant 80% — CA stomach most common; benign 20% — PUD stricture), dysphagia (oesophageal cancer, achalasia/pseudoachalasia), epigastric mass (lymphoma, GIST, pancreatic mass, omental cake).
- Gastric ulcers must always be biopsied — they can harbour carcinoma.
- GOO is malignant until proven otherwise.
- Pseudoachalasia (malignancy mimicking achalasia) must be excluded by OGD ± EUS before diagnosing achalasia.
- For submucosal gastric masses: think GIST (CD117+, muscularis propria), lymphoma (submucosa), NET — require EUS ± FNA.
- Non-GI causes: pancreatic cancer, liver metastases, HCC, mesenteric ischaemia.
Active Recall - CA Stomach Differential Diagnosis
References
[2] Senior notes: maxim.md (Gastric cancer section) [4] Senior notes: felixlai.md (PUD section, pp. 386–389) [5] Lecture slides: GC 212. Weight loss and vomiting gastric cancer; abdominal imaging.pdf (p23–26) [6] Lecture slides: GC 189. I can't swallow oesophageal cancer.pdf [8] Senior notes: felixlai.md (Dyspepsia section, pp. 327–329; UGIB DDx, pp. 334–335) [9] Senior notes: felixlai.md (Pancreatic cancer section, p. 591) [10] Senior notes: maxim.md (Pancreatic carcinoma section) [11] Senior notes: maxim.md (UGIB section) [12] Senior notes: maxim.md (Gastric outlet obstruction section) [13] Senior notes: maxim.md (Achalasia / pseudoachalasia section); Senior notes: felixlai.md (Achalasia section, p. 360) [14] Senior notes: maxim.md (GIST section) [15] Lecture slides: WCS 064 - A large liver - by Prof R Poon [20191108].doc.pdf (p6)
Diagnosis of CA Stomach — Diagnostic Criteria, Algorithm and Investigations
There is no single "diagnostic criterion" for gastric cancer in the way that rheumatological or metabolic diseases have point-based criteria. Instead, the diagnosis rests on a histopathological confirmation from tissue obtained at endoscopy. The clinical workflow is:
- Suspicion → clinical features + alarm symptoms
- Tissue diagnosis → OGD + biopsy (the gold standard)
- Staging → determine extent of disease to guide management
- Pre-operative assessment → fitness for surgery
It is notoriously difficult to make an early diagnosis — the clinical presentations of benign gastric ulcer, early gastric cancer, and advanced gastric cancer overlap substantially [5]. This means a low threshold for endoscopy in at-risk patients is essential.
The following algorithm integrates clinical suspicion, tissue diagnosis, and staging into a single workflow:
III. Investigation Modalities — Detailed Breakdown
CBP, LFT, RFT are the mandatory baseline investigations [5][16].
| Test | What You're Looking For | Rationale / Interpretation |
|---|---|---|
| CBC with differentials | Hypochromic microcytic anaemia (low MCV, low MCH, low ferritin, low iron, high TIBC) | Iron deficiency anaemia from chronic occult GI blood loss — tumour ulceration erodes mucosal vessels. This may be the only clue in early/submucosal tumours [16][3] |
| LFT | Raised ALP, GGT (cholestatic pattern); hypoalbuminaemia | ALP/GGT rise suggests liver metastases or biliary obstruction from porta hepatis lymphadenopathy. Albumin is a marker of nutritional status — often low in advanced cancer with cachexia [3][16] |
| RFT | Raised creatinine, proteinuria | Evaluate for membranous nephropathy (nephrotic syndrome) — a recognised paraneoplastic syndrome of gastric adenocarcinoma [3][5]. Also baseline for chemotherapy dosing and contrast administration |
| Clotting profile | Prolonged PT/INR | Liver synthetic function assessment (if metastatic liver disease); also baseline for surgery. Disseminated intravascular coagulation can occur in advanced malignancy (Trousseau's) |
| Electrolyte profile | Hypochloraemic hypokalaemic metabolic alkalosis | Occurs secondary to GOO with repeated vomiting of HCl → loss of H⁺ and Cl⁻ → metabolic alkalosis; renal compensation leads to K⁺ wasting (secondary hyperaldosteronism from volume depletion) [3][12] |
| Iron studies | Low ferritin, low serum iron, high TIBC | Confirms iron deficiency as the cause of anaemia |
| Group and save / Crossmatch | Blood type; antibody screen | Pre-operative preparation; anticipate blood loss |
Tumour Markers Are NOT Diagnostic
This is a common exam pitfall. CEA and CA125 are NOT useful in diagnosis [3]. They lack sufficient sensitivity and specificity for screening or primary diagnosis. They are useful for:
| Marker | Notes |
|---|---|
| CEA (carcinoembryonic antigen) | Epithelial marker; elevated in many GI malignancies, smoking, IBD, pregnancy — very non-specific. Elevated in ~30-40% of gastric cancers |
| CA19-9 | Also elevated in pancreatic, biliary, and colorectal cancers; and in benign biliary obstruction, pancreatitis |
| CA125 | More commonly associated with ovarian cancer; can be elevated in peritoneal carcinomatosis from gastric cancer |
| CA72-4 | Most specific tumour marker for gastric cancer (though still not widely used for screening); may be used in combination |
Upper endoscopy and biopsies [5][16] — this is the single most important investigation. It serves two purposes:
- Obtain tissue diagnosis (histological confirmation of malignancy)
- Evaluate extent of primary tumour endoscopically [2]
Why OGD is the gold standard:
- Direct visualisation of the gastric mucosa with magnification
- Ability to take multiple targeted biopsies from suspicious lesions
- Assessment of tumour location, size, morphology (Borrmann type), and involvement of the GOJ
- Therapeutic potential (e.g., endoscopic mucosal resection for early gastric cancer)
Endoscopic findings in gastric cancer:
| Finding | Type of Cancer | Description |
|---|---|---|
| Ulcerated mass protruding into lumen | Advanced (Borrmann I/II) | Irregular, raised edges; friable tissue; necrotic base — contrasts with benign ulcers that have smooth, regular, rounded edges and a flat base [4] |
| Irregular/thickened ulcer margins | Advanced (Borrmann III) | Ulcer with poorly defined, heaped-up margins; folds surrounding the crater are nodular, clubbed, fused [4] |
| Rigid stomach that could not be distended with air; mucosa may appear "normal" | Linitis plastica (Borrmann IV) [5] | The stomach fails to inflate properly on insufflation. The mucosa looks deceptively normal because the tumour infiltrates the submucosa/muscularis propria. This is the classic trap — standard superficial biopsies will miss it |
| Subtle mucosal irregularity, discolouration, depression | Early gastric cancer | Small, flat or depressed lesions; may require chromoendoscopy or narrow-band imaging (NBI) to detect |
Biopsy technique:
- At least 6–8 biopsies should be taken from the margin of any gastric ulcer (multiple quadrants) to maximise diagnostic sensitivity — a single biopsy has only ~70% sensitivity, but 7 biopsies reaches > 98%
- For suspected linitis plastica: use deep "strip and bite" biopsy technique — standard mucosal biopsies are insufficient because the tumour is submucosal [3]
- Biopsies of normal-appearing mucosa in the antrum and body should also be taken to assess for H. pylori, atrophic gastritis, and intestinal metaplasia (the Sydney protocol: 5 biopsies — 2 antrum, 1 incisura, 2 body)
Advanced endoscopic techniques:
- Narrow-band imaging (NBI): Uses specific wavelengths of light to enhance surface mucosal and vascular patterns — helps distinguish neoplastic from non-neoplastic lesions without dye application
- Chromoendoscopy: Application of dyes (e.g., indigo carmine, methylene blue) to enhance mucosal detail — useful for detecting early gastric cancer and defining margins for endoscopic resection
- Magnification endoscopy: Allows detailed assessment of mucosal pit patterns and microvascular architecture
Histological analysis from biopsy should determine:
- Histological type (adenocarcinoma vs lymphoma vs GIST vs other)
- Lauren classification (intestinal vs diffuse)
- Grade of differentiation (well / moderately / poorly differentiated)
- HER2 status (by IHC ± FISH) — essential for treatment decisions (trastuzumab eligibility; HER2 +ve in ~15% of intestinal type) [2]
- Microsatellite instability (MSI) / mismatch repair (MMR) status — for immunotherapy eligibility
- PD-L1 combined positive score (CPS) — for checkpoint inhibitor eligibility
- EBV status (EBER ISH)
Key Molecular Markers to Request on Biopsy (2025 Standard of Care)
For all newly diagnosed gastric/GOJ adenocarcinomas, request:
- HER2 (IHC ± FISH) — if positive → trastuzumab
- MSI/MMR status — if MSI-H/dMMR → checkpoint inhibitors (pembrolizumab/nivolumab)
- PD-L1 CPS — if CPS ≥ 5 → nivolumab in first-line setting
- Claudin 18.2 (CLDN18.2) — if positive → zolbetuximab (new targeted therapy)
These molecular tests fundamentally change the treatment algorithm and should never be forgotten.
Alternative to OGD — Barium Swallow/Meal:
- Limited diagnostic value except for linitis plastica [2]
- Shows a non-distensible "leather bottle" stomach with loss of mucosal folds — the classic radiographic appearance
- Cannot take biopsies — so even if barium is suggestive, OGD is still needed
- Largely superseded by OGD in modern practice but still useful when OGD cannot adequately assess gastric distensibility
D. Staging Investigations
Once histological diagnosis is confirmed, staging determines the extent of disease and guides treatment decisions. The most important prognostic factor is depth of tumour invasion [2].
The staging workup is best understood by what each modality assesses:
| Investigation | Best For | Limitations |
|---|---|---|
| CT abdomen + pelvis ± thorax with contrast | M staging (mandatory); locoregional extension | Not accurate for T & N staging [2] |
| Endoscopic ultrasound (EUS) | T staging and N staging (most accurate) | NOT mandatory for CA stomach — upfront surgery advocated in most cases [2]; operator-dependent; more invasive |
| Staging laparoscopy + peritoneal lavage | Peritoneal and liver metastasis (more accurate than CT) | Invasive (requires GA); does not assess distant nodal/haematogenous metastases |
| PET-CT | Distant metastasis; treatment response monitoring | Not too sensitive for CA stomach (especially mucinous/signet ring tumours — low FDG avidity) [2] |
| CXR | Lung metastases; pleural effusion; pre-op | Low sensitivity for small pulmonary metastases |
Mandatory for M staging but not accurate for T & N [2].
- Why CT? It provides a rapid, non-invasive survey of the entire torso to detect:
- Liver metastases — hypodense lesions in the liver parenchyma (the most common distant metastatic site)
- Peritoneal nodules / ascites — though CT has limited sensitivity for small peritoneal deposits (hence the need for staging laparoscopy)
- Lymphadenopathy — enlarged lymph nodes along coeliac axis, para-aortic region, mediastinum (Virchow's)
- Direct invasion into adjacent organs (pancreas, transverse colon, spleen)
- Hydronephrosis — from ureteric obstruction by pelvic or retroperitoneal tumour deposits
- Lung metastases, pleural effusion — especially if proximal (cardia) tumour
- Thorax CT is included if proximal tumour (e.g., cardia/GOJ) — to assess mediastinal involvement [2]
- CT is also the basis for assessing resectability — e.g., major vessel encasement, distant metastatic disease
CT appearances of gastric cancer:
- Focal or diffuse gastric wall thickening (> 5mm when distended)
- Enhancing intraluminal mass
- Loss of fat planes with adjacent organs (suggesting T4b invasion)
- In linitis plastica: diffuse circumferential wall thickening with loss of rugal folds
- More sensitive in T staging (e.g., differentiating T4a vs T4b) and N staging (e.g., perigastric LN) [2]
- More operator-dependent and more invasive compared to CT [2]
- NOT mandatory for CA stomach — unlike CA oesophagus where EUS is standard, in CA stomach upfront surgery is advocated in most situations [2]
When IS EUS useful?
- Suspected early gastric cancer (T1a vs T1b) — this distinction determines eligibility for endoscopic resection (T1a only, if other criteria met) vs surgery
- Assessing depth of invasion when CT is equivocal (e.g., T3 vs T4a — determines whether neoadjuvant chemotherapy is warranted)
- EUS-guided FNA of suspicious perigastric lymph nodes for cytological confirmation
- Submucosal masses — to determine the layer of origin and guide biopsy approach [14]
EUS wall layers of the stomach (from lumen outward):
- Hyperechoic — superficial mucosa
- Hypoechoic — deep mucosa (muscularis mucosae)
- Hyperechoic — submucosa
- Hypoechoic — muscularis propria
- Hyperechoic — serosa
The tumour appears as a hypoechoic lesion disrupting these normal layer patterns. The key question is: which layer does the tumour reach?
More accurate for peritoneal and liver metastasis compared to CT [2]. This is considered routine in many centres (including HK) before committing to curative-intent surgery.
Why is it needed?
- CT has a sensitivity of only ~30–50% for detecting peritoneal carcinomatosis — small (< 5mm) peritoneal deposits are easily missed
- Direct visualisation of the peritoneal surfaces, liver surface, and omentum ± biopsy of suspicious lesions for frozen section [2]
- Peritoneal washing for cytology — even in the absence of visible peritoneal deposits, positive peritoneal cytology indicates microscopic peritoneal metastasis (classified as M1) and renders the disease incurable by surgery alone [2]
- Avoids unnecessary laparotomy in patients with occult peritoneal disease — a significant benefit given the morbidity of a non-therapeutic gastrectomy
Indications for staging laparoscopy (typically):
- Any patient being considered for curative-intent gastrectomy with ≥T3 or node-positive disease on imaging
- Particularly important for diffuse-type / linitis plastica (high rate of occult peritoneal metastasis — 1/3 at diagnosis) [3]
- Uses ¹⁸F-fluorodeoxyglucose (FDG) — a glucose analogue taken up preferentially by metabolically active (including malignant) cells
- Not too sensitive for CA stomach [2] — Why?
- Mucinous and signet ring cell adenocarcinomas (diffuse type) have relatively low metabolic activity and therefore low FDG uptake → false negatives
- Normal physiological gastric uptake can obscure the primary tumour
- When PET-CT IS useful:
- Detecting distant metastases not seen on CT (e.g., unsuspected bone, distant nodal metastases)
- Monitoring treatment response after neoadjuvant chemotherapy (metabolic response assessment)
- Detecting recurrence post-surgery
- Alternative to CT for M staging but not routinely first-line for gastric cancer [2]
Chest x-ray is a basic but essential investigation:
- Detect lung metastases (cannonball lesions)
- Pleural effusion (malignant or reactive)
- Lymphangitis carcinomatosis (reticular interstitial pattern — bilateral, often lower zones)
- Pre-operative baseline assessment of cardiopulmonary status
Diagnostic imaging is valuable for: [5]
- Staging — chest x-ray, CAT scan, PET scan
- Diagnosis of:
- Intestinal obstruction
- Malignant biliary obstruction
- Malignant ureteric obstruction
- Monitoring response to treatment
From the lecture slides, the clinical staging workup consists of:
- History and physical examination
- Liver function test
- Chest x-ray
- Ultrasonography or CAT scan abdomen
- PET/CT scan
- Endoscopic ultrasound
- Laparoscopy
| Purpose | Investigation | Key Findings |
|---|---|---|
| Tissue Diagnosis | OGD + multiple biopsies | Histological type, Lauren classification, differentiation grade, HER2, MSI, PD-L1, CLDN18.2 |
| Alternative for linitis plastica | Barium swallow | Non-distensible leather bottle stomach; loss of rugal folds |
| T and N staging | EUS (if needed) | Depth of wall invasion (T1a vs T1b vs T2+); perigastric LN involvement |
| M staging | CT TAP with contrast (mandatory) | Liver mets, peritoneal nodules, LN, direct invasion, hydronephrosis |
| Peritoneal staging | Staging laparoscopy + peritoneal lavage | Peritoneal deposits, liver surface mets, positive peritoneal cytology |
| Distant metastasis | PET-CT (adjunct) | Unsuspected distant mets; treatment response |
| Baseline / Pre-op | CBC, LFT, RFT, clotting, electrolytes, CXR | Anaemia, liver function, renal function, nutritional status, cardiopulmonary fitness |
| Follow-up / Monitoring | CEA, CA19-9, CA125 | Trend over time; rising level suggests recurrence |
This is a high-yield comparison for exams [4]:
| Feature | Benign Ulcer | Malignant Ulcer |
|---|---|---|
| Edges | Smooth, regular, rounded | Irregular, thickened, heaped-up |
| Base | Flat, smooth, often filled with exudate | Necrotic, nodular |
| Surrounding folds | Radiate symmetrically to the ulcer edge | Nodular, clubbed, fused — folds do not reach the edge cleanly |
| Mucosa | Smooth, pliable surrounding mucosa | Friable, easily bleeds on contact |
| Shape | Round or oval | Irregular |
Every Gastric Ulcer Gets Biopsied
Even if an ulcer looks "benign" endoscopically, always biopsy (≥6 biopsies from the margin). A proportion of malignant ulcers can appear deceptively benign. Furthermore, every gastric ulcer must have a repeat OGD at 6–8 weeks post-treatment to confirm healing. A non-healing gastric ulcer despite appropriate therapy is malignant until proven otherwise [4].
VI. Special Diagnostic Considerations
As covered earlier, linitis plastica presents a unique diagnostic problem:
- Mucosa may appear "normal" on endoscopy [5]
- Rigid, could not be distended with air [5]
- Standard mucosal biopsies → false negatives because the tumour infiltrates the submucosa and muscularis propria [3]
Diagnostic approach:
- Deep strip-and-bite biopsies (grab deeper tissue including submucosa)
- EUS — shows diffuse hypoechoic wall thickening involving the 3rd and 4th layers (submucosa and muscularis propria)
- Barium swallow — may be superior to OGD for this specific entity; shows the classic non-distensible stomach with narrowed lumen and loss of rugal folds [2]
- CT — shows diffuse circumferential gastric wall thickening
- HER2 (Human Epidermal growth factor Receptor 2) is a transmembrane tyrosine kinase receptor; when amplified/overexpressed, it drives uncontrolled cell proliferation
- HER2 +ve in ~15% of gastric cancers (predominantly intestinal type) [2]
- Testing method: IHC first → if 2+ (equivocal) → confirm with FISH (fluorescence in situ hybridisation)
- A positive HER2 result qualifies the patient for trastuzumab (Herceptin) — a monoclonal antibody targeting HER2 — in combination with chemotherapy
High Yield Summary — Diagnosis of CA Stomach
- Gold standard: OGD + multiple biopsies (≥6 from ulcer margins). Request histology + HER2 + MSI/MMR + PD-L1 + CLDN18.2 on all new diagnoses.
- Tumour markers (CEA, CA19-9, CA125) are NOT diagnostic — used for follow-up and monitoring recurrence only.
- Staging workup: CT TAP with contrast (mandatory for M staging, not accurate for T/N); EUS (best for T/N but NOT mandatory — upfront surgery advocated); Staging laparoscopy + peritoneal lavage (routine — more accurate than CT for peritoneal disease); PET-CT (adjunct, not sensitive for mucinous/signet ring tumours).
- Linitis plastica is the diagnostic trap: normal-appearing mucosa on OGD, non-distensible stomach, requires deep biopsies + EUS + barium swallow.
- Benign vs malignant ulcer: benign = smooth, regular, rounded edges, flat base; malignant = irregular, thickened edges, nodular/clubbed/fused surrounding folds. ALL gastric ulcers must be biopsied and followed up.
- Clinical staging checklist (from lecture): H&P, LFT, CXR, USG/CT abdomen, PET/CT, EUS, laparoscopy.
Active Recall - CA Stomach Diagnosis and Investigations
References
[2] Senior notes: maxim.md (Gastric cancer — Investigations and Staging section) [3] Senior notes: felixlai.md (CA Stomach — Diagnosis section, pp. 411–412) [4] Senior notes: felixlai.md (PUD — OGD findings and Forrest classification, p. 390) [5] Lecture slides: GC 212. Weight loss and vomiting gastric cancer; abdominal imaging.pdf (p23, p27, p31, p57) [12] Senior notes: maxim.md (Gastric outlet obstruction section) [14] Senior notes: maxim.md (GIST section — EUS and FNA) [16] Senior notes: felixlai.md (CA Stomach — Biochemical tests, pp. 411–412)
Management of CA Stomach
The management of gastric cancer depends on two fundamental assessments:
- Patient fitness ("Can this patient tolerate surgery?") — age, comorbidities, nutritional status, performance status
- Clinical stage ("Is the disease curable?") — determined by staging investigations (CT, staging laparoscopy, ± EUS, ± PET-CT)
Treatment depends on "fitness" and clinical stage [5].
Currently, resection remains the only hope for cure for resectable disease [5].
In HK, ~70% patients present with diseases Stage III [5] — this is a sobering statistic. The majority of patients present with locally advanced disease, which explains the high mortality of gastric cancer in Hong Kong despite it being only the 6th most common cancer.
III. Endoscopic Treatment — Potentially Curative for Early Gastric Cancer
Early cancer: T1, mucosal. Rare in Hong Kong. Japan — screening endoscopy [5].
In Japan and Korea, where gastric cancer screening programmes exist, a significant proportion of cancers are detected at the early (T1) stage. In Hong Kong, this is rare because there is no population screening programme, so most cancers are advanced at presentation [5].
Indications: early gastric CA confined to mucosa (T1a) — diagnosed by endoscopic white light picture (not EUS!) [2]
The rationale is based on lymph node metastasis risk:
- T1a (mucosal): LN metastasis risk ~3–5% (acceptable for endoscopic resection if other criteria met)
- T1b (submucosal): LN metastasis risk ~15–25% → requires surgical resection with lymphadenectomy [3][17]
Expanded criteria for endoscopic resection (Japanese Gastric Cancer Treatment Guidelines 2021):
| Criterion | Absolute Indication | Expanded Indication |
|---|---|---|
| Depth | Mucosal (T1a) | Mucosal (T1a) |
| Size | ≤ 2 cm | > 2 cm (if differentiated, no ulceration) |
| Histology | Differentiated (intestinal) | Differentiated; undifferentiated ≤ 2 cm without ulceration |
| Ulceration | No ulceration | ≤ 3 cm with ulceration (differentiated only) |
| Lymphovascular invasion | Absent | Absent |
| LN status | N0 on staging | N0 on staging |
B. Techniques
- Technique: Injection of saline ± adrenaline beneath the mucosa to "lift" the lesion from the muscularis propria → snare resection of the raised lesion
- Only resects lesions < 2 cm — larger lesions require piecemeal resection, which:
- Increases risk of complications
- Makes histological margin assessment impossible (fragmented specimen)
- Higher recurrence rate [2]
- Technique: Uses a specialised electrocautery knife to dissect the lesion directly from the submucosa, achieving en bloc resection regardless of size
- Can resect lesions > 2 cm [2]
- Permits a deeper resection margin with submucosal involvement — the specimen includes the submucosa, allowing accurate histological assessment of deep margins [3]
- Higher en bloc resection rate and lower recurrence rate compared to EMR [3]
- More complications: bleeding, perforation, stricture [2]
EMR vs ESD — When to Use Which
Think of it this way: EMR is simpler and safer but limited to small lesions (< 2 cm) because it cannot guarantee en bloc resection for larger lesions. ESD is more technically demanding and has higher complication rates but can achieve en bloc resection of large lesions with accurate margin assessment. The trend in expert centres is towards ESD for most early gastric cancers [2][3].
After EMR/ESD, the resected specimen is meticulously assessed histologically:
- Lateral margins — clear or involved?
- Deep margin — clear or involved?
- Depth of invasion — T1a (mucosal) vs T1b (submucosal)?
- Lymphovascular invasion (LVI) — present or absent?
- Differentiation — well/moderately vs poorly differentiated?
Histology determines margin (lateral and deep) — consider curative if clear; salvage gastrectomy if T1b+ [2]
If curative criteria are met → endoscopic surveillance annually [2] If non-curative (T1b, positive margins, LVI, undifferentiated) → salvage gastrectomy with lymphadenectomy
IV. Surgical Treatment — The Mainstay of Curative Therapy
Surgery is the primary treatment in the absence of distant metastasis. Many patients with positive LN are cured by adequate surgery [3].
-
Complete resection with negative microscopic margins (R0 resection) [3]
- Gross negative margins of ≥ 5 cm are required from the macroscopic tumour edge [3]
- Why 5 cm? Because gastric cancer (especially diffuse type) can have microscopic intramural extension beyond the visible tumour margin. A wide margin minimises the risk of positive microscopic margins.
- Intraoperative frozen section of the proximal resection margin is performed to confirm negative margins in real time
-
Adequate lymphadenectomy — at minimum, D2 (see below)
-
En bloc resection of adjacent involved organs in T4b tumours — e.g., distal pancreas, transverse colon, spleen [3]
Tumours are considered unresectable (i.e., curative-intent surgery is not appropriate) if:
- Distant metastasis (e.g., multiple liver metastases, peritoneal nodules, pelvic deposits, Virchow's nodes) [17]
- Extensive nodal involvement (D3) [17]
- Invasion of major vascular structures: aorta, hepatic artery, coeliac axis, proximal splenic artery [3][17]
- Positive peritoneal cytology on staging laparoscopy (= M1) [2]
Resectability Assessment — Think of Two Axes
Borrowed from the pancreatic cancer framework but equally applicable here [18]:
Patient axis: Is the patient fit enough? (Performance status, nutrition, comorbidities) Tumour axis: Is the tumour technically removable? (No distant metastases, no major vessel encasement)
Both must be favourable for curative-intent surgery to be offered.
The extent of gastric resection depends on the location of the tumour:
Gastric resection with D2 lymph node dissection [5]:
| Tumour Location | Type of Gastrectomy | Reconstruction | Rationale |
|---|---|---|---|
| Distal stomach (antrum/pylorus) | Distal (subtotal) gastrectomy | Billroth I (gastroduodenostomy) or Billroth II (gastrojejunostomy) or Roux-en-Y gastrojejunostomy | Removes tumour with ≥5 cm proximal margin; preserves proximal stomach (better nutritional outcomes, lower morbidity than total gastrectomy) |
| Proximal stomach (cardia/body/fundus) or GOJ | Total gastrectomy | Roux-en-Y oesophagojejunostomy [5] | Cannot achieve adequate proximal margin with subtotal gastrectomy; the entire stomach must be removed |
| Middle body (equivocal) | Total gastrectomy (usually) | Roux-en-Y oesophagojejunostomy | Depends on whether 5 cm proximal AND distal margins can be achieved with subtotal gastrectomy |
| Linitis plastica | Total gastrectomy (always) | Roux-en-Y oesophagojejunostomy | Diffuse involvement of the entire stomach wall; microscopic disease at margins is common [3] |
Common reconstruction patterns after gastrectomy:
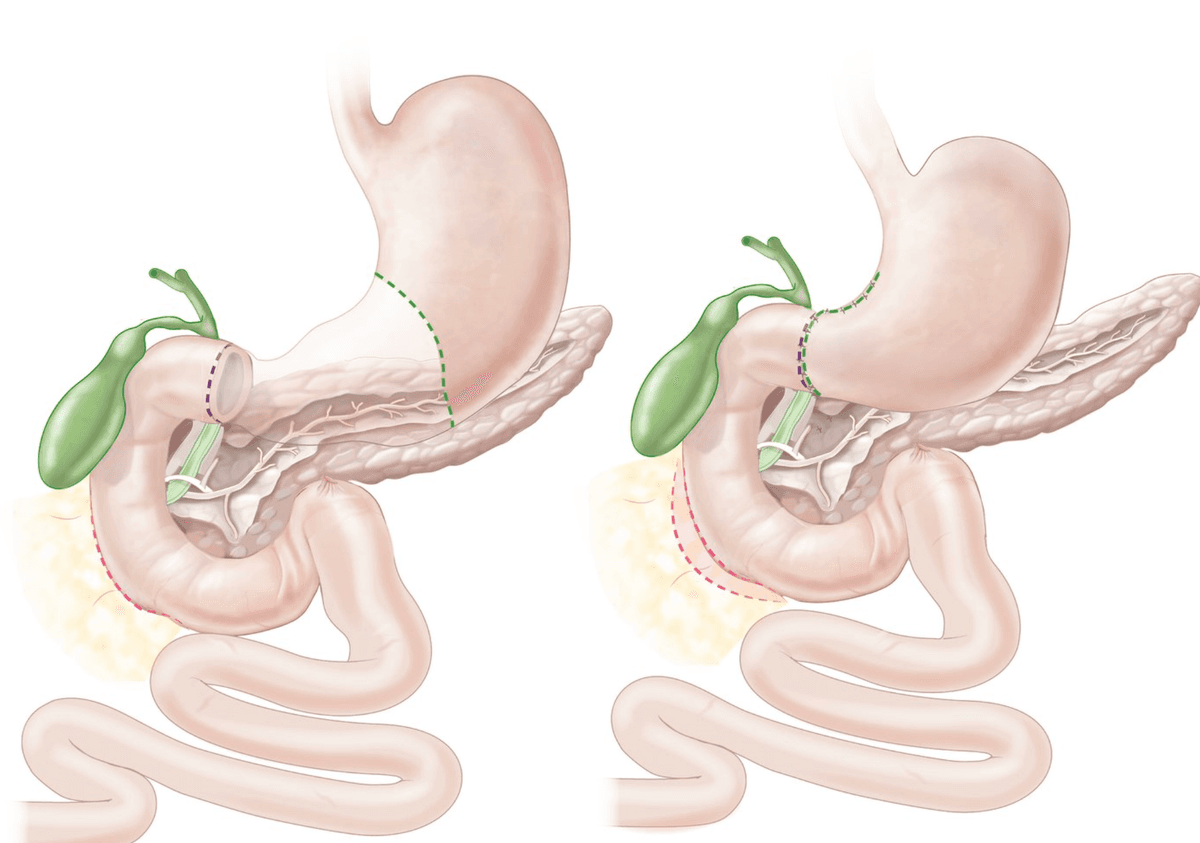
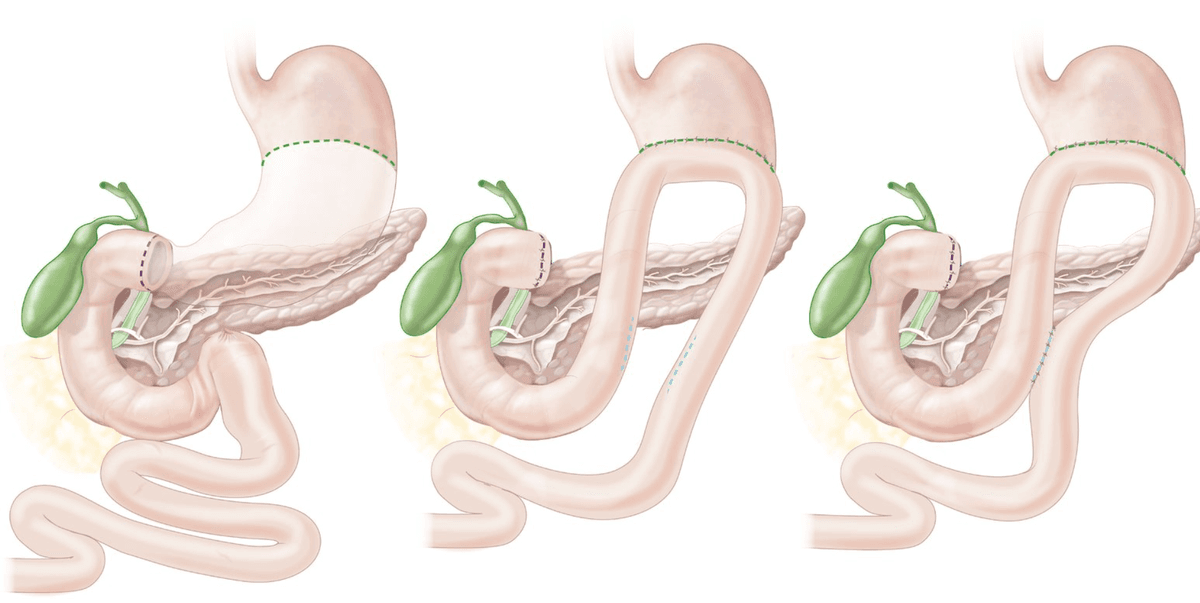
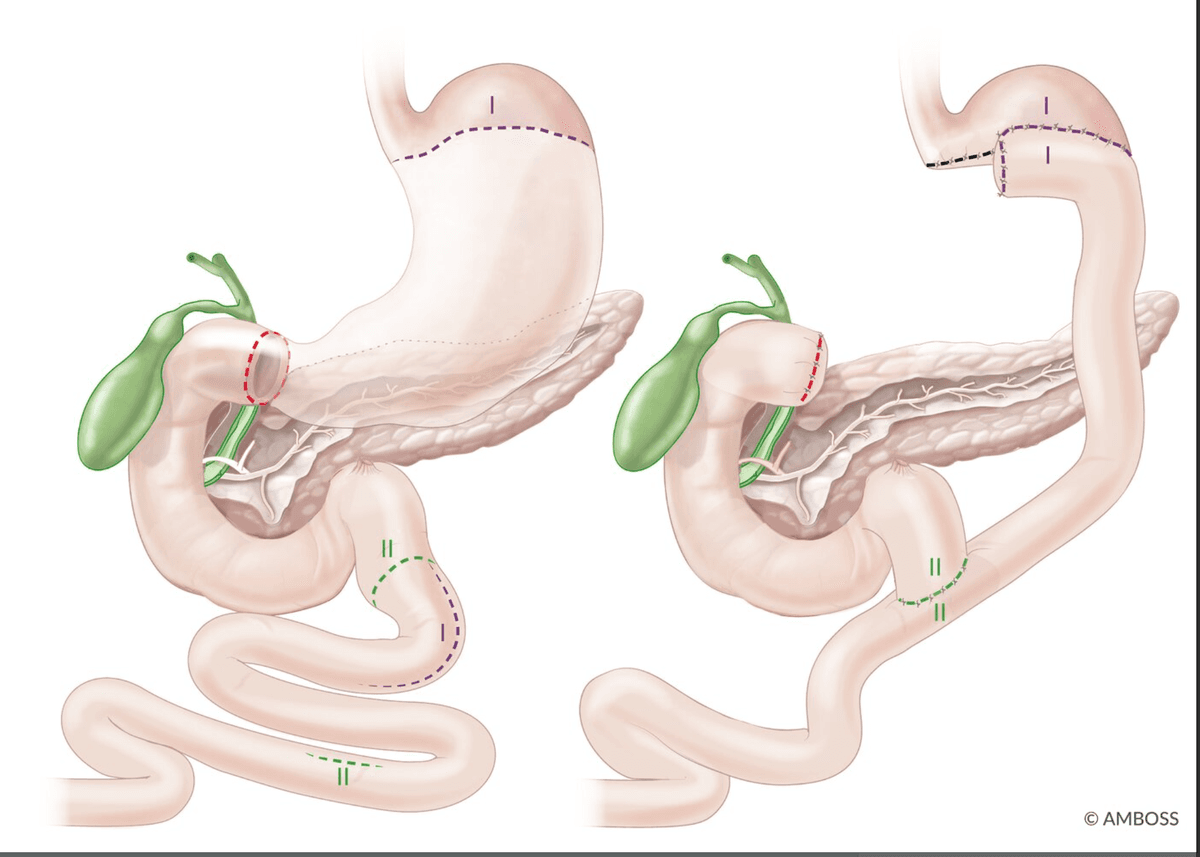
Why Roux-en-Y for total gastrectomy?
- After total gastrectomy, the oesophagus is anastomosed to a Roux limb of jejunum (a defunctionalised limb)
- This prevents bile reflux oesophagitis — a major problem with direct oesophagojejunostomy without a Roux limb, because bile and pancreatic juices would reflux into the oesophagus causing severe chemical injury
- Roux-en-Y oesophagojejunostomy is the standard reconstruction [5]
This is a critically important concept and frequently examined:
| Level | Stations Removed | Description |
|---|---|---|
| D1 lymphadenectomy | Stations 1–6 | Perigastric LNs only — along the greater and lesser curvature |
| D2 lymphadenectomy | Stations 1–6 + 7–11 | D1 + LNs along coeliac trunk, common hepatic artery, splenic artery, left gastric artery, and splenic hilum |
| D3 lymphadenectomy | Stations 1–11 + 12–16 | D2 + para-aortic, retropancreatic, mesenteric root LNs — NOT standard; only in clinical trials |
D2 lymphadenectomy is the STANDARD of care in patients with potentially curable gastric cancer [3][5]
Why D2 over D1?
- Better disease-specific survival [3]
- Allows more accurate N staging — minimises stage migration (Will Rogers phenomenon: removing more LNs → some N0 patients reclassified as N+ → apparent improvement in survival of both groups without any real treatment benefit — D2 avoids this artifact by providing a truer staging picture) [3]
- Requires removal of at least 15 lymph nodes for adequate staging (AJCC recommends ≥16) [3]
The trade-off:
- Higher perioperative morbidity and mortality compared to D1 — historically related to routine splenectomy and distal pancreatectomy performed during D2, which are now largely avoided unless the spleen/pancreas is directly invaded [3]
- In experienced centres (Japan, Korea, Hong Kong), the morbidity of D2 is now comparable to D1
Minimally invasive approach:
- Laparoscopic gastrectomy is increasingly performed for early gastric cancer [5] and even for advanced disease in experienced centres
- Benefits: reduced blood loss, shorter hospital stay, less postoperative pain, comparable oncological outcomes (in experienced hands)
V. Perioperative Chemotherapy — Neoadjuvant and Adjuvant
The evidence for perioperative chemotherapy in gastric cancer has evolved substantially. The approach differs slightly between Western and East Asian practice.
Preop neoadjuvant chemotherapy — selected patients [5]
HK: Upfront surgery is preferred — only consider if T3+ / N+ [17]
Rationale for neoadjuvant chemotherapy:
- Downstage the tumour to improve resectability rate [17] — shrink a borderline-resectable tumour to make R0 resection achievable
- Reduce rate of local and distant recurrence [3] — by treating micrometastatic disease early, before it becomes clinically apparent
- Allows assessment of in vivo chemosensitivity — if the tumour responds to neoadjuvant therapy, the same regimen can be continued adjuvantly; if it progresses, the regimen can be changed
Indications:
Regimens:
| Regimen | Drugs | Context |
|---|---|---|
| FLOT (current preferred Western standard) | Fluorouracil + Leucovorin (folinic acid) + Oxaliplatin + Docetaxel | Perioperative (4 cycles pre-op + 4 cycles post-op); based on the FLOT4-AIO trial showing superiority over ECF/ECX [17] |
| Xelox (if less fit) | Capecitabine + Oxaliplatin | Used in patients who cannot tolerate the FLOT regimen [17] |
| ECF / ECX (historical) | Epirubicin + Cisplatin + 5-FU (or Capecitabine) | MAGIC trial regimen; largely superseded by FLOT [3] |
Postop adjuvant chemotherapy — for advanced cancer [5]
Rationale:
- Eradicate micrometastasis remaining after surgery [17]
- Reduce risk of local and systemic recurrence
Indications:
- All patients except those with (T1-2; N0; M0) disease — since the majority of patients with locoregional disease are at high risk of recurrence following curative surgery [3]
- Consider if T3+ / N+ [17]
Regimens:
| Approach | Regimen | Trial Basis |
|---|---|---|
| Adjuvant chemo (East Asian preference) | 5-FU (or capecitabine) ± oxaliplatin (i.e., Xelox) or TS-1 | CLASSIC trial (capecitabine + oxaliplatin); ACTS-GC trial (TS-1 monotherapy — Japan) [17] |
| Adjuvant chemoradiation (US preference) | 5-FU / Leucovorin + Radiation therapy (4500 cGy) | US Intergroup 0116 (INT-0116 / Macdonald trial) — improved OS and DFS in resected Stage IB–IV (M0) gastric adenocarcinoma [5] |
| Perioperative chemo (Western preference) | FLOT x 4 pre-op + 4 post-op | FLOT4-AIO trial [17] |
East Asian vs Western Approach to Perioperative Therapy
There is a philosophical difference:
- East Asia (Japan, Korea, HK): Emphasis on upfront surgery with D2 lymphadenectomy → adjuvant chemotherapy post-op. Neoadjuvant is reserved for T3+/N+ only [17].
- Western (US, Europe): Emphasis on perioperative chemotherapy (neoadjuvant + adjuvant, e.g., FLOT) because D2 lymphadenectomy is less consistently performed and surgery alone has worse outcomes.
- Adjuvant chemoradiation (INT-0116 regimen) is favoured in the US, especially when D2 was NOT performed (radiation compensates for inadequate lymphadenectomy) [5].
In Hong Kong practice, the standard is closer to the East Asian model: upfront D2 gastrectomy → adjuvant chemo if T3+/N+, with neoadjuvant reserved for selected cases [17].
These are increasingly integrated into the treatment algorithm:
| Agent | Target | Indication |
|---|---|---|
| Trastuzumab (Herceptin) | HER2 | HER2-positive metastatic/advanced gastric cancer; combined with chemotherapy (ToGA trial) |
| Ramucirumab (Cyramza) | VEGFR2 | Second-line for advanced gastric cancer; anti-angiogenic monoclonal antibody (REGARD and RAINBOW trials) [17] |
| Nivolumab / Pembrolizumab | PD-1 | MSI-H/dMMR or PD-L1 CPS ≥ 5; now incorporated into first-line with chemo (CheckMate-649, KEYNOTE-859) |
| Zolbetuximab | Claudin 18.2 | CLDN18.2-positive, HER2-negative; first-line with chemo (SPOTLIGHT/GLOW trials — approved 2024) |
VI. Palliative Management [3][5][17]
Unresectable disease [5]:
Palliative care is indicated for patients with unequivocal evidence of incurability including metastasis, involvement of peritoneum, and N4/D3 nodal stage disease [3].
Principles: relieve pain, nutrition, bleeding, obstruction, perforation [17]
- Transfusion — for anaemia from chronic GI blood loss
- PPI — reduce acid secretion, promote ulcer healing, reduce bleeding
- Iron supplementation — for iron deficiency anaemia
- Pain control — WHO analgesic ladder; consider coeliac plexus block for intractable epigastric/back pain
- Nutritional support — oral supplements, enteral feeding (NJ tube), parenteral nutrition if necessary
| Problem | Endoscopic Treatment | Mechanism |
|---|---|---|
| Bleeding | Ethanol injection, adrenaline injection, clipping | Local haemostasis; adrenaline causes vasoconstriction; clipping mechanically occludes the bleeding vessel [17] |
| Gastric outlet obstruction | Metallic stenting (self-expandable metal stent — SEMS) | Bypasses the obstructing tumour; risk of re-stenosis by tumour ingrowth [17] |
| Luminal obstruction | Endoscopic laser ablation | Debulks intraluminal tumour to restore luminal patency [3] |
Endoscopic stenting [5] — quick, minimally invasive, provides rapid symptom relief, but less durable than surgical bypass.
| Problem | Surgical Option | Notes |
|---|---|---|
| Bleeding | Palliative gastrectomy or transcatheter arterial embolisation (TAE) | Gastrectomy removes the bleeding source; TAE is less invasive [3] |
| Gastric outlet obstruction | Palliative bypass (gastrojejunostomy / gastroenterostomy) | More durable than stenting but may cause impaired gastric emptying / bile reflux [17]; patient must be fit enough for surgery |
| Bleeding | External beam radiotherapy (EBRT) | Can reduce tumour vascularity and bleeding [3] |
Palliative resection: relieve bleeding / obstruction [17] Palliative bypass (gastrojejunostomy): more durable than stenting, but possible impaired gastric emptying / bile reflux [17]
Stent vs Bypass for Malignant GOO
- SEMS: Quick procedure, no GA needed, rapid oral intake resumption, but risk of tumour ingrowth/re-stenosis, stent migration; better for patients with short expected survival (< 3–6 months)
- Gastrojejunostomy: More durable, better long-term patency, but requires GA and laparotomy/laparoscopy; better for patients with longer expected survival (> 6 months) and those who fail stenting [17]
Palliative chemo ± HER2 inhibitor (if HER2 +ve) ± ramucirumab (VEGFR2 antagonist) [17]
For patients with metastatic or unresectable gastric cancer who have adequate performance status:
| Line | Regimen | Notes |
|---|---|---|
| First-line | Doublet/triplet chemo (e.g., fluoropyrimidine + platinum) ± nivolumab (if PD-L1 CPS ≥ 5) ± trastuzumab (if HER2+) ± zolbetuximab (if CLDN18.2+) | Backbone is cytotoxic chemotherapy with targeted/immune agents layered on based on biomarker status |
| Second-line | Paclitaxel ± ramucirumab (VEGFR2 antagonist) | Ramucirumab = anti-angiogenic monoclonal antibody; RAINBOW trial showed OS benefit [17] |
| Third-line+ | Trifluridine/tipiracil (TAS-102); nivolumab (if not given earlier); clinical trials | Options become limited; consider best supportive care |
External beam radiotherapy (EBRT) for painful bone metastases [17] — highly effective for pain palliation; single-fraction (8 Gy) or multi-fraction (30 Gy in 10 fractions) regimens.
VII. Post-Gastrectomy Complications and Long-Term Sequelae
Understanding these is essential because they affect long-term quality of life and are frequently examined:
| Complication | Mechanism | Management |
|---|---|---|
| Anastomotic leak | Failure of surgical anastomosis to heal; ischaemia, tension, or technical error | Sepsis workup, CT with oral contrast, NPO, drainage (percutaneous or re-operation) |
| Haemorrhage | Intra-abdominal bleeding from staple lines, vascular injury | Resuscitation, re-exploration if ongoing |
| Wound infection | Contamination during surgery | Antibiotics, wound care |
| Pneumonia / Atelectasis | Post-operative immobility, pain-related splinting | Chest physiotherapy, early mobilisation |
| Syndrome | Mechanism | Management |
|---|---|---|
| Dumping syndrome | Loss of pylorus → rapid gastric emptying of hyperosmolar carbohydrates → draw fluid into intestinal lumen + release of vasoactive gut hormones [17] | |
| — Early (15–30 min) | Osmotic fluid shift → hypovolaemia; gut hormone release → vasomotor symptoms | Small frequent meals, avoid simple carbs [17] |
| — Late (2–3 h) | Post-prandial hyperinsulinaemic hypoglycaemia (PHH) — reactive insulin overshoot after rapid glucose absorption [17] | Dietary modification; octreotide (inhibits insulin and gut hormone secretion) [17] |
| Small stomach syndrome | Reduced gastric reservoir capacity after gastrectomy | Early satiety; small frequent meals [17] |
| Alkaline reflux gastritis | Bile reflux into gastric remnant (especially Billroth II) | PPI, sucralfate; may need conversion to Roux-en-Y |
| Roux stasis syndrome | Ectopic pacemakers in Roux limb → net propulsive activity directed proximally towards the stomach → bloating, nausea/vomiting, delayed regurgitation [17] | Prokinetics (metoclopramide, erythromycin) |
| Afferent loop syndrome | Obstruction of the afferent limb (Billroth II) → bile/pancreatic juice accumulation → bilious vomiting (non-food) and epigastric pain relieved by vomiting [17] | Revision of GJ / conversion to Roux-en-Y / Braun enteroenterostomy [17] |
| Efferent loop syndrome | Obstruction of efferent limb → GOO | Surgical revision |
| Deficiency | Mechanism | Management |
|---|---|---|
| B12 deficiency (megaloblastic anaemia) | ↓ Gastric acid + ↓ intrinsic factor (parietal cells removed) | IM B12 every 3 months (lifelong) [17] |
| Iron deficiency (microcytic anaemia) | ↓ Gastric acid required to cleave iron from food + duodenal bypass (iron absorbed in duodenum) | Oral/IV iron supplementation [17] |
| Calcium deficiency (osteoporosis) | ↓ Gastric acid → impaired calcium absorption + loss of duodenal continuity (calcium absorbed in duodenum) | Calcium + vitamin D supplementation [17] |
| Fat-soluble vitamin deficiency (A, D, E, K) | Loss of duodenal continuity → bile and pancreatic enzymes mix with food further downstream → impaired fat digestion and absorption | Fat-soluble vitamin supplementation [17] |
| Steatorrhoea | Pancreaticobiliary-food mismatch (asynchrony); bacterial overgrowth in blind loops | Pancreatic enzyme supplementation; antibiotics for bacterial overgrowth [17] |
| Stage | Treatment | Key Points |
|---|---|---|
| T1a, N0, M0 (early, mucosal) | EMR / ESD [5] | Endoscopic surveillance annually if curative; salvage gastrectomy if non-curative |
| T1b, N0, M0 (early, submucosal) | Gastrectomy + D2 LN dissection [5] | LN met risk 15–25% precludes endoscopic treatment |
| T1-2, N0, M0 (localised) | Gastrectomy + D2 → observe | Low risk of recurrence; adjuvant chemo not routinely indicated |
| T3+, N+, M0 (locally advanced) | ± Neoadjuvant FLOT → Gastrectomy + D2 → Adjuvant chemo [5][17] | HK: may proceed with upfront surgery → adjuvant |
| Any T, any N, M1 (metastatic) | Palliative chemo ± targeted/immunotherapy; palliative surgery/stent/EBRT as needed [5][17] | Not curable; goal is symptom control and QoL |
High Yield Summary — Management of CA Stomach
- Only hope for cure = surgical resection with D2 lymphadenectomy (≥15 LNs).
- Early gastric cancer (T1a): EMR/ESD — rare in HK (no screening); ESD preferred over EMR for > 2 cm lesions (en bloc resection). Salvage gastrectomy if non-curative histology.
- Resectable (T1b–T4a): Gastrectomy (distal for distal tumours, total for proximal) + D2 lymphadenectomy ± perioperative chemotherapy. Neoadjuvant (FLOT) if T3+/N+.
- Unresectable/metastatic: Palliative chemo ± HER2 inhibitor ± ramucirumab ± immunotherapy; endoscopic stent for GOO; palliative GJ if longer survival expected; EBRT for bone mets; palliative gastrectomy for bleeding.
- Unresectability criteria: distant metastasis, peritoneal deposits, D3 nodal involvement, encasement of aorta/hepatic artery/coeliac axis/proximal splenic artery.
- Post-gastrectomy: Dumping syndrome (early + late), B12/iron/calcium deficiency, afferent loop syndrome, Roux stasis. Lifelong IM B12.
- HK context: ~70% present Stage III; upfront surgery preferred over neoadjuvant in most cases.
Active Recall - CA Stomach Management
References
[2] Senior notes: maxim.md (Gastric cancer — Management and Endoscopic treatment section) [3] Senior notes: felixlai.md (CA Stomach — Treatment section, pp. 413–415) [5] Lecture slides: GC 212. Weight loss and vomiting gastric cancer; abdominal imaging.pdf (p34, p35, p39, p41, p48, p49, p53) [17] Senior notes: maxim.md (Non-surgical treatments in CA stomach; Palliative care; Post-gastrectomy complications) [18] Senior notes: felixlai.md (General principles of resectability — pancreatic/biliary cancer framework, p. 503)
Complications of CA Stomach
Complications of gastric cancer can be broadly divided into two categories:
- Complications of the disease itself (from the tumour)
- Complications of treatment (from surgery, chemotherapy, and radiotherapy)
Understanding these requires connecting the pathophysiology of the tumour and the consequences of removing a major digestive organ.
I. Complications of the Disease (Tumour-Related)
These arise directly from the tumour's growth, invasion, ulceration, and metastasis.
Mechanism: The tumour ulcerates through the gastric mucosa → erosion of submucosal and mucosal blood vessels → bleeding into the GI lumen. This can be:
- Chronic occult bleeding → iron-deficiency anaemia (hypochromic microcytic) [19]
- Why iron deficiency? Chronic slow blood loss depletes iron stores faster than dietary intake can replenish them. Red blood cells cannot be loaded with haemoglobin without iron → microcytic, hypochromic anaemia.
- Often insidious — the patient gradually becomes fatigued, pale, and short of breath without realising they are bleeding.
- Acute overt bleeding → haematemesis and melaena [19]
- Haematemesis (vomiting blood) occurs when blood accumulates in the stomach; if slow, gastric acid converts haemoglobin to haematin → "coffee-ground" vomitus.
- Melaena (black, tarry stools) occurs when blood is digested during transit through the GI tract.
- Massive haemorrhage can present with haemodynamic instability (tachycardia, hypotension, shock).
Management:
- Acute: Resuscitation (IV fluids, blood transfusion), urgent OGD with endoscopic haemostasis (adrenaline injection, clipping, thermal coagulation)
- If endoscopy fails: Transcatheter arterial embolisation (TAE) or palliative surgery [17]
- Chronic: Iron supplementation (oral or IV), PPI (reduces acid-mediated re-bleeding), blood transfusion as needed [17]
- Palliative resection for bleeding [5] — in unresectable disease with refractory bleeding, palliative gastrectomy removes the bleeding source
- External beam radiotherapy (EBRT) can reduce tumour vascularity and control bleeding [3][17]
Mechanism: Tumour at the antrum or pylorus progressively narrows the gastric outlet → food cannot pass into the duodenum → proximal gastric distension.
Clinical features:
- Abdominal distension [19]
- Vomiting — characteristically non-bilious (obstruction is proximal to the ampulla of Vater), projectile, containing undigested food eaten hours or days previously [19]
- Succussion splash (audible splash on shaking the abdomen > 3 hours post-prandially)
- Progressive weight loss and dehydration
Metabolic consequences:
-
Risk of dehydration and electrolyte abnormalities including hyponatraemia, hypokalaemia, and metabolic alkalosis [19]
- Why? Repeated vomiting of gastric acid (HCl) → loss of H⁺ and Cl⁻ → hypochloraemic metabolic alkalosis
- Volume depletion → activation of the renin-angiotensin-aldosterone system → aldosterone promotes Na⁺ reabsorption in exchange for K⁺ and H⁺ excretion in the distal nephron → hypokalaemia + paradoxical aciduria (the kidneys excrete H⁺ to preserve K⁺ and Na⁺, worsening the alkalosis)
- This is a classic exam concept: vomiting → hypochloraemic, hypokalaemic metabolic alkalosis with paradoxical aciduria
-
Risk of aspiration pneumonia [19] — retained gastric contents can be regurgitated and aspirated into the lungs, especially in debilitated patients or when lying flat
Management:
- "Drip and suck" — NPO, IV fluids (normal saline + KCl), nasogastric decompression [12]
- IV PPI to reduce gastric secretion
- Palliative bypass (GJ) for outlet obstruction [5] — gastrojejunostomy bypasses the obstructed pylorus
- Endoscopic stenting [5] — self-expandable metal stent (SEMS) across the obstructing tumour for rapid relief
- Systemic chemotherapy [5] — may shrink the tumour and relieve obstruction
- If resectable: curative gastrectomy addresses both the cancer and the obstruction
Mechanism: Tumour necrosis and ulceration → full-thickness erosion through the gastric wall → loss of wall integrity → gastric contents (acid, food, bacteria) leak into the peritoneal cavity.
Consequence: Leads to peritonitis [19]
Clinical features:
- Sudden-onset severe generalised abdominal pain
- Board-like rigidity (involuntary guarding) — generalised peritoneal inflammation causes reflex contraction of the abdominal wall muscles
- Absent bowel sounds (paralytic ileus from peritoneal irritation)
- Sepsis (fever, tachycardia, hypotension)
- CXR: pneumoperitoneum (free gas under the diaphragm — gas escapes from the perforated stomach)
Management:
- Emergency resuscitation (IV fluids, broad-spectrum antibiotics, analgesia)
- Emergency surgery: exploration, washout, and either primary repair with omental patch (if small perforation in a palliative setting) or gastrectomy (if tumour is resectable)
- This is a rare presentation of gastric cancer and carries a poor prognosis
These are not "complications" in the traditional sense but rather the clinical consequences of tumour spread:
| Site of Metastasis | Complication | Mechanism |
|---|---|---|
| Liver | Hepatomegaly, jaundice, liver failure, portal hypertension, ascites | Tumour replaces hepatic parenchyma → loss of synthetic and excretory function; compression of intrahepatic bile ducts; portal vein compression → portal hypertension |
| Peritoneum | Malignant ascites, bowel obstruction | Peritoneal carcinomatosis → increased peritoneal capillary permeability + lymphatic obstruction → fluid accumulation; tumour deposits on bowel serosa → adhesions and mechanical obstruction |
| Ovaries (Krukenberg) | Pelvic mass, abdominal distension | Transcoelomic spread of signet ring cells with tropism for ovarian stroma |
| Bone | Pathological fractures, bone pain, hypercalcaemia | Osteolytic or osteoblastic metastases weaken bone architecture; tumour-mediated osteoclast activation releases calcium |
| Lung | Dyspnoea, cough, haemoptysis, pleural effusion, lymphangitis carcinomatosis | Haematogenous spread → pulmonary parenchymal deposits; lymphatic obstruction → interstitial oedema and pleural effusion |
| Brain (rare) | Headache, focal neurological deficits, seizures | Space-occupying lesion → raised intracranial pressure |
| Ureteric obstruction | Hydronephrosis, acute renal failure | Pelvic or retroperitoneal tumour deposits compress the ureters |
These occur due to tumour-secreted substances, not direct invasion:
| Syndrome | Mechanism | Complication |
|---|---|---|
| Trousseau's syndrome | Mucin-secreting adenocarcinoma releases procoagulant substances (tissue factor, mucins) → hypercoagulable state | Migratory superficial thrombophlebitis, DVT, PE |
| Nephrotic syndrome (membranous nephropathy) | Tumour antigens deposit in the glomerular basement membrane → immune complex formation → complement activation → podocyte damage [5] | Proteinuria, hypoalbuminaemia, peripheral oedema |
| Acanthosis nigricans | Tumour-secreted growth factors (TGF-α, IGF) stimulate keratinocyte proliferation | Velvety hyperpigmentation of skin folds |
| Dermatomyositis | Autoimmune paraneoplastic process | Proximal muscle weakness, heliotrope rash |
II. Complications of Treatment (Surgery-Related)
These are the complications that arise from gastrectomy and its reconstructions. They are best organised by timing.
| Complication | Mechanism | Management |
|---|---|---|
| Bleeding | Intra-operative haemorrhage from splenic hilum, short gastric vessels, or staple lines | Intra-operative haemostasis; post-op: blood transfusion, correction of coagulopathy; re-exploration if ongoing |
| Injury to neighbouring structures | Surgical dissection near the pancreas, spleen, transverse colon, duodenum → inadvertent damage [17] | Intra-operative recognition and repair; e.g., splenectomy if splenic injury, repair of serosal tears |
| Pancreatic injury/fistula | D2 lymphadenectomy involves dissection along the superior border of the pancreas and splenic hilum → risk of pancreatic parenchymal injury | Drain management; octreotide; TPN if high-output fistula |
| Complication | Mechanism | Clinical Features | Management |
|---|---|---|---|
| Wound infection | Contamination during GI surgery; patient often malnourished and immunocompromised | Erythema, swelling, purulent discharge at wound site | Wound care, antibiotics, drainage if abscess |
| Chest infection / Pneumonia | Post-operative pain limits deep breathing (splinting) → atelectasis → secondary infection; aspiration risk if vomiting | Fever, productive cough, reduced breath sounds, consolidation on CXR | Chest physiotherapy, antibiotics, early mobilisation |
| Post-operative ileus | Normal post-operative bowel paralysis from surgical handling, anaesthesia, opioids, electrolyte disturbance | Abdominal distension, absent bowel sounds, inability to pass flatus | NPO, NG tube, IV fluids, correct electrolytes; usually self-resolving |
| Anastomotic leak | Failure of the surgical join (oesophagojejunostomy, gastrojejunostomy, or jejunojejunostomy) to heal — due to ischaemia, tension, technical error, or patient factors (malnutrition, steroids, diabetes) | Usually appears POD 5–10 [3][17]; fever, tachycardia, abdominal pain/peritonitis, feculent/purulent drain output; CT: extraluminal fluid/gas collection | NPO, IV fluids, broad-spectrum antibiotics ± exploration and revision [17]; percutaneous drainage of collections; re-operation if haemodynamically unstable or peritonitis |
| Duodenal stump blowout | Specific to Billroth II / Roux-en-Y with closed duodenal stump; raised intraluminal pressure in the afferent loop → rupture of the duodenal closure | Sudden abdominal pain, peritonitis, bilious drain output | Emergency re-operation; consider tube duodenostomy if duodenal stump leak [17] |
| Chyle leak | Injury to lymphatic channels during D2 dissection (particularly around the coeliac axis) → chyle leaks into the peritoneal cavity | Milky drain output after resumption of enteral feeding; TG > 110 mg/dL in drain fluid | NPO + TPN (eliminates chyle production by removing enteral fat); octreotide; re-operation if > 1 L/day or not resolving |
Anastomotic Leak — The Most Feared Complication
Anastomotic leak after gastrectomy: OJ > GJ/JJ in frequency [17]. Oesophagojejunal (OJ) leaks are the most common and most dangerous because the oesophagus lacks a serosal layer (unlike bowel), making healing less reliable and leaks more likely. This is why patients are kept NPO for 5–7 days post-op, fed via a jejunostomy tube, and may undergo a contrast swallow (water-soluble) before oral intake is commenced to check for leak [3].
C. Late Complications (Weeks to Months/Years Post-op) [3][17]
These are the chronic sequelae of living without a stomach (or with a small gastric remnant). They are collectively known as post-gastrectomy syndromes.
| Complication | Mechanism | Management |
|---|---|---|
| Anastomotic stricture | Fibrosis and scarring at the anastomosis → progressive narrowing | Endoscopic balloon dilatation; rarely surgical revision |
| Afferent loop syndrome | Mechanical obstruction of the afferent limb (Billroth II/Roux-en-Y) due to kinking, anastomotic narrowing, adhesions, volvulus, or internal herniation [3][17] | Conversion to Roux-en-Y / Braun enteroenterostomy [17] |
| Efferent loop syndrome | Obstruction of the efferent limb → GOO | Surgical revision |
| Internal hernia (Petersen's defect) | Bowel herniates through the mesenteric defect created during Roux-en-Y reconstruction | Surgical reduction and closure of defect |
| Jejuno-gastric intussusception | Efferent limb intussuscepts retrogradely into the gastric remnant → GOO | Surgical reduction |
Afferent loop syndrome — in more detail [3][17]:
- The afferent limb carries bile and pancreatic secretions from the duodenum to the gastrojejunal anastomosis
- If this limb becomes obstructed, bile and pancreatic juice accumulate → progressive distension
- Acute presentation: severe epigastric pain, non-bilious vomiting (bilious only after obstruction relieves), deranged LFT and raised amylase [17]
- Emergency: closed-loop obstruction → risk of duodenal stump blowout, obstructive jaundice, ascending cholangitis, pancreatitis [17]
- Why? The accumulated bile and pancreatic juice transmit high pressure back to the biliopancreatic ductal system [3]
- Chronic presentation: post-prandial pain, intermittent bilious vomiting [17]
- Usually due to excessive length of afferent loop [17]
- Dx: CT abdomen (dilated afferent loop) [17]
- Mx: revise GJ / convert to Roux-en-Y / Braun enteroenterostomy [17]
| Syndrome | Mechanism | Clinical Features | Management |
|---|---|---|---|
| Dumping syndrome | Loss of pylorus → rapid gastric emptying of hyperosmolar carbohydrates → draw fluid into intestinal lumen and release vasoactive gut hormones [17] | ||
| — Early (15–30 min) | Osmotic fluid shift → intravascular hypovolaemia; rapid gut hormone (serotonin, VIP, neurotensin) release → vasomotor symptoms | Abdominal pain, nausea/vomiting/diarrhoea, vasomotor symptoms (sweating, flushing, palpitations, dizziness) [17] | Small frequent meals, avoid simple carbohydrates [17] |
| — Late (2–3 hours) | Rapid glucose absorption → exaggerated insulin secretion → post-prandial hyperinsulinaemic hypoglycaemia (PHH) [17] | Tremor, sweating, confusion, palpitations (neuroglycopaenic and adrenergic symptoms of hypoglycaemia) | Dietary modification; octreotide (inhibits insulin secretion and delays gut transit) [17] |
| Small stomach syndrome | Reduced gastric reservoir after gastrectomy → cannot accommodate normal meal volume | Early satiety [3][17] | Small frequent meals (6+ per day) |
| Gastric stasis | Impaired gastric emptying due to post-operative atony / vagal denervation [17] | Nausea, vomiting, bloating, retained food | Prokinetics (metoclopramide, erythromycin) [17] |
| Alkaline reflux gastritis | Bile reflux into the gastric remnant (especially after Billroth II where the afferent loop delivers bile directly to the gastric stump) | Epigastric burning pain, bilious vomiting, endoscopic appearance of inflamed, bile-stained mucosa | PPI, sucralfate, cholestyramine (bile acid binder); conversion to Roux-en-Y if refractory |
| Roux stasis syndrome | Ectopic pacemakers in the Roux limb → net propulsive activity directed proximally towards the stomach rather than distally [17] — the Roux limb effectively pushes contents backwards | Bloating, nausea/vomiting, heartburn, delayed regurgitation [17] | Prokinetics (metoclopramide, erythromycin); surgical shortening of Roux limb |
| Post-vagotomy diarrhoea | Alteration in gastric emptying and vagal denervation of the small bowel and biliary tree [3] — bile acid malabsorption and rapid small bowel transit | Watery, episodic diarrhoea (occurs in ~20% after truncal vagotomy) [3] | Decrease excessive fluid intake, avoid lactose; antidiarrhoeal medications (loperamide) [3]; cholestyramine (binds bile acids) |
Understanding Dumping Syndrome From First Principles
The pylorus normally acts as a "gatekeeper" — it meters out small amounts of chyme into the duodenum in a controlled fashion. When you remove the pylorus (distal gastrectomy) or bypass it entirely (total gastrectomy with Roux-en-Y), hyperosmolar food (especially simple sugars) rushes into the small bowel unregulated. This creates an osmotic gradient that draws water from the intravascular space into the bowel lumen (early dumping — hypovolaemia, vasomotor symptoms). The rapid glucose absorption then triggers a massive insulin spike that overshoots, causing reactive hypoglycaemia 2–3 hours later (late dumping). The treatment is logical: eat small meals, avoid simple sugars (reduce the osmotic load), and in refractory cases, use octreotide (a somatostatin analogue that inhibits GI hormone secretion and slows transit) [17].
These are inevitable long-term consequences of gastrectomy and require lifelong supplementation:
| Deficiency | Mechanism | Clinical Consequence | Management |
|---|---|---|---|
| Vitamin B12 deficiency | ↓ Gastric acid + ↓ intrinsic factor — parietal cells (which produce intrinsic factor needed for B12 absorption in the terminal ileum) are removed with the stomach [17] | Megaloblastic anaemia (macrocytic), subacute combined degeneration of the spinal cord, peripheral neuropathy, glossitis | IM B12 every 3 months (lifelong) [17] — oral B12 is insufficient because intrinsic factor is absent |
| Iron deficiency | ↓ Gastric acid required to cleave iron from food (acid converts Fe³⁺ to Fe²⁺, the absorbable form) + bypass of duodenum (primary site of iron absorption) [17] | Microcytic hypochromic anaemia, koilonychia, glossitis | Oral iron supplementation (take with vitamin C to enhance absorption); IV iron if oral is insufficient |
| Calcium deficiency | ↓ Gastric acid → impaired calcium solubilisation and absorption + loss of duodenal continuity (calcium absorbed in duodenum) [17] | Osteoporosis, pathological fractures, tetany (if severe hypocalcaemia) | Calcium + vitamin D supplementation; DEXA scanning for osteoporosis monitoring |
| Fat-soluble vitamin deficiency (A, D, E, K) | Loss of duodenal continuity → bile and pancreatic enzymes mix with food further downstream → impaired fat digestion → impaired fat-soluble vitamin absorption [17] | Vitamin D: osteomalacia; Vitamin K: coagulopathy; Vitamin A: night blindness; Vitamin E: neurological dysfunction | Fat-soluble vitamin supplementation |
| Steatorrhoea | Pancreaticobiliary-food asynchrony (food reaches the jejunum before bile/pancreatic juice can mix with it); bacterial overgrowth in blind loops (afferent limb) [17] | Fatty, foul-smelling, floating stools; weight loss; fat-soluble vitamin deficiency | Pancreatic enzyme supplementation; antibiotics for bacterial overgrowth |
- Usually at the gastric bed [17] — the site of the original tumour
- Can also recur at the anastomosis, peritoneum, liver, or distant sites
- Monitored by:
- Regular clinical follow-up (symptoms, examination)
- Serial tumour markers (CEA, CA19-9) — a rising level after initial post-operative normalisation is suspicious
- Surveillance CT scans
- Endoscopic surveillance of the anastomosis
| Complication | Mechanism | Notes |
|---|---|---|
| Myelosuppression (neutropaenia, thrombocytopaenia, anaemia) | Cytotoxic drugs kill rapidly dividing cells, including bone marrow haematopoietic progenitors | Increased infection risk (neutropaenic sepsis), bleeding risk, fatigue; manage with G-CSF, transfusions |
| Nausea / Vomiting | Chemotherapy triggers the chemoreceptor trigger zone (area postrema) and damages GI mucosa | Anti-emetics: 5-HT₃ antagonists (ondansetron), NK1 antagonists (aprepitant), dexamethasone |
| Mucositis / Stomatitis | Damage to rapidly dividing mucosal epithelial cells | Oral care, analgesic mouthwashes |
| Peripheral neuropathy | Oxaliplatin (component of FLOT/Xelox) causes dorsal root ganglion neurotoxicity | Dose-limiting; may be irreversible; cold-induced dysaesthesia is characteristic of oxaliplatin |
| Cardiotoxicity | 5-FU can cause coronary vasospasm; trastuzumab can reduce LV ejection fraction | Cardiac monitoring (ECG, echocardiography) |
| Diarrhoea | GI mucosal damage; 5-FU and irinotecan are particularly associated | Loperamide; IV fluids if severe |
| Hand-foot syndrome | Capecitabine (oral 5-FU prodrug) concentrates in palms/soles → painful erythema, desquamation | Dose reduction; emollients; pyridoxine (vitamin B6) |
| Radiation-induced complications | Radiation to the gastric bed damages adjacent structures (liver, kidneys, small bowel, spinal cord) | Radiation enteritis, nephrotoxicity; strict field planning to minimise collateral damage |
Prognostic indicators [19]:
- Depth of invasion (T stage) — the single most important prognostic factor [2]
- Lymph node involvement (N stage)
- Degree of differentiation — poorly differentiated tumours have worse outcomes
- Additional factors: Lauren type (diffuse worse than intestinal), resection margin status (R0 vs R1/R2), lymphovascular invasion, molecular subtype (MSI-H better prognosis)
| Stage | Approximate 5-Year Survival |
|---|---|
| Stage IA (T1N0) | > 90% |
| Stage IB–IIA | 60–80% |
| Stage IIB–IIIA | 35–60% |
| Stage IIIB–IIIC | 15–30% |
| Stage IV (M1) | < 5% |
High Yield Summary — Complications of CA Stomach
Disease complications:
- Bleeding: Chronic (IDA) or acute (haematemesis/melaena); manage with endoscopy, TAE, palliative resection, or EBRT.
- GOO: Non-bilious vomiting, hypochloraemic hypokalaemic metabolic alkalosis with paradoxical aciduria; manage with drip-and-suck, stenting, or palliative GJ.
- Perforation: Peritonitis; emergency surgery.
- Metastatic: Liver failure, malignant ascites, Krukenberg tumour, hydronephrosis, bone pain, brain mets.
- Paraneoplastic: Trousseau's syndrome, membranous nephropathy, acanthosis nigricans.
Post-gastrectomy complications:
- Early: Anastomotic leak (OJ > GJ/JJ, POD 5–10), duodenal stump blowout, bleeding, infection, chyle leak.
- Anastomosis-related late: Afferent loop syndrome (bilious vomiting, risk of stump blowout/cholangitis), efferent loop syndrome, internal hernia (Petersen's defect), stricture.
- Motility-related late: Dumping syndrome (early: osmotic; late: hyperinsulinaemic hypoglycaemia), small stomach syndrome, gastric stasis, alkaline reflux gastritis, Roux stasis syndrome.
- Nutritional: B12 deficiency (IM B12 Q3mo lifelong), iron deficiency, calcium deficiency (osteoporosis), fat-soluble vitamin deficiency, steatorrhoea.
- Recurrence: Usually at gastric bed; monitor with CEA/CA19-9 and CT.
Prognostic factors: Depth of invasion (most important), LN involvement, differentiation grade.
Active Recall - CA Stomach Complications
References
[2] Senior notes: maxim.md (Gastric cancer — Staging and Investigations section) [3] Senior notes: felixlai.md (CA Stomach — Complications and Treatment sections, pp. 413–419) [5] Lecture slides: GC 212. Weight loss and vomiting gastric cancer; abdominal imaging.pdf (p53) [12] Senior notes: maxim.md (Gastric outlet obstruction section) [17] Senior notes: maxim.md (Post-gastrectomy complications section; Palliative care section; Nutritional deficiency section) [19] Senior notes: felixlai.md (CA Stomach — Complications section, p. 419; Prognosis section)
High Yield Summary
Definition: Gastric cancer = predominantly adenocarcinoma (90%) of the stomach; classified by Lauren into intestinal (well-differentiated, elderly male, distal, better prognosis) and diffuse (undifferentiated, young female, proximal, worse prognosis).
Epidemiology (HK): 6th most common cancer, 4th–5th mortality; M:F = 1.5:1; declining incidence overall but cardia cancers increasing.
Key Risk Factors: H. pylori (WHO Group 1 carcinogen — Correa cascade), EBV (10%), atrophic gastritis (MOST common precursor), pernicious anaemia, Menetrier's disease, adenomatous polyps, prior gastrectomy (>20 yrs, bile reflux), dietary nitrosamines/smoked/pickled/salted food, smoking, HDGC (E-cadherin/CDH1 mutation → prophylactic gastrectomy), FAP, HNPCC, CVID.
Protective: Fresh fruits/vegetables, vitamin C, selenium.
Pathophysiology: Intestinal type follows the Correa cascade (normal → chronic gastritis → atrophy → intestinal metaplasia → dysplasia → carcinoma). Diffuse type driven by E-cadherin loss → signet ring cells, linitis plastica.
Spread: Lymphatic (most common), haematogenous (liver > lung), transcoelomic (peritoneum, Krukenberg tumour), direct invasion.
Clinical Features: Often asymptomatic early. Alarm symptoms: weight loss, dysphagia, vomiting, GI bleed, epigastric mass, anaemia. Key metastatic signs: Virchow's node, Sister Mary Joseph's nodule, Krukenberg tumour, Blumer's shelf.
Linitis plastica: Diffuse type, leather bottle stomach, hard to biopsy endoscopically (submucosal infiltration), poor prognosis, 1/3 have peritoneal mets at diagnosis.
High Yield Summary — Differential Diagnosis of CA Stomach
- The DDx depends on the presenting syndrome: dyspepsia (functional dyspepsia, PUD, GERD, chronic pancreatitis, pancreatic cancer), UGIB (PUD most common, varices, Mallory-Weiss, Dieulafoy), GOO (malignant 80% — CA stomach most common; benign 20% — PUD stricture), dysphagia (oesophageal cancer, achalasia/pseudoachalasia), epigastric mass (lymphoma, GIST, pancreatic mass, omental cake).
- Gastric ulcers must always be biopsied — they can harbour carcinoma.
- GOO is malignant until proven otherwise.
- Pseudoachalasia (malignancy mimicking achalasia) must be excluded by OGD ± EUS before diagnosing achalasia.
- For submucosal gastric masses: think GIST (CD117+, muscularis propria), lymphoma (submucosa), NET — require EUS ± FNA.
- Non-GI causes: pancreatic cancer, liver metastases, HCC, mesenteric ischaemia.
High Yield Summary — Diagnosis of CA Stomach
- Gold standard: OGD + multiple biopsies (≥6 from ulcer margins). Request histology + HER2 + MSI/MMR + PD-L1 + CLDN18.2 on all new diagnoses.
- Tumour markers (CEA, CA19-9, CA125) are NOT diagnostic — used for follow-up and monitoring recurrence only.
- Staging workup: CT TAP with contrast (mandatory for M staging, not accurate for T/N); EUS (best for T/N but NOT mandatory — upfront surgery advocated); Staging laparoscopy + peritoneal lavage (routine — more accurate than CT for peritoneal disease); PET-CT (adjunct, not sensitive for mucinous/signet ring tumours).
- Linitis plastica is the diagnostic trap: normal-appearing mucosa on OGD, non-distensible stomach, requires deep biopsies + EUS + barium swallow.
- Benign vs malignant ulcer: benign = smooth, regular, rounded edges, flat base; malignant = irregular, thickened edges, nodular/clubbed/fused surrounding folds. ALL gastric ulcers must be biopsied and followed up.
- Clinical staging checklist (from lecture): H&P, LFT, CXR, USG/CT abdomen, PET/CT, EUS, laparoscopy.
High Yield Summary — Management of CA Stomach
- Only hope for cure = surgical resection with D2 lymphadenectomy (≥15 LNs).
- Early gastric cancer (T1a): EMR/ESD — rare in HK (no screening); ESD preferred over EMR for > 2 cm lesions (en bloc resection). Salvage gastrectomy if non-curative histology.
- Resectable (T1b–T4a): Gastrectomy (distal for distal tumours, total for proximal) + D2 lymphadenectomy ± perioperative chemotherapy. Neoadjuvant (FLOT) if T3+/N+.
- Unresectable/metastatic: Palliative chemo ± HER2 inhibitor ± ramucirumab ± immunotherapy; endoscopic stent for GOO; palliative GJ if longer survival expected; EBRT for bone mets; palliative gastrectomy for bleeding.
- Unresectability criteria: distant metastasis, peritoneal deposits, D3 nodal involvement, encasement of aorta/hepatic artery/coeliac axis/proximal splenic artery.
- Post-gastrectomy: Dumping syndrome (early + late), B12/iron/calcium deficiency, afferent loop syndrome, Roux stasis. Lifelong IM B12.
- HK context: ~70% present Stage III; upfront surgery preferred over neoadjuvant in most cases.
High Yield Summary — Complications of CA Stomach
Disease complications:
- Bleeding: Chronic (IDA) or acute (haematemesis/melaena); manage with endoscopy, TAE, palliative resection, or EBRT.
- GOO: Non-bilious vomiting, hypochloraemic hypokalaemic metabolic alkalosis with paradoxical aciduria; manage with drip-and-suck, stenting, or palliative GJ.
- Perforation: Peritonitis; emergency surgery.
- Metastatic: Liver failure, malignant ascites, Krukenberg tumour, hydronephrosis, bone pain, brain mets.
- Paraneoplastic: Trousseau's syndrome, membranous nephropathy, acanthosis nigricans.
Post-gastrectomy complications:
- Early: Anastomotic leak (OJ > GJ/JJ, POD 5–10), duodenal stump blowout, bleeding, infection, chyle leak.
- Anastomosis-related late: Afferent loop syndrome (bilious vomiting, risk of stump blowout/cholangitis), efferent loop syndrome, internal hernia (Petersen's defect), stricture.
- Motility-related late: Dumping syndrome (early: osmotic; late: hyperinsulinaemic hypoglycaemia), small stomach syndrome, gastric stasis, alkaline reflux gastritis, Roux stasis syndrome.
- Nutritional: B12 deficiency (IM B12 Q3mo lifelong), iron deficiency, calcium deficiency (osteoporosis), fat-soluble vitamin deficiency, steatorrhoea.
- Recurrence: Usually at gastric bed; monitor with CEA/CA19-9 and CT.
Prognostic factors: Depth of invasion (most important), LN involvement, differentiation grade.
Ca Esophagus
Esophageal cancer is a malignant neoplasm of the esophageal mucosa, predominantly squamous cell carcinoma or adenocarcinoma, presenting with progressive dysphagia and weight loss.
Dysphagia
Dysphagia is difficulty in swallowing solids, liquids, or both, resulting from functional or structural impairment of the oral, pharyngeal, or esophageal phases of deglutition.