Streptococcus pyogenes
A clinically integrated guide to group A streptococcal biology, disease, diagnosis, treatment, post-infectious sequelae, and Sketchy recall.
Foundations: From a Chain-Forming Coccus to Toxin and Immune Disease
| Property | Streptococcus pyogenes | Why it matters |
|---|---|---|
| Common names | Group A Streptococcus (GAS), group A β-haemolytic streptococcus | Lancefield group A carbohydrate and β-haemolysis are the classic laboratory identity. |
| Gram/morphology | Gram-positive cocci in chains or pairs | Division in one plane without complete separation produces chains; a thick peptidoglycan wall retains crystal violet. |
| Physiology | Catalase negative, non-motile, non-spore-forming, aerotolerant facultative anaerobe | Catalase separates streptococci from staphylococci; oxygen tolerance permits growth on mucosa and damaged tissue. |
| Reservoir | Humans: pharynx and skin | Respiratory droplets/direct secretions spread pharyngeal disease; direct contact spreads skin disease. |
| Capsule | Hyaluronic acid | Mimics host connective-tissue material, so it is poorly immunogenic and inhibits phagocytosis. |
| Surface antigen | M protein, encoded by emm | Major anti-phagocytic factor and epidemiological typing target; some immune responses cross-react with host tissue. |
| Major disease families | Pharyngitis/scarlet fever; impetigo/erysipelas/cellulitis; invasive disease; ARF and PSGN | One organism causes local infection, toxin-mediated disease, destructive invasion, and delayed immune sequelae. |
GC 105 places GAS among the β-haemolytic streptococci and explicitly links it to pharyngitis, scarlet fever, impetigo, cellulitis, necrotising fasciitis, toxic shock, acute rheumatic fever, and PSGN. [1]
“Strepto-” comes from Greek streptos, twisted or chain-like; “-coccus” means a spherical cell; “pyogenes” means pus-producing. The name therefore previews both morphology and clinical behaviour.
| Structure/factor | Host interaction | Consequence |
|---|---|---|
| M protein | Binds host factors and impairs complement deposition/opsonophagocytosis | Persistence on mucosa and tissue; type-specific immunity; molecular-mimicry link to ARF. |
| Hyaluronic-acid capsule | Resembles host hyaluronan and physically limits phagocyte access | Immune camouflage and anti-phagocytic survival without a strongly immunogenic capsule. |
| Lipoteichoic acid and protein F | Bind epithelial fibronectin | Pharyngeal/skin adherence establishes the infection before invasion. |
| C5a peptidase | Cleaves the neutrophil chemoattractant C5a | Delays neutrophil recruitment at the inoculation site. |
| Streptolysin O | Oxygen-labile pore-forming toxin lyses RBCs, leukocytes, and platelets | Tissue damage; immunogenicity permits ASO serology after pharyngeal infection. |
| Streptolysin S | Oxygen-stable cytolysin injures cells | Responsible for surface β-haemolysis and contributes to tissue injury; poorly immunogenic. |
| Streptokinase | Converts plasminogen to plasmin | Dissolves fibrin barriers and promotes spread through tissue planes. |
| DNases | Degrade DNA in pus and neutrophil extracellular traps | Liquefy viscous exudate and facilitate escape; anti-DNase B documents recent skin or throat infection. |
| SpeA/SpeC and related pyrogenic exotoxins | Cross-link MHC II to T-cell receptor outside the peptide groove | Superantigen-driven cytokine release → scarlet fever and streptococcal toxic shock syndrome. |
| SpeB | Secreted cysteine protease cleaves host matrix and immune proteins | Promotes invasive tissue destruction; also serves as a candidate nephritogenic antigen in PSGN. |
The same virulence programme changes meaning with anatomical depth. Adherence and local inflammation cause pharyngitis; toxin release creates a systemic rash without requiring bacteraemia; anti-phagocytic factors plus tissue-spreading enzymes permit invasive disease; antibodies and immune complexes create disease after viable bacteria have disappeared.
Complete lysis of sheep RBCs around colonies produces a clear zone: β-haemolysis. GAS is classically PYR positive and bacitracin susceptible, whereas group B streptococcus is PYR negative and bacitracin resistant. These are useful teaching discriminators, but modern laboratories commonly use MALDI-TOF, antigen grouping, or molecular identification rather than bacitracin alone.
| Organism | Haemolysis | Catalase | Classical discriminator | Signature disease |
|---|---|---|---|---|
| S. pyogenes | β | Negative | Group A antigen, PYR positive | Pharyngitis, impetigo, invasive GAS, ARF, PSGN |
| S. agalactiae | Usually β | Negative | Group B antigen, CAMP positive, hippurate positive | Neonatal sepsis/meningitis, peripartum infection |
| S. pneumoniae | α | Negative | Optochin susceptible, bile soluble | Pneumonia, meningitis, otitis |
| Viridans streptococci | α or non-haemolytic | Negative | Optochin resistant, bile insoluble | Dental caries, subacute endocarditis |
| Staphylococcus aureus | Often β | Positive | Coagulase positive; clusters | Abscesses, bacteraemia, toxin disease |
High Yield Summary
- GAS is a catalase-negative, β-haemolytic Gram-positive coccus in chains with group A carbohydrate.
- M protein and the hyaluronic-acid capsule resist opsonophagocytosis; adhesins establish pharyngeal and skin infection.
- Streptolysins injure cells, streptokinase and DNases open tissue pathways, and Spe toxins drive superantigen disease.
- Local infection, toxin disease, invasive destruction, and delayed immune sequelae are four different pathogenetic modes.
- PYR positivity and classic bacitracin susceptibility distinguish GAS from GBS in teaching laboratories.
Active Recall - GAS Foundations
[1] Lecture slides: GC 105. Medically important microbes what every doctor should know.pdf (β-haemolytic streptococcal classification and disease spectrum) [2] Lecture slides: GC 050. Fever and a murmur.pdf (Lancefield/haemolysis classification and GAS syndromes) [3] CDC: Clinical Considerations for Group A Streptococcus (updated August 2025) [4] Existing MBBSPedia: Necrotizing fasciitis — Etiology (GAS toxins, enzymes, and invasive pathogenesis)
Clinical Disease: Recognise Depth, Toxin Effects, and Timing
| Disease mode | Syndromes | Dominant mechanism |
|---|---|---|
| Local mucosal | Pharyngitis/tonsillitis | Epithelial adherence plus neutrophilic inflammation |
| Local cutaneous | Impetigo, erysipelas, non-purulent cellulitis | Entry through skin breaks followed by superficial or dermal spread |
| Toxin mediated | Scarlet fever, streptococcal toxic shock syndrome (STSS) | Pyrogenic exotoxin superantigen activity |
| Invasive | Bacteraemia, puerperal sepsis, necrotising fasciitis, myositis | Anti-phagocytic survival, enzymatic spread, direct tissue injury |
| Post-infectious | Acute rheumatic fever (ARF), post-streptococcal glomerulonephritis (PSGN) | Molecular mimicry or immune-complex/complement injury |
GC 105 teaches this exact breadth: pharyngitis, scarlet fever, impetigo, cellulitis, necrotising fasciitis, toxic shock, ARF, and PSGN should be recognised as one GAS spectrum. [1]
Typical GAS pharyngitis has abrupt sore throat, fever, painful swallowing, tonsillopharyngeal erythema/exudate, palatal petechiae, and tender anterior cervical nodes. Cough, coryza, hoarseness, oral ulcers, and conjunctivitis favour a viral cause. Children may have abdominal pain, nausea, or vomiting.
Clinical scoring estimates probability; it does not prove the organism. HKUMed lecture material emphasises that GAS pharyngitis is a microbiological diagnosis, and current guidance confirms with RADT or culture when viral features are absent and testing is indicated. [2][3]
Scarlet fever is GAS infection plus a pyrogenic exotoxin-associated scarlatiniform rash:
- Pharyngitis and fever usually precede or accompany the eruption.
- The fine erythematous rash blanches and feels like sandpaper.
- It starts on the trunk/groin and spreads, with relative sparing of palms and soles.
- Flexural accentuation produces Pastia lines.
- Circumoral pallor and a white then red strawberry tongue are classic.
- Desquamation follows as the rash resolves.
The rash is not bacteria spreading through skin. Superantigen-induced cytokines alter cutaneous vessels, producing a diffuse toxin phenotype.
| Syndrome | Anatomical level | Recognition | GAS logic |
|---|---|---|---|
| Non-bullous impetigo | Very superficial epidermis | Vesicle/pustule ruptures → honey-coloured crust, commonly perinasal/perioral | GAS or S. aureus enters minor skin breaks; bullous impetigo is toxin-producing S. aureus, not GAS. |
| Erysipelas | Upper dermis and superficial lymphatics | Bright red, raised, sharply demarcated tender plaque | Lymphatic involvement creates oedema and a “step-off” edge; GAS is classic. |
| Cellulitis | Deep dermis/subcutaneous tissue | Warm, tender, spreading erythema with poorly defined margin | GAS spreads diffusely; purulence/abscess shifts concern toward S. aureus. |
| Necrotising fasciitis | Fascia and deep soft tissue | Pain out of proportion, rapid progression, oedema beyond erythema, bullae, dusky skin, systemic toxicity, later anaesthesia | Toxins/enzymes and microvascular thrombosis destroy deep tissue before surface signs become dramatic. |
CFB Dermatology teaches that delay in necrotising fasciitis diagnosis and treatment markedly worsens mortality: early surgical and ICU involvement is part of recognition, not an afterthought. [4]
STSS is invasive GAS infection with abrupt shock and organ failure. Superantigens cross-link antigen-presenting cells and T cells non-specifically, activating a large T-cell fraction:
Early symptoms can resemble influenza or gastroenteritis. Severe focal pain, rapidly progressive swelling, hypotension, AKI, coagulopathy, ARDS, or hepatic injury should trigger a search for a deep source requiring surgery.
| Feature | ARF | PSGN |
|---|---|---|
| Preceding GAS site | Pharyngitis | Pharyngitis or skin infection |
| Typical latency | About 2–4 weeks; chorea may be later | Roughly 1–3 weeks after pharyngitis; often 3–6 weeks after skin infection |
| Mechanism | Cross-reactive adaptive immunity | Streptococcal antigens/immune complexes activate glomerular complement |
| Main phenotype | Migratory large-joint arthritis, carditis, chorea, erythema marginatum, nodules | Cola urine, oedema, hypertension, oliguria, renal impairment |
| Antibiotic prevention | Timely pharyngitis treatment reduces ARF | Treatment does not reliably prevent PSGN |
| Presentation | Important alternative | Discriminator |
|---|---|---|
| Exudative pharyngitis | EBV | Posterior/generalised nodes, hepatosplenomegaly, atypical lymphocytes; aminopenicillin-associated rash |
| Sandpaper rash | Viral exanthem, Kawasaki disease | Confirm GAS; Kawasaki has prolonged fever, conjunctivitis, mucosal/extremity changes and lymphadenopathy |
| Honey crust | S. aureus impetigo | Both may coexist; bullae strongly favour staphylococcal exfoliative toxin |
| Non-purulent cellulitis | DVT, contact dermatitis, stasis dermatitis | Bilateral/recurrent sharply patterned erythema or absent fever/tenderness argues against bacterial cellulitis |
| Painful swollen limb | DVT, compartment syndrome, pyomyositis | Disproportionate pain and rapid systemic toxicity require urgent surgical exploration for NF |
| Cola urine after URTI | IgA nephropathy | IgA haematuria is synpharyngitic; PSGN has a latent interval and low C3 |
High Yield Summary
- Divide GAS disease into local, toxin-mediated, invasive, and post-infectious syndromes.
- Viral features make GAS pharyngitis less likely; clinical features alone cannot reliably confirm it.
- Scarlet fever is pharyngitis plus toxin-mediated sandpaper rash, Pastia lines, and strawberry tongue.
- Erysipelas is raised and sharply demarcated; cellulitis is deeper and poorly demarcated; NF causes disproportionate pain and rapid toxicity.
- ARF follows pharyngitis; PSGN follows pharyngitis or skin infection and presents after a latent interval.
Active Recall - GAS Clinical Disease
[1] Lecture slides: GC 105. Medically important microbes what every doctor should know.pdf [2] Lecture slides: GC 021. Upper respiratory tract infections.pdf (Centor/McIsaac and test-before-treatment framing) [3] CDC: Clinical Guidance for Group A Streptococcal Pharyngitis and Scarlet Fever (updated 2025–2026) [4] Lecture slides: CFB (MED09) Dermatology (II).pdf (necrotising fasciitis recognition and urgency) [5] Existing MBBSPedia: It is red and painful — lecture notes (impetigo, erysipelas, cellulitis, and type II NF)
Diagnosis: Match the Specimen to the Syndrome
A positive result answers different questions in different settings. A throat test detects current pharyngeal GAS, a sterile-site culture proves invasive disease, and antibody titres document a recent immune response rather than active infection.
Swab both tonsillar pillars and posterior pharynx while avoiding tongue, cheeks, and saliva. Sampling before antibiotics improves culture yield.
| Test | Detects | Turnaround | Interpretation |
|---|---|---|---|
| Rapid antigen detection test (RADT) | Group A carbohydrate antigen | Minutes | High specificity; a positive result supports treatment. Sensitivity is imperfect. |
| Throat culture on blood agar | Viable β-haemolytic GAS | Usually 24–48 hours | Reference method; permits identification. In symptomatic children, a negative RADT is commonly backed up by culture. |
| NAAT/PCR | GAS nucleic acid | Rapid to same day | Highly sensitive; may detect low-level carriage, so interpret with compatible symptoms. |
Do not test when overt viral features dominate. Conversely, examination alone cannot reliably separate GAS from viral pharyngitis when viral features are absent. Asymptomatic carriage means a positive test can coexist with a viral sore throat; the clinical syndrome still matters. [2]
Routine non-purulent cellulitis is often a clinical diagnosis because superficial swabs poorly represent deep dermal organisms. Culture becomes more useful with pus, open wounds, unusual exposures, recurrence, immunocompromise, treatment failure, or severe/invasive disease.
For suspected necrotising fasciitis:
- Obtain blood cultures if this does not delay treatment.
- Surgical exploration is both diagnostic and therapeutic.
- Send deep tissue/fascial specimens, aspirate, and blood for Gram stain, aerobic/anaerobic culture, identification, and susceptibility.
- Superficial wound swabs can mislead through colonising organisms.
- Imaging may show fascial oedema, fluid, or gas, but a normal scan does not exclude early NF and imaging must not delay surgery in a high-probability case.
| Step | GAS finding | Biological basis |
|---|---|---|
| Gram stain | Gram-positive cocci in chains/pairs | Thick peptidoglycan retains crystal violet; one-plane division creates chains. |
| Blood agar | Small translucent colonies with a wide clear β-haemolytic zone | Streptolysins completely lyse surrounding RBCs. |
| Catalase | Negative | GAS lacks catalase; no bubbling with hydrogen peroxide. |
| Lancefield grouping | Group A carbohydrate detected | Cell-wall polysaccharide defines the serogroup. |
| PYR | Positive | GAS hydrolyses pyrrolidonyl-β-naphthylamide. |
| Bacitracin | Classically susceptible | Useful presumptive teaching test, but not sufficiently specific for definitive modern identification. |
| MALDI-TOF/NAAT | Species-specific protein or nucleic-acid profile | Rapid contemporary confirmation. |
| Susceptibility | β-lactam susceptible; macrolide/clindamycin resistance varies | Penicillin remains predictably active; alternatives require local susceptibility awareness. |
There is no single confirmatory GAS test for ARF. Diagnose with the revised Jones framework, population-risk thresholds, and evidence of preceding GAS infection:
- Major manifestations: carditis (including subclinical echocardiographic carditis), arthritis pattern according to risk group, chorea, erythema marginatum, subcutaneous nodules.
- Minor manifestations: fever, arthralgia, inflammatory markers, and prolonged PR interval, with risk-group-specific thresholds.
- Evidence of preceding infection: rising/elevated streptococcal antibody titre, positive throat culture/RADT, or recent scarlet fever.
Sydenham chorea or indolent carditis may present so late that streptococcal titres have fallen; apply specialist criteria rather than mechanically rejecting the diagnosis.
| Domain | Expected finding | Why |
|---|---|---|
| Urine | Haematuria, dysmorphic RBCs/RBC casts, variable proteinuria | Inflamed glomerular barrier leaks RBCs and protein. |
| Renal function | Raised creatinine/urea, oliguria | Endocapillary proliferation lowers GFR. |
| Volume | Oedema, hypertension | Salt/water retention accompanies reduced filtration. |
| Complement | Low C3, often normal C4; C3 should recover within about 6–8 weeks | Alternative-pathway-predominant complement consumption supports PSGN. |
| Streptococcal evidence | ASO and/or anti-DNase B | Documents the antecedent immune response after the original infection has resolved. |
ASO versus anti-DNase B
ASO is usually stronger after pharyngeal infection and may be weak after impetigo. Anti-DNase B rises after both sites and is especially useful after skin infection. A rising paired titre is more persuasive than an isolated value because background titres vary by age and population. Neither test proves viable GAS remains present.
Renal biopsy is usually unnecessary in a typical recovering child. Consider it or broaden the differential for rapidly progressive renal failure, nephrotic-range proteinuria, absent streptococcal evidence, low C4, or C3 that remains low beyond the expected recovery window.
- Treating Centor as a culture: it estimates pre-test probability; it does not identify the organism.
- Using a throat culture to prove ARF/PSGN: the initiating infection may have resolved; serology is often more useful.
- Ordering ASO alone after impetigo: add anti-DNase B.
- Trusting a superficial swab in NF: obtain deep operative tissue.
- Letting imaging delay exploration: NF is a clinical-surgical emergency.
- Calling bacitracin definitive: use validated modern identification.
High Yield Summary
- Match test to compartment: throat antigen/NAAT/culture for pharyngitis, deep tissue and blood cultures for invasive disease, serology for delayed sequelae.
- RADT is specific but less sensitive than culture; back-up strategy depends on age and guideline.
- GAS is β-haemolytic, catalase negative, group A antigen positive, and PYR positive.
- ASO supports recent pharyngeal GAS; anti-DNase B is more useful after skin infection.
- PSGN typically has nephritic urine and low C3; ARF requires Jones-based clinical synthesis plus antecedent GAS evidence.
Active Recall - GAS Diagnosis
[1] Lecture slides: GC 021. Upper respiratory tract infections.pdf (test-directed pharyngitis diagnosis) [2] CDC: Clinical Guidance for Group A Streptococcal Pharyngitis (updated November 2025) [3] Existing MBBSPedia: Diagnosis of infections — lecture notes (culture, antigen, nucleic-acid, and serological principles) [4] Existing MBBSPedia: Post-streptococcal glomerulonephritis — Diagnosis (ASO/anti-DNase B and complement interpretation) [5] CDC: Diagnosing Acute Rheumatic Fever and Clinical Guidelines for PSGN (accessed July 2026)
Treatment and Prevention: Eradicate Local Disease, Operate on Deep Disease
| Syndrome | Core approach | Why |
|---|---|---|
| Confirmed pharyngitis/scarlet fever | Penicillin V or amoxicillin; use a guideline-supported alternative for true allergy | GAS remains β-lactam susceptible; eradication shortens illness/transmission and prevents ARF. |
| Localised impetigo | Local wound/skin care plus topical therapy when appropriate; oral therapy if extensive | Therapy must cover GAS and often S. aureus. |
| Erysipelas/non-purulent cellulitis | A β-lactam active against streptococci; choose route by severity | Diffuse non-purulent disease is commonly streptococcal; drainage is needed if a collection is present. |
| Necrotising fasciitis | Immediate broad empirical IV antibiotics + urgent exploration/debridement; when GAS confirmed, penicillin plus clindamycin | Surgery removes devitalised tissue; penicillin kills GAS and clindamycin suppresses protein/toxin synthesis. |
| STSS | ICU resuscitation, penicillin + clindamycin, and source control | Antibiotics alone cannot reverse toxin-driven shock or remove an infected deep focus. |
| PSGN | Support volume, BP, electrolytes and renal function; eradicate residual GAS if present | Renal injury is immune-mediated, so antibiotics do not reverse established nephritis. |
| ARF | Eradicate GAS, treat inflammation/carditis, then secondary prophylaxis | Preventing recurrent pharyngeal GAS prevents cumulative immune-mediated valve damage. |
GC 098 teaches that confirmed GAS pharyngitis should receive the full 10-day penicillin course for primary ARF prevention, even when symptoms resolve after a few days. [1]
Penicillin binds penicillin-binding proteins and blocks transpeptidation of peptidoglycan. Growing GAS cannot maintain its thick cell wall and undergoes osmotic lysis. No clinical penicillin-resistant GAS has been established, but resistance to macrolides and clindamycin varies; allergy alternatives should follow local susceptibility and guidance. [3]
For uncomplicated pharyngitis, narrow-spectrum penicillin is preferred because it reliably treats GAS while exerting less collateral selection than broad-spectrum agents. Do not prescribe antibiotics for a negative test or overt viral pharyngitis.
Why combine clindamycin?
Clindamycin inhibits the 50S ribosomal subunit, reducing exotoxin and M-protein synthesis. Its activity is less dependent on rapid bacterial growth than a cell-wall agent, which is valuable in high-inoculum, stationary-phase infection. It is an adjunct, not a substitute for β-lactam killing or surgery. Confirm susceptibility because clindamycin resistance exists.
CFB Dermatology specifically frames NF treatment as immediate hospitalisation, surgical/ICU involvement, high-dose IV antibiotics, aggressive debridement, and supportive care; delay worsens mortality. [2]
Support includes haemodynamic resuscitation, early vasopressors when required, ventilation, renal support, coagulation management, glycaemic/electrolyte correction, and repeated source-control assessment. IVIG may be considered in severe STSS by specialists, but efficacy is not definitive and it must never delay surgery or antibiotics.
Treating confirmed GAS pharyngitis:
- Reduces symptoms modestly.
- Reduces transmission once effective therapy has been given.
- Reduces suppurative complications.
- Prevents most ARF when started promptly.
- Does not reliably prevent PSGN.
Patients should follow current school/work exclusion advice, cover coughs, avoid sharing utensils, and perform hand hygiene. Replace myths about “sterilising the household” with targeted testing/treatment of symptomatic contacts; routine prophylaxis for ordinary household pharyngitis exposure is not standard.
After ARF, recurrent GAS pharyngitis can trigger further immune attacks and cumulative valve injury. Long-term penicillin prophylaxis is therefore secondary prevention. Duration depends on carditis, residual valvular disease, age, time since the last attack, exposure risk, and local protocol; it is not a single duration for every patient.
Established PSGN is managed primarily by:
- Sodium/fluid restriction when overloaded.
- Diuretics and antihypertensive therapy as clinically indicated.
- Monitoring weight, BP, urine output, creatinine, potassium, and complement recovery.
- Dialysis for refractory fluid overload, severe hyperkalaemia/acidosis, or uraemic complications.
- Antibiotic eradication of any remaining GAS to limit spread, while explaining that this does not undo immune-complex renal injury.
Use standard precautions and syndrome-appropriate additional precautions. Pharyngeal GAS spreads by droplets/direct secretions; skin lesions should be covered and hand hygiene reinforced. Healthcare-associated puerperal or surgical clusters require infection-control and public-health investigation.
There is no licensed GAS vaccine in routine clinical use as of July 2026. M-protein diversity, potential cross-reactivity, and the need to cover globally diverse emm types complicate development. Prevention therefore relies on prompt diagnosis/treatment, wound care, hygiene, source control, and ARF secondary prophylaxis.
Treatment Guardrails
- For the in-house exam, Penicillin V is the expected treatment for confirmed GAS pharyngitis, matching the 2025 Fourth Summative option set. [4]
- In current practice, confirm pharyngitis when testing is indicated and use local allergy/resistance guidance rather than defaulting to a macrolide.
- For NF/STSS, “penicillin-sensitive” does not mean penicillin alone: add toxin-suppressing therapy and obtain urgent source control.
- Antibiotics prevent ARF after pharyngitis but do not reliably prevent PSGN.
High Yield Summary
- Penicillin or amoxicillin treats confirmed uncomplicated pharyngitis; complete the recommended course.
- Timely pharyngitis treatment prevents ARF, not PSGN.
- GAS NF/STSS requires immediate broad empirical coverage, surgery, ICU support, then penicillin plus clindamycin when confirmed.
- Clindamycin suppresses toxin/protein production; penicillin provides reliable bactericidal activity.
- ARF needs long-term secondary prophylaxis; PSGN needs supportive renal/volume management.
Active Recall - GAS Treatment and Prevention
[1] Lecture slides: GC 098. Antibiotic prophylaxis.pdf (primary and secondary ARF prevention) [2] Lecture slides: CFB (MED09) Dermatology (II).pdf (urgent NF antibiotics, surgery, and supportive care) [3] CDC: Clinical Guidance for GAS Pharyngitis, Type II Necrotizing Fasciitis, and STSS (updated 2025) [4] Past papers: 2025 Fourth Summative MCQ.pdf, Question 20 (Penicillin V for GAS pharyngitis) [5] Existing MBBSPedia: Practical issues in antibiotic use — lecture notes
Complications and Exam Links
| Complication | Mechanism | Red flag |
|---|---|---|
| Peritonsillar/retropharyngeal abscess | Local extension from pharynx into deep neck spaces | Trismus, “hot-potato” voice, uvular deviation, drooling, torticollis, stridor |
| Cervical lymphadenitis/otitis/sinusitis | Contiguous mucosal spread | Focal pain/swelling or persistent fever after apparent pharyngitis |
| Bacteraemia/puerperal sepsis | Mucosal or uterine invasion with bloodstream spread | Hypotension, lactate rise, organ dysfunction |
| Necrotising fasciitis/myositis | Enzymes, cytolysins, proteases, microvascular thrombosis | Pain out of proportion, rapid progression, bullae, dusky skin, later anaesthesia |
| STSS | Superantigen cytokine storm during invasive infection | Shock plus renal, hepatic, pulmonary, coagulation, or soft-tissue failure |
ARF follows GAS pharyngitis, not impetigo. Antibodies and T cells primed against streptococcal antigens cross-react with cardiac, synovial, and neural targets.
JONES manifestations
| Hook | Manifestation | Clinical meaning |
|---|---|---|
| J | Migratory large-joint polyarthritis | Fleeting inflammation moves between knees, ankles, elbows, and wrists. |
| O | Carditis | Can involve pericardium, myocardium, and endocardium; valvulitis, especially mitral regurgitation, drives chronic morbidity. |
| N | Subcutaneous nodules | Firm, painless nodules over extensor surfaces; uncommon and associated with carditis. |
| E | Erythema marginatum | Evanescent, non-pruritic annular rash on trunk/proximal limbs, usually sparing the face. |
| S | Sydenham chorea | Delayed purposeless movements, emotional lability, hypotonia, and motor impersistence. |
JONES is a memory aid for major manifestations, not the complete diagnostic rule. The revised criteria also require the appropriate major/minor combination, evidence of preceding GAS, and population-risk adjustments.
PSGN can follow pharyngitis or impetigo. Nephritogenic antigens such as SpeB/NAPlr become planted or form circulating immune complexes; complement activation recruits neutrophils and produces diffuse proliferative glomerular injury.
| Consequence | Mechanism |
|---|---|
| Cola/tea urine and RBC casts | RBCs cross the inflamed glomerular barrier and oxidise during tubular transit. |
| Oedema and hypertension | Reduced GFR causes sodium/water retention. |
| Oliguria/AKI | Endocapillary proliferation and inflammation narrow capillary lumina. |
| Low C3 | Complement is consumed during immune-complex injury. |
| Subepithelial “humps” | Electron-dense immune deposits accumulate on the epithelial side of GBM. |
GC 057 emphasises children aged roughly 2–10 years and the sequence “streptococcal antigens planted in the glomerulus → host immune response 10–14 days later.” [2]
| Exam discriminator | ARF | PSGN |
|---|---|---|
| Trigger | Pharyngitis | Pharyngitis or skin infection |
| Immune mechanism | Molecular mimicry/cross-reactivity | Immune complex and complement injury |
| Key organ | Heart/joints/CNS/skin | Kidney |
| Evidence | Jones framework + antecedent GAS | Nephritic syndrome + low C3 + antecedent GAS |
| Antibiotic prevention | Yes, if pharyngitis treated promptly | Not reliably |
| Recurrence prevention | Long-term penicillin after ARF | No routine long-term antibiotic prophylaxis |
| Retrieved source | Point taught | Likely exam hook |
|---|---|---|
| GC 105 microbiology | GAS spans pharyngitis, scarlet fever, skin infection, NF/STSS, ARF, and PSGN. [1] | Classify a vignette as local, toxin, invasive, or post-infectious disease. |
| GC 098 antibiotic prophylaxis | GAS pharyngitis is microbiologically diagnosed; full-course treatment prevents ARF; distinguish primary from secondary prevention. [3] | “Why treat?” and duration/prophylaxis reasoning. |
| GC 057 nephrology | PSGN follows planted antigen with delayed host response and presents as nephritic syndrome. [2] | Latency, low C3, cola urine, and IgA nephropathy discrimination. |
| CFB Dermatology II | NF requires immediate antibiotics, debridement, ICU/surgical care; delay worsens outcome. [4] | Pain out of proportion → act before late skin signs. |
| 2025 Fourth Summative MCQ Q20 | Penicillin V appears as the most suitable treatment for GAS pharyngitis. [5] | Choose the narrow β-lactam, not a broad agent. |
Integrated Vignettes
A teenager develops fever and exudative pharyngitis, then three weeks later has migratory knee/ankle arthritis and a new apical pansystolic murmur. Think ARF: obtain evidence of antecedent GAS, ECG/inflammatory markers, and echocardiography; apply revised Jones criteria. Eradicate GAS, treat inflammation/carditis, and plan secondary prophylaxis.
A child develops periorbital oedema, hypertension, oliguria, and brown urine three weeks after honey-crusted lesions. Think PSGN, not ARF. Look for RBC casts, renal impairment, low C3, and anti-DNase B. Treat volume/BP/renal complications; antibiotics do not reverse established immune injury.
An otherwise healthy adult develops escalating limb pain, little initial erythema, then swelling, bullae, hypotension, and AKI. Think GAS NF with STSS. Call surgery/ICU, give broad empirical antibiotics, obtain deep specimens at immediate exploration, and use penicillin plus clindamycin when GAS is confirmed.
- ARF after impetigo — classic ARF follows pharyngitis.
- Assuming all JONES letters are enough — apply full revised criteria and antecedent GAS evidence.
- Saying antibiotics prevent PSGN — they do not reliably do so.
- Waiting for gas on imaging in NF — GAS NF may have no gas.
- Treating shock without source control — STSS often has a surgically removable focus.
- Using ASO alone after skin infection — anti-DNase B is more sensitive.
High Yield Summary
- GAS complications divide into suppurative spread, invasive toxin disease, ARF, and PSGN.
- ARF is molecular-mimicry disease after pharyngitis; carditis can cause chronic mitral valve disease.
- PSGN is immune-complex/complement disease after throat or skin infection; expect cola urine, nephritic syndrome, and low C3.
- NF/STSS is time-critical: disproportionate pain and shock demand immediate surgery, antibiotics, and ICU support.
- The 2025 local paper directly tested Penicillin V for GAS pharyngitis.
Active Recall - GAS Complications and Exam Links
[1] Lecture slides: GC 105. Medically important microbes what every doctor should know.pdf [2] Lecture slides: GC 057. Glomerular and Tubulo-interstitial Diseases and Acute Kidney Injury.pdf [3] Lecture slides: GC 098. Antibiotic prophylaxis.pdf [4] Lecture slides: CFB (MED09) Dermatology (II).pdf [5] Past papers: 2025 Fourth Summative MCQ.pdf, Question 20 [6] CDC: Clinical Guidance for Acute Rheumatic Fever and PSGN (accessed July 2026)
Streptococcus pyogenes: Integrated Revision Summary
| Domain | Must know |
|---|---|
| Identity | Group A, β-haemolytic, catalase-negative Gram-positive coccus in chains |
| Reservoir/transmission | Human pharynx and skin; respiratory secretions or direct contact |
| Immune evasion | M protein + host-like hyaluronic-acid capsule |
| Tissue spread | Streptokinase, DNases, SpeB, streptolysins |
| Toxin disease | Pyrogenic exotoxin superantigens → scarlet fever and STSS |
| Bench tests | Group A antigen, PYR positive, classically bacitracin susceptible |
| Drug anchor | GAS remains penicillin susceptible; macrolide/clindamycin resistance varies |
| Organism | Morphology/haemolysis | Key test | High-yield disease |
|---|---|---|---|
| S. pyogenes | Chains, β | PYR positive, group A | Pharyngitis, skin disease, NF/STSS, ARF, PSGN |
| S. agalactiae | Chains, β | CAMP/hippurate positive, group B | Neonatal/peripartum infection |
| S. pneumoniae | Lancet diplococci, α | Optochin susceptible, bile soluble | Pneumonia, meningitis, otitis |
| Viridans streptococci | Chains, α | Optochin resistant | Caries, subacute endocarditis |
| S. aureus | Clusters, often β | Catalase/coagulase positive | Purulent abscess and toxin disease |
| Syndrome | Recognition | Key action |
|---|---|---|
| Pharyngitis | Abrupt sore throat, fever, exudate, tender anterior nodes; cough/coryza favour virus | Test when indicated; treat confirmed GAS |
| Scarlet fever | Sandpaper rash, Pastia lines, strawberry tongue with GAS infection | Confirm and treat as GAS |
| Impetigo | Honey-coloured crust | Cover GAS and often S. aureus |
| Erysipelas/cellulitis | Sharp raised edge versus diffuse deep erythema | Streptococcal-active β-lactam; drain collections |
| NF/STSS | Disproportionate pain, rapid spread, bullae, shock/organ failure | Immediate surgery + broad antibiotics + ICU |
| ARF | Migratory arthritis, carditis, chorea, nodules, erythema marginatum | Jones synthesis, eradicate GAS, secondary prophylaxis |
| PSGN | Cola urine, oedema, hypertension, oliguria after throat/skin infection | Nephritic work-up, supportive renal care |
| Feature | ARF | PSGN |
|---|---|---|
| Trigger | Pharyngitis only | Pharyngitis or skin infection |
| Mechanism | Molecular mimicry | Immune complexes/complement |
| Marker | Jones criteria + antecedent GAS | RBC casts, low C3, ASO/anti-DNase B |
| Prevention by treating pharyngitis | Yes | Not reliably |
| Long-term prophylaxis | Required after ARF | Not routine |
GC 105: one β-haemolytic organism links pharyngitis, scarlet fever, impetigo/cellulitis, NF/STSS, ARF, and PSGN. [1]
GC 098: confirmed GAS pharyngitis requires the full penicillin course to prevent ARF; distinguish primary treatment from secondary rheumatic-fever prophylaxis. [2]
2025 Fourth Summative MCQ Question 20 directly maps GAS pharyngitis to Penicillin V. [3]
- ASO is strongest after pharyngitis; anti-DNase B is especially useful after skin infection.
- ARF follows pharyngitis; PSGN follows throat or skin infection.
- Clindamycin is added in severe invasive disease to suppress toxin synthesis.
- NF is a surgical diagnosis: imaging must not delay debridement.
- Bacitracin susceptibility is a classic discriminator, not the sole modern identification method.
- Gram-positive cocci in chains; catalase negative
- Group A, β-haemolytic, PYR positive
- M protein + hyaluronic-acid capsule
- Streptolysin O/S, streptokinase, DNase, SpeB
- Pyrogenic exotoxin = superantigen
- Pharyngitis, scarlet fever, impetigo, erysipelas, cellulitis
- Pain out of proportion = NF until proven otherwise
- Penicillin + clindamycin + surgery for confirmed GAS NF/STSS
- JONES manifestations and mitral valvulitis
- PSGN: cola urine, low C3, ASO/anti-DNase B
- Antibiotics prevent ARF, not PSGN
High Yield Summary
Think group A β-haemolytic chains + M protein/capsule + four disease modes: local infection, exotoxin disease, invasive tissue destruction, and delayed immune sequelae. Confirm pharyngitis before narrow penicillin therapy, never delay surgery in NF, add clindamycin for toxin suppression in severe invasive GAS, and distinguish ARF from PSGN by trigger, mechanism, timing, and prevention.
Active Recall - Streptococcus pyogenes
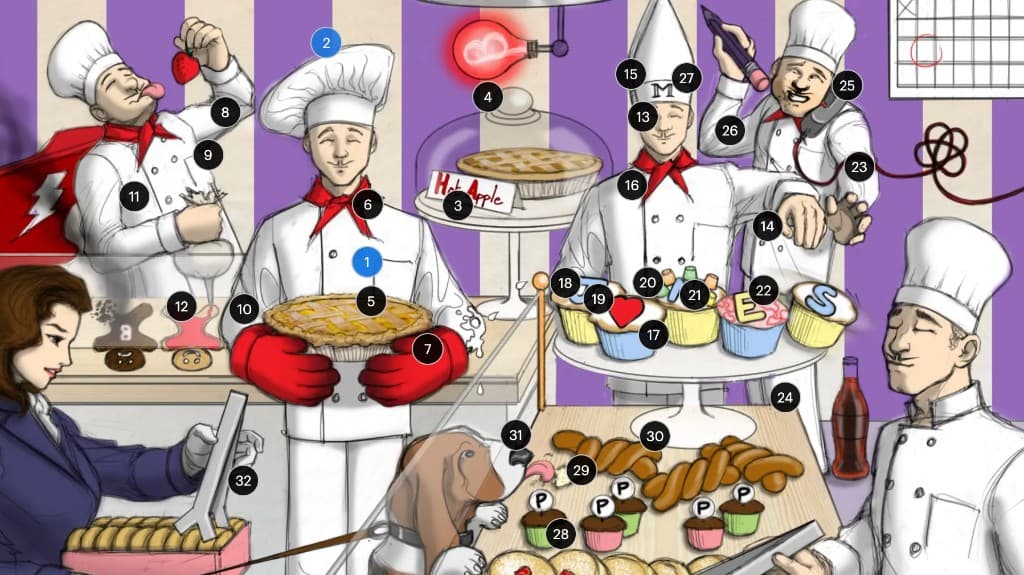
Sketchy Micro hooks for Streptococcus pyogenes (group A Streptococcus)
How to Use This Sketchy
The 32 supplied labels are grouped by the clinical sequence identity → local/toxin disease → virulence → rheumatic fever → PSGN → laboratory diagnosis. The Note concept column is the medically reconciled source of truth; the supplied Sketchy meaning remains the recall hook.
Important Guardrails
- The image’s bacitracin clue is a classic presumptive discriminator; modern laboratories confirm GAS with validated antigen, MALDI-TOF, or molecular methods.
- Rheumatic fever classically follows pharyngitis, whereas PSGN can follow pharyngitis or skin infection.
- Treating confirmed pharyngitis prevents most acute rheumatic fever but does not reliably prevent PSGN.
- In confirmed GAS necrotising fasciitis/STSS, penicillin susceptibility does not remove the need for urgent surgery and adjunctive toxin-suppressing therapy.
- JONES is a memory aid for major manifestations, not the entire revised diagnostic criteria.
| No. | Visible symbol | Sketchy meaning | Note concept | Why the association works | Lecture / exam link |
|---|---|---|---|---|---|
| 1 | Pie bakers | Streptococcus pyogenes (group A strep), a Gram-positive coccus | GAS is a group A, β-haemolytic, catalase-negative Gram-positive coccus in chains. | “Pie-genies” cues pyogenes; multiple bakers cue chained cocci. | GC 105 classifies GAS among β-haemolytic streptococci. |
| 2 | Purple stripes | S. pyogenes is a Gram-positive coccus | A thick peptidoglycan wall retains purple crystal violet on Gram stain. | Purple is the conventional Gram-positive colour; round markings cue cocci. | Distinguish from Gram-negative diplococci and Gram-positive rods. |
| 3 | “Hot Apple” pie beside a glass capsule | Hyaluronic-acid capsule helps evade host immunity | The host-like hyaluronic-acid capsule is poorly immunogenic and anti-phagocytic. | “Hot apple” approximates hyaluronate; glass encasement makes the capsule visible. | Capsule and M protein cooperate in opsonophagocytic evasion. |
| 4 | Glowing beta light bulb | Complete β-haemolysis on blood agar | Streptolysins produce a clear zone of complete RBC lysis around colonies. | The β-shaped light “clears” its surroundings. | GC 050/105 use haemolysis as the first streptococcal classification step. |
| No. | Visible symbol | Sketchy meaning | Note concept | Why the association works | Lecture / exam link |
|---|---|---|---|---|---|
| 5 | Flaky pie crust | Impetigo with honey-crusted lesions | GAS can cause non-bullous impetigo, typically superficial perioral/perinasal honey-coloured crusts. | Flaking golden crust resembles impetigo’s dried exudate. | Differentiate non-bullous GAS/S. aureus disease from bullous staphylococcal impetigo. |
| 6 | Red neckerchief on the pie chef | Streptococcal pharyngitis | GAS is the principal bacterial cause of acute pharyngitis; abrupt fever/sore throat with no viral features prompts microbiological testing. | Red cloth at the neck localises inflammation to the pharynx. | GC 021: clinical features alone do not confirm GAS; test when indicated. |
| 7 | Large red puffy gloves | GAS skin infections including cellulitis, erysipelas, impetigo, and NF | GAS causes superficial, dermal, and rapidly invasive soft-tissue infection. | Puffy red gloves mimic swollen erythematous skin and deeper tissue oedema. | Pain out of proportion and rapid progression signal NF. |
| 8 | Chef licking a strawberry | Scarlet fever with strawberry tongue | Scarlet fever causes a white then red strawberry tongue with pharyngitis. | The literal strawberry places the clue at the tongue. | CFB paediatrics sample: sore throat + sandpaper rash = scarlet fever. |
| 9 | Red neckerchief on the cookie chef | Scarlet fever includes pharyngitis | Scarlet fever is GAS infection, usually pharyngitis, plus a pyrogenic-exotoxin rash. | Repeated red throat marker links the rash syndrome to pharyngeal GAS. | Do not diagnose scarlet fever from rash alone; confirm GAS. |
| 10 | Red frosting on the body but not hands or feet | Desquamative sandpaper rash that usually spares palms and soles | A fine blanching scarlatiniform rash starts on trunk/flexures, feels like sandpaper, and later desquamates. | Red coating depicts diffuse rash; bare extremities cue relative palm/sole sparing. | Pastia lines and strawberry tongue strengthen the diagnosis. |
| No. | Visible symbol | Sketchy meaning | Note concept | Why the association works | Lecture / exam link |
|---|---|---|---|---|---|
| 11 | Superhero cape with a lightning bolt | Pyrogenic exotoxins are superantigens associated with TSS | Spe toxins activate many T cells outside normal peptide specificity, causing cytokine-driven shock and organ failure. | “Super” hero cues superantigen; lightning depicts abrupt shock. | GC 105 lists GAS toxic shock; severe disease needs ICU and source control. |
| 12 | Letter “B” beside a black necrotic cookie | SpeB contributes to necrotising fasciitis | SpeB, a cysteine protease, degrades host matrix/immune proteins and contributes to invasive tissue destruction. | B labels SpeB; the black cookie depicts necrosis. | CFB Dermatology: do not delay debridement in NF. |
| 13 | Letter “M” on the chef’s hat | M protein is a major surface virulence factor | emm-encoded M protein promotes adherence and resists complement-mediated opsonisation. | The surface hat label makes M protein prominent on the bacterial “character.” | M type also provides epidemiological/strain classification. |
| 14 | Hand blocking food from a mouth | M protein resists phagocytosis | M protein limits effective complement deposition and phagocytic uptake. | The blocked eating action visualises inhibition of “cell eating.” | Mechanism question: anti-phagocytic M protein + capsule. |
| 15 | Mitre-shaped chef’s hat | M protein resembles host tissue → rheumatic heart disease, especially mitral valve | Cross-reactive immunity after GAS pharyngitis targets cardiac tissue; chronic disease often prominently affects the mitral valve. | Mitre sounds like mitral; shared “M” links M protein and molecular mimicry. | ARF is immune-mediated, not active bacterial invasion of valves. |
| No. | Visible symbol | Sketchy meaning | Note concept | Why the association works | Lecture / exam link |
|---|---|---|---|---|---|
| 16 | Red neckerchief on the master chef | Untreated GAS pharyngitis can precede rheumatic fever | ARF follows pharyngeal GAS after a latent immune response; prompt treatment prevents most attacks. | The red throat on the senior chef marks the antecedent infection. | GC 098: confirmed pharyngitis treatment is primary ARF prevention. |
| 17 | Five cupcakes spelling “JONES” | JONES major manifestations | Joints, carditis, subcutaneous nodules, erythema marginatum, and Sydenham chorea are major ARF manifestations. | The five letters provide the standard mnemonic. | Use revised Jones criteria, risk thresholds, minor criteria, and antecedent GAS evidence. |
| 18 | “J” cupcake with elbow frosting | Migratory large-joint polyarthritis | ARF typically causes fleeting, migratory inflammation of large joints such as knees, ankles, elbows, and wrists. | J = joints; frosting on the elbow localises large-joint inflammation. | Contrast with persistent/non-migratory post-streptococcal reactive arthritis. |
| 19 | Heart symbol on a cupcake | Pancarditis, especially valvulitis | ARF may affect pericardium, myocardium, and endocardium; mitral valvulitis is the key chronic-disease pathway. | The heart icon directly cues carditis. | Echocardiography detects clinical or subclinical carditis. |
| 20 | “N” cupcake topped by nodular candies | Subcutaneous nodules | Firm painless nodules occur on extensor surfaces and are strongly associated with carditis. | N = nodules; small candy lumps depict palpable nodules. | Nodules are uncommon, so their presence is diagnostically weighty. |
| 21 | “E” cupcake with a ring pattern | Erythema marginatum | Evanescent, non-pruritic annular/serpiginous rash affects trunk and proximal limbs. | Ringed margin depicts the expanding erythematous edge. | Usually spares the face; distinguish from scarlet fever’s sandpaper rash. |
| 22 | “S” cupcake falling sideways | Sydenham chorea | Delayed purposeless movements, motor impersistence, emotional lability, and hypotonia reflect post-streptococcal basal-ganglia autoimmunity. | The unstable falling cupcake mimics involuntary, poorly controlled movement. | Chorea may appear months later when streptococcal titres have declined. |
| No. | Visible symbol | Sketchy meaning | Note concept | Why the association works | Lecture / exam link |
|---|---|---|---|---|---|
| 23 | Black knot in a cord beside the arm | Immune complexes deposit in glomeruli causing nephritic syndrome | Nephritogenic antigens/immune complexes activate complement, causing glomerular inflammation, haematuria, oedema, hypertension, and oliguria. | The tangled knot resembles a glomerular capillary tuft obstructed by immune deposits. | GC 057: planted antigen → host response 10–14 days later. |
| 24 | Cola bottle | Gross haematuria appears tea/cola/rust coloured | Glomerular RBCs oxidise during nephron transit, producing smoky brown urine rather than bright lower-tract bleeding. | Cola directly matches the classic urine description. | Check RBC casts, creatinine, BP, and volume status. |
| 25 | Calendar with a later date circled | PSGN appears weeks after acute streptococcal infection | PSGN is delayed: about 1–3 weeks after pharyngitis and often 3–6 weeks after skin infection. | The later calendar circle encodes the latent immune interval. | Contrast synpharyngitic IgA nephropathy. |
| 26 | Cookie crumbs on the face plus a red neckerchief | Pharyngitis and skin infection can both precede PSGN | PSGN follows nephritogenic GAS infection at either the pharynx or skin. | Face crumbs cue impetigo; red neckerchief cues pharyngitis. | ARF classically follows pharyngitis, not impetigo. |
| 27 | Purple pencil | Penicillin reduces ARF risk, but PSGN may still occur despite appropriate treatment | Treating confirmed pharyngitis prevents most ARF but does not reliably prevent PSGN after throat or skin infection. | Pencil cues penicillin; its placement beside both pathways highlights unequal prevention. | 2025 Fourth Summative Q20: Penicillin V for GAS pharyngitis. |
| No. | Visible symbol | Sketchy meaning | Note concept | Why the association works | Lecture / exam link |
|---|---|---|---|---|---|
| 28 | Broken “O” doughnuts | Streptolysin O lyses RBCs and immune cells | Oxygen-labile streptolysin O forms membrane pores, injures host cells, and elicits the ASO antibody response. | Broken O-shaped doughnuts depict lysis by the O toxin. | ASO supports recent pharyngeal GAS but may be weak after skin infection. |
| 29 | Cupcakes marked “P” | Streptokinase converts plasminogen to plasmin and degrades fibrin | Streptokinase activates plasmin, dissolving fibrin barriers and promoting tissue spread. | P labels plasmin/plasminogen; scattered pastries suggest spread. | Pair with DNase and SpeB in an invasive-disease mechanism answer. |
| 30 | Twisted strands above the pastries | DNases degrade host DNA | GAS DNases digest DNA in pus and neutrophil extracellular traps, reducing viscosity and aiding escape. | Twisted strands resemble DNA being pulled apart. | Anti-DNase B is especially useful after skin infection. |
| 31 | Basset hound licking pastries | Bacitracin susceptibility and PYR positivity distinguish GAS from GBS | GAS is classically bacitracin susceptible and PYR positive; GBS is bacitracin resistant and PYR negative. | “Basset” cues bacitracin; licking/eating cues a positive biochemical reaction. | Presumptive teaching tests only; modern labs confirm species. |
| 32 | “O” doughnuts held by antibody-shaped tongs | ASO helps diagnose post-pharyngeal sequelae; anti-DNase B improves sensitivity after skin infection | Antistreptolysin O documents recent pharyngeal GAS; anti-DNase B rises after throat and skin infection and is preferred after impetigo. | Tongs shaped like antibodies grasp the O antigen, depicting anti-streptolysin O. | Serology documents antecedent infection; it does not diagnose active pharyngitis. |
High Yield Summary
Read the bakery as one causal story: group A β-haemolytic purple cocci use capsule and M protein to evade phagocytosis → cause throat and skin disease → release superantigen/protease toxins in scarlet fever, STSS, and NF → trigger ARF after pharyngitis or PSGN after throat/skin infection → remain penicillin susceptible while ASO/anti-DNase B document delayed sequelae.