Neisseria meningitidis
A clinically integrated guide to meningococcal biology, invasive disease, diagnosis, treatment, prevention, and Sketchy recall.
Foundations: From Diplococcus to Invasive Disease
| Property | Neisseria meningitidis | Why it matters clinically |
|---|---|---|
| Common name | Meningococcus | “Meningo-” flags its classic meningeal tropism, but bloodstream disease may be even more fulminant. |
| Gram stain | Gram-negative diplococci, often kidney-bean shaped and intracellular in neutrophils | A compatible sterile-site smear can give a rapid presumptive diagnosis while culture or PCR is pending. |
| Metabolism | Aerobic/facultatively anaerobic, oxidase positive; ferments glucose and maltose | Maltose fermentation classically separates meningococcus from N. gonorrhoeae, which ferments glucose but not maltose. |
| Reservoir | Humans only, especially the nasopharynx | Carriage sustains transmission; there is no animal reservoir to control. |
| Transmission | Close exposure to respiratory or throat secretions | Household crowding, dormitories, military barracks, intimate kissing, and direct airway secretion exposure increase risk. |
| Major syndromes | Meningitis and meningococcaemia/septicaemia | Either can occur alone or together; shock may evolve before meningism becomes obvious. |
| Capsule | Polysaccharide capsule; important serogroups include A, B, C, W, X, and Y | The capsule resists opsonophagocytosis and determines vaccine strategy. |
GC lecture classification anchor: place meningococcus under Gram-negative cocci, then under Neisseria; connect organism → disease → treatment rather than memorising an isolated name. [1]
The logic is sequential:
- Gram-negative means a thin peptidoglycan layer plus an outer membrane. Alcohol disrupts that outer membrane during staining, so crystal violet is lost and the organism takes up the pink counterstain.
- Coccus describes a spherical cell. Division in one plane with paired cells produces the characteristic diplococcus.
- Oxidase positivity reflects cytochrome-c oxidase in the respiratory chain.
- Maltose fermentation is a classic bench discriminator: meningococcus uses both glucose and maltose, whereas gonococcus classically uses glucose alone.
Most acquisition produces asymptomatic nasopharyngeal carriage, not invasive disease. Disease requires a sequence of biological hurdles:
| Virulence factor | First-principles action | Clinical consequence |
|---|---|---|
| Type IV pili | Initial attachment to nasopharyngeal epithelium; undergo antigenic and phase variation | Promotes carriage while helping the organism evade pre-existing antibodies. |
| IgA protease | Cleaves secretory IgA at the mucosal surface | Weakens immune exclusion and facilitates persistence at the portal of entry. |
| Opa/Opc adhesins | Strengthen intimate epithelial and endothelial interaction after pili establish contact | Help traversal across epithelial and vascular barriers. |
| Polysaccharide capsule | Masks the bacterial surface and impairs complement-dependent opsonisation and phagocytosis | Enables survival in blood; explains severe risk in asplenia and complement deficiency. |
| Factor H-binding protein | Recruits human factor H, which restrains the alternative complement pathway | Reduces complement deposition; also provides an antigen used in protein-based MenB vaccines. |
| Lipooligosaccharide (LOS) | TLR4-active endotoxin lacking the long O-antigen side chain of classic LPS | Drives cytokine release, endothelial injury, capillary leak, tissue-factor activation, DIC, and shock. |
| LOS-rich outer-membrane vesicles/blebs | Shed inflammatory membrane material into the circulation | A small bacterial burden can deliver a disproportionately large systemic endotoxin signal. |
| Iron-acquisition proteins | Extract iron from human transferrin and lactoferrin | Supports growth in an iron-restricted human host and reinforces human specificity. |
The capsule is an anti-phagocytic shield. Antibody bound to capsule normally activates complement and promotes opsonisation; without effective antibody-complement cooperation, circulating meningococci can multiply rapidly.
Serogroups are defined by capsular chemistry. Serogroup B capsule resembles polysialic-acid structures found on human neural-cell adhesion molecules, so it is poorly immunogenic and raises concern for immune tolerance. Consequently:
- MenACWY vaccines can target capsular polysaccharides conjugated to a carrier protein.
- MenB vaccines instead use recombinant surface proteins/outer-membrane antigens, not serogroup-B capsular polysaccharide.
Why Complement and the Spleen Matter
C5b, C6, C7, C8, and C9 assemble the membrane attack complex (MAC), which inserts pores into Gram-negative outer membranes. Terminal complement deficiency therefore produces a striking, relatively specific susceptibility to recurrent invasive Neisseria infection. Recurrent meningococcal disease should trigger complement-pathway evaluation with CH50/AH50 and specialist assessment.
The spleen filters blood and coordinates antibody-mediated clearance of encapsulated organisms. Without a functioning spleen, a capsule-shielded meningococcus may remain poorly opsonised and multiply explosively. The GC microbiology material explicitly links meningococcus with post-splenectomy sepsis risk. [1]
LOS is not simply “toxic”; it activates innate immunity:
- LOS binds LPS-binding protein and CD14/TLR4 on monocytes and endothelium.
- NF-κB signalling releases TNF-α, IL-1, IL-6, and other mediators.
- Endothelium becomes activated and leaky; nitric oxide lowers vascular tone.
- Tissue factor activates coagulation while natural anticoagulant pathways, including protein C, are impaired.
- Microvascular thrombi consume platelets and clotting factors.
- The patient simultaneously develops ischaemia from thrombosis and bleeding from consumptive coagulopathy.
- Capillary leak plus vasodilation produces relative and absolute intravascular volume loss → shock.
This unifies the apparently separate findings of petechiae, purpura, thrombocytopenia, prolonged clotting times, cold ischaemic limbs, hypotension, and multi-organ failure.
High Yield Summary
- N. meningitidis is an encapsulated, oxidase-positive Gram-negative diplococcus that ferments glucose and maltose.
- Pili + IgA protease establish nasopharyngeal carriage; capsule + factor H binding permit bloodstream survival.
- LOS-rich blebs drive endothelial injury, capillary leak, DIC, and shock.
- Terminal complement deficiency impairs MAC killing; asplenia impairs clearance of encapsulated bloodstream organisms.
- Serogroup B capsule is poorly immunogenic because it resembles human polysialic acid, so MenB vaccines use recombinant proteins.
Active Recall - Meningococcal Foundations
[1] Lecture slides: GC 105. Medically important microbes what every doctor should know.pdf (Gram-negative cocci classification and encapsulated-organism risk) [2] Senior notes: Gen Clerk Anaes + Microbiology Summary.pdf (meningococcal biology and invasive disease) [3] Centre for Health Protection: Meningococcal Infection (reviewed March 2026)
Clinical Disease: Recognise the Syndrome Before It Declares Itself
Invasive meningococcal disease (IMD) is uncommon but time-critical. In Hong Kong, 94 cases were notified from 2005 to June 2025, with a median annual incidence of 0.07 per 100,000, an overall case-fatality rate of 13%, and serogroup B accounting for 50% of typed disease. Most cases were sporadic. [3]
| Risk setting | Why risk rises | Clinical implication |
|---|---|---|
| Infancy, adolescence/young adulthood, older age | Immune maturation, high carriage/social mixing, or immunosenescence | Keep a low threshold when compatible symptoms evolve rapidly. |
| Household/intimate contact | Repeated close exposure to respiratory and throat secretions | Contacts require urgent public-health risk assessment and often chemoprophylaxis. |
| Dormitory, barracks, institutional crowding | Close prolonged contact and shared airspace/social behaviours facilitate secretion exchange | Explains outbreak clusters; crowding alone does not mean every casual contact needs prophylaxis. |
| Smoking or passive smoke; recent viral URTI | Mucosal injury impairs ciliary clearance and epithelial barrier integrity | Makes invasion after colonisation more likely. |
| Asplenia | Poor clearance of encapsulated bloodstream organisms | Fulminant septicaemia risk; vaccination is indicated. |
| C5-C9 deficiency or complement-inhibitor therapy | Failure of MAC-mediated Neisseria killing | Recurrent or unusual meningococcal disease is a clue. |
| Advanced HIV or other immunodeficiency | Impaired humoral/complement cooperation | Vaccination and early assessment are important. |
| Travel to meningitis belt, Hajj/Umrah, or an outbreak area | Higher exposure to circulating epidemic serogroups | Pre-travel MenACWY or destination-matched vaccination may be required. |
| Laboratory exposure to meningococcal isolates | Aerosol or mucosal inoculation risk | Occupational vaccination and strict biosafety are required. |
Meningococcal meningitis and meningococcaemia overlap, but the dominant physiology differs.
| Feature | Meningococcal meningitis | Meningococcaemia / meningococcal sepsis |
|---|---|---|
| Primary compartment | Subarachnoid space and meninges | Bloodstream and microvasculature |
| Typical clues | Fever, severe headache, neck stiffness, photophobia, vomiting | Fever, intense limb/back myalgia, rapidly progressive non-blanching rash, cold extremities, prolonged capillary refill, hypotension |
| Dominant mechanism | Neutrophilic meningeal inflammation → BBB leak, oedema, raised ICP | LOS-mediated endothelial injury → capillary leak, vasoplegia, myocardial dysfunction, DIC |
| Rash | May be present | Often prominent, but absence does not exclude early disease |
| Main immediate threat | Raised ICP, cerebral hypoperfusion, seizures | Shock, purpura fulminans, multi-organ failure |
GC lecture exam anchor: fever/confusion with a petechial or purpuric rash is a neurological and septic emergency; treatment must not wait for imaging or lumbar puncture. [1]
Clinical Evolution From First Principles
Fever, malaise, nausea/vomiting, coryzal or pharyngeal symptoms, and a “flu-like” illness can precede invasive disease. These symptoms are non-specific because they reflect circulating cytokines rather than a uniquely meningeal process.
Intense myalgia, especially limb or back pain, matters because early tissue hypoperfusion and inflammatory mediator release can precede classic meningism. A patient who looks disproportionately ill deserves repeated examination.
| Finding | Why it occurs |
|---|---|
| Fever | IL-1/TNF induce hypothalamic prostaglandin E2 and reset the temperature set-point. |
| Headache/photophobia | Inflamed pain-sensitive meninges and trigeminal afferents are stretched; light worsens meningeal/ocular discomfort. |
| Neck stiffness | Inflamed cervical meninges and roots trigger painful reflex paraspinal muscle spasm during neck flexion. |
| Vomiting | Meningeal inflammation and raised ICP activate medullary vomiting pathways. |
| Reduced consciousness/seizures | Cerebral oedema, impaired perfusion, infarction, metabolic disturbance, or meningoencephalitic involvement indicates severe disease. |
The classic triad is not sufficiently sensitive to exclude meningitis. Infants may show irritability, poor feeding, lethargy, a bulging fontanelle, or temperature instability rather than neck stiffness.
The rash is a bedside window into the microcirculation:
- LOS activates endothelium and coagulation.
- Dermal microvascular thrombi cause focal ischaemia.
- Platelet/factor consumption plus vessel injury permits blood extravasation.
- Small non-blanching petechiae can coalesce into ecchymoses and necrotic purpura.
Pressure does not empty extravasated blood, so the rash remains visible during the glass test. Do not wait for a rash: fulminant meningococcaemia may initially have normal skin.
Meningococcal shock combines:
- Distributive physiology: nitric-oxide-mediated vasodilation lowers systemic vascular resistance.
- Relative hypovolaemia: endothelial leak moves fluid and albumin out of vessels.
- Myocardial depression: inflammatory mediators impair cardiac contractility.
- Obstructed microcirculation: DIC-related thrombi reduce tissue oxygen delivery.
This explains why a patient may have tachycardia, prolonged capillary refill, mottled/cold limbs, oliguria, metabolic acidosis, and altered mentation before measured hypotension appears.
| Syndrome | Clinical clue | Mechanism |
|---|---|---|
| Pharyngitis | Sore throat resembling streptococcal pharyngitis | Local nasopharyngeal inflammation; invasive disease must be judged from systemic features. |
| Septic arthritis | Acute mono-/oligoarthritis with systemic illness | Direct bloodstream seeding of synovium. |
| Pneumonia | Fever, cough, consolidation, especially with some serogroups/older patients | Aspiration or lower-respiratory invasion followed by inflammation. |
| Chronic meningococcaemia | Recurrent fever, migratory arthralgia, intermittent rash | Low-grade persistent bacteraemia with immune phenomena; rare. |
| Immune-complex pericarditis/arthritis | Symptoms appearing during recovery | Antigen-antibody complexes deposit after bacterial control; distinguish from persistent infection. |
| Presentation | Important alternative | Discriminator |
|---|---|---|
| Acute bacterial meningitis | S. pneumoniae | Gram-positive lancet diplococci; no characteristic meningococcal purpura; pneumococcus is often the leading adult bacterial cause. |
| Meningitis after pig/pork exposure in Hong Kong | Streptococcus suis | Gram-positive cocci; occupational exposure; striking risk of sensorineural hearing loss. |
| Fever + purpura + shock | Severe pneumococcal sepsis, rickettsial disease, viral haemorrhagic illness, TTP/HUS, acute leukaemia | Culture/PCR, travel/exposure, blood film and coagulation pattern; treat suspected meningococcal disease immediately while investigating. |
| Fever + rash + normal perfusion | Viral exanthem | Blanching rash and stable physiology are reassuring but do not replace serial assessment. |
| Meningism with lymphocytic CSF | Viral or TB meningitis | CSF differential and glucose ratio; TB is particularly relevant in Hong Kong. |
Exam Guardrail: Frequency Claims
Do not memorise “second most common cause” as a universal ranking. The position of N. meningitidis varies with age, geography, vaccination, and outbreak status. For HKUMed adult cases, identify it from Gram-negative diplococci + abrupt meningitis and/or rapidly progressive non-blanching rash, while remembering that pneumococcus is commonly the leading adult bacterial cause and TB meningitis is locally important.
High Yield Summary
- Invasive disease presents as meningitis, meningococcaemia, or both.
- Early flu-like symptoms and severe myalgia can precede rash and shock.
- A non-blanching petechial/purpuric rash reflects endothelial injury plus DIC; its absence does not exclude early disease.
- Shock is a combined vasoplegic, capillary-leak, myocardial, and microthrombotic process.
- Hong Kong incidence is very low, but disease remains rapidly fatal and legally notifiable when suspected.
Active Recall - Meningococcal Clinical Disease
[1] Lecture slides: GC 051. Fever and confusion_meningitis and encephalitis; suppurative brain infection.pdf (presentation, rash, and emergency approach) [2] Lecture slides: GC 105. Medically important microbes what every doctor should know.pdf (Gram-negative cocci and encapsulated-organism framing) [3] Centre for Health Protection: Updated Recommendations on the Use of Meningococcal Vaccines in Hong Kong (28 July 2025) [4] Centre for Health Protection: Meningococcal Infection (reviewed March 2026)
Diagnosis: Treat First, Confirm in Parallel
Suspected invasive meningococcal disease is a clinical emergency, not a diagnosis that waits for laboratory certainty.
GC lecture rule: obtain a quick septic work-up and blood cultures, perform early lumbar puncture when safe, but never allow CT or LP to delay high-dose parenteral antibiotics. [1]
If drawing blood would delay antibiotics in an unstable patient, give antibiotics first.
| Test/assessment | Expected or important finding | Why it matters |
|---|---|---|
| Serial vitals, GCS, capillary refill, urine output | Tachycardia, fever, poor perfusion, falling BP, altered consciousness | Trends reveal evolving shock earlier than a single BP reading. |
| Full skin examination | Petechiae, purpura, ecchymoses, peripheral ischaemia | Supports invasive disease and reveals DIC severity; mark lesion margins to monitor progression. |
| CBC and film | Neutrophilia or leukopenia; thrombocytopenia | Low platelets suggest consumption in DIC; leukopenia in overwhelming sepsis is ominous. |
| PT, APTT, fibrinogen, D-dimer | Prolonged PT/APTT, low fibrinogen, high D-dimer | Defines consumptive coagulopathy and determines procedural/transfusion safety. |
| Blood gas and lactate | Metabolic/lactic acidosis | Indicates tissue hypoperfusion and helps track resuscitation. |
| Urea/creatinine, LFT, glucose, electrolytes | AKI, hepatic injury, hypoglycaemia or sodium/potassium disturbance | Detects organ failure and possible adrenal crisis. |
| Blood cultures | Growth of N. meningitidis from a sterile site | Confirms invasive disease and permits susceptibility testing. Draw before antibiotics if this causes no delay. |
| Whole-blood PCR/NAAT | Meningococcal DNA | Particularly valuable after antibiotics have reduced culture yield. |
Perform LP promptly when the patient is stable and there is no contraindication. Defer it for significant cardiorespiratory instability, major coagulopathy/thrombocytopenia, local infection at the puncture site, or clinical concern for a mass lesion/pressure gradient. If neuroimaging is required first, start treatment before transfer.
Collect:
- Opening pressure.
- Cell count and differential.
- Protein.
- CSF glucose with a paired serum glucose.
- Gram stain.
- Bacterial culture and antimicrobial susceptibility.
- Meningococcal or multiplex PCR/NAAT.
- Additional tests driven by the differential, such as HSV PCR, cryptococcal antigen, or TB studies.
Typical pyogenic CSF pattern
| Parameter | Typical bacterial meningitis pattern | Mechanism |
|---|---|---|
| Opening pressure | Raised | Inflammatory oedema and impaired CSF absorption increase intracranial pressure. |
| Appearance | Turbid | Large numbers of neutrophils and protein scatter light. |
| White cells | Neutrophilic pleocytosis | Innate immune recruitment responds to extracellular bacteria. |
| Protein | Raised | BBB permeability allows plasma proteins into CSF. |
| CSF:serum glucose ratio | Low, often < 0.4 | Activated leukocytes/bacteria consume glucose and inflamed transport systems impair entry. |
| Gram stain | Gram-negative diplococci, often within neutrophils | Rapid presumptive clue; sensitivity falls after antibiotics or with low bacterial burden. |
| Culture | May grow N. meningitidis | Gives definitive identification and susceptibility, but antibiotics can sterilise CSF quickly. |
| PCR | Meningococcal DNA detected | Can remain useful after antimicrobial exposure and does not require viable organisms. |
The paired glucose ratio is a recurring HKUMed written-paper discriminator: an apparently “normal” absolute CSF glucose may be abnormally low relative to a high serum glucose. [1]
| Step | Finding | Interpretation |
|---|---|---|
| Sterile-site microscopy | Kidney-bean-shaped Gram-negative diplococci, sometimes intracellular | Probable meningococcal disease in a compatible clinical syndrome. |
| Culture | Small grey colonies on enriched chocolate/blood agar in CO₂-enriched conditions | Fastidious organism; prompt transport and pre-antibiotic sampling improve yield. |
| Oxidase | Positive | Supports Neisseria/Moraxella group identification. |
| Carbohydrate utilisation | Glucose and maltose positive | Classical distinction from N. gonorrhoeae (glucose only). |
| MALDI-TOF/modern identification | Species-level protein fingerprint | Rapid identification from culture in equipped laboratories. |
| PCR/NAAT | Species/serogroup nucleic acid | Confirms culture-negative disease and supports surveillance. |
| Serogrouping and sequencing | Capsular group and strain relationships | Guides outbreak investigation and vaccine response. |
| Susceptibility testing | Penicillin/cephalosporin/ciprofloxacin profile | Required before narrowing to penicillin and increasingly relevant to prophylaxis choice. |
Do not culture a routine throat swab to “rule out” invasive disease: asymptomatic carriage is possible, and a negative nasopharyngeal sample does not exclude bloodstream or CNS infection.
Hong Kong classifies a clinically compatible illness as confirmed when N. meningitidis is isolated, antigen is detected, or nucleic acid is detected from a normally sterile site such as blood or CSF. Compatible illness plus Gram-negative diplococci in sterile fluid is a probable case. [3]
Invasive meningococcal infection is notifiable in Hong Kong on suspicion; do not wait for laboratory confirmation. Early notification enables contact assessment, chemoprophylaxis, and outbreak control.
| Pattern | Most useful discriminator |
|---|---|
| S. pneumoniae meningitis | Gram-positive lancet-shaped diplococci; alpha-haemolysis; optochin susceptibility/bile solubility. |
| H. influenzae meningitis | Tiny pleomorphic Gram-negative coccobacilli; X and V factor dependence. |
| Listeria monocytogenes meningitis | Gram-positive rods/coccobacilli; tumbling motility; elderly, pregnant, neonatal, or immunocompromised host. |
| S. suis meningitis | Gram-positive cocci with pig/pork occupational exposure and high hearing-loss risk. |
| Viral meningitis | Lymphocytic CSF with usually normal glucose ratio and milder protein rise. |
| TB/fungal meningitis | Subacute course; lymphocytic CSF, low glucose, high protein; targeted PCR/culture/antigen tests. |
High Yield Summary
- Meningococcal disease is treated on clinical suspicion; cultures, CT, and LP must not delay ceftriaxone.
- Obtain blood cultures and whole-blood PCR; perform LP when safe.
- Pyogenic CSF is typically high pressure, neutrophilic, high protein, and low glucose ratio.
- Gram-negative intracellular diplococci are a rapid clue; culture enables susceptibility testing, while PCR retains value after antibiotics.
- Notify suspected invasive disease promptly in Hong Kong.
Active Recall - Meningococcal Diagnosis
[1] Lecture slides: GC 051. Fever and confusion_meningitis and encephalitis; suppurative brain infection.pdf (urgent work-up, LP, CSF interpretation, and treatment timing) [2] Senior notes: Gen Clerk Anaes + Microbiology Summary.pdf (meningococcal identification and meningitis investigations) [3] Centre for Health Protection: Communicable Disease Surveillance Case Definitions, Version 18.12 (revised 24 February 2025) [4] WHO: Guidelines on meningitis diagnosis, treatment and care (2025)
Treatment and Prevention: Kill Fast, Then Stop Secondary Cases
Treat suspected meningococcal disease as both bacterial meningitis and fulminant sepsis until the phenotype is clear.
GC lecture principle: high mortality and morbidity follow delayed treatment; use early high-dose parenteral antibiotics that penetrate the blood-brain barrier, then streamline when microbiology results are available. [1]
Antimicrobial strategy
| Situation | Preferred approach | Why |
|---|---|---|
| Suspected disease before susceptibility | IV ceftriaxone or cefotaxime | Reliable activity, bactericidal action, and therapeutic CSF penetration in inflamed meninges. |
| Confirmed penicillin-susceptible isolate | Continue ceftriaxone/cefotaxime or narrow to IV benzylpenicillin | Narrowing is stewardship-friendly, but reduced penicillin susceptibility exists, so do not assume sensitivity. |
| Severe immediate β-lactam allergy | Urgent microbiology/infectious-disease advice; use a locally supported alternative | The consequences of inadequate CNS therapy are severe, and cross-reactivity/allergy phenotype must be weighed against drug efficacy. |
| Ceftriaxone unavailable in a constrained setting | WHO allows limited use of long-acting chloramphenicol in specified circumstances | This is a contingency pathway, not the routine answer for every penicillin or β-lactam allergy. |
Current WHO guidance uses ceftriaxone or cefotaxime empirically and allows penicillin G/ampicillin/amoxicillin only for a penicillin-susceptible meningococcal isolate; a typical directed course is 5–7 days, adjusted to clinical response and local protocol. [3]
Sketchy Treatment Guardrail
The purple pencil is a valid reminder that penicillin can treat susceptible meningococcus, but penicillin is not the safest blind empirical monotherapy. Likewise, chloramphenicol is not the automatic modern substitute for any β-lactam allergy. Start ceftriaxone/cefotaxime, clarify the allergy and susceptibility, and involve microbiology for alternatives.
Ceftriaxone binds penicillin-binding proteins and blocks peptidoglycan cross-linking. A growing bacterium cannot maintain cell-wall integrity, so osmotic stress causes death. High-dose IV administration creates reliable serum levels and, during meningeal inflammation, clinically useful CSF exposure.
Rapid killing is lifesaving but can transiently increase release of inflammatory bacterial components. In suspected acute bacterial meningitis, follow the local dexamethasone protocol and give it before or with the first antibiotic dose when indicated; never delay antibiotics to arrange steroid administration. The strongest established adult benefit is in pneumococcal rather than proven meningococcal meningitis.
Antibiotics alone do not reverse established shock:
- Give oxygen and support ventilation if required.
- Use careful crystalloid resuscitation with frequent reassessment; capillary leak can worsen oedema.
- Start noradrenaline early for persistent vasoplegic shock and involve ICU.
- Correct hypoglycaemia and major electrolyte abnormalities.
- Monitor urine output, lactate, perfusion, mental state, and limb viability.
- Treat clinically significant DIC with source control plus targeted platelets, fresh frozen plasma, or cryoprecipitate guided by bleeding and laboratory results.
- Suspect Waterhouse-Friderichsen syndrome in refractory shock with compatible biochemical features; give stress-dose hydrocortisone according to adrenal-crisis protocol without waiting for confirmatory testing.
- Manage raised ICP, seizures, respiratory failure, AKI, and myocardial dysfunction with appropriate critical-care and specialty teams.
Use droplet precautions in addition to standard precautions. The patient is generally considered non-infectious after 24 hours of effective antimicrobial therapy. Staff exposed only through routine care do not automatically need prophylaxis; unprotected direct exposure to respiratory secretions during intubation, suction, or mouth-to-mouth resuscitation does.
Public-health teams determine eligibility. High-yield contact groups include:
- Household members or people frequently sleeping/eating in the same dwelling.
- Day-care contacts where close secretion exposure is plausible.
- Intimate kissing contacts.
- Anyone directly exposed to oral/nasal secretions.
- Healthcare workers with unprotected airway secretion exposure.
- Context-dependent prolonged close proximity, such as more than 8 hours within 1 metre, from 7 days before symptom onset until 24 hours after effective therapy. [3]
Casual classroom, ward, workplace, or transport proximity without direct secretion exposure is usually not enough by itself.
Give prophylaxis as soon as possible, ideally within 24 hours after the index patient is identified. Do not wait for the contact to develop symptoms; prophylaxis eradicates nasopharyngeal carriage before invasion. Vaccination does not replace immediate chemoprophylaxis for an eligible exposure.
| Agent | Typical role | Key cautions |
|---|---|---|
| Rifampicin | Traditional first-line oral option; given as a short multi-dose course | Potent drug interactions, orange body fluids, reduced oral-contraceptive effectiveness, pregnancy cautions, and possible resistance. |
| Ciprofloxacin | Convenient single-dose oral option where local susceptibility supports use | Avoid when ciprofloxacin-resistant meningococci are circulating; follow public-health advice. |
| Ceftriaxone | Single IM option; preferred during pregnancy in WHO guidance | Injection required; useful when oral agents are unsuitable. |
| Azithromycin | Alternative selected by public health in areas with ciprofloxacin resistance | Not a universal first choice; resistance ecology and local policy matter. |
Index patient carriage eradication
Ceftriaxone usually eradicates nasopharyngeal carriage. If the index case was treated with an agent that may not eradicate carriage, such as penicillin alone, give eradication therapy before discharge according to public-health/microbiology advice.
Vaccination
Pure capsular polysaccharide activates B cells poorly, especially in young children, and produces limited immune memory. Linking polysaccharide to a carrier protein recruits T-cell help:
| Vaccine | Antigen strategy | Exam logic |
|---|---|---|
| MenACWY conjugate | Capsular polysaccharides from A, C, W, Y linked to a carrier protein such as diphtheria-derived protein or tetanus toxoid, depending on product | Covers four major capsular groups and generates T-dependent memory. |
| MenB | Recombinant surface proteins, sometimes with outer-membrane vesicle antigen depending on product | Serogroup B capsule mimics human polysialic acid and is poorly immunogenic, so proteins are targeted instead. |
Hong Kong does not currently recommend universal meningococcal vaccination in the Childhood Immunisation Programme because local IMD incidence is very low. The July 2025 recommendation targets people at increased risk: [4]
- Travellers to the sub-Saharan meningitis belt during the dry season.
- Hajj/Umrah pilgrims and travellers to outbreak areas.
- Long-term travellers following destination-country recommendations.
- People with advanced HIV, terminal complement deficiency, or asplenia.
- Laboratory workers routinely exposed to N. meningitidis isolates.
Vaccine choice must match risk: MenACWY does not cover serogroup B, and MenB does not replace MenACWY when A/C/W/Y protection is required.
- Notify suspected invasive meningococcal infection promptly.
- Coordinate contact identification, medical surveillance, chemoprophylaxis, and outbreak assessment with the Centre for Health Protection.
- Educate contacts to seek urgent care for fever, severe headache, myalgia, rash, or systemic illness even after prophylaxis.
- Consider reactive vaccination when directed during a cluster/outbreak; it does not replace antibiotics for already exposed eligible contacts.
High Yield Summary
- Start IV ceftriaxone immediately; narrow to benzylpenicillin only after susceptibility is known.
- Resuscitate shock and treat DIC/adrenal crisis in parallel with antibiotics.
- Use droplet precautions until 24 hours of effective therapy.
- Eligible close contacts need rapid chemoprophylaxis: rifampicin, ciprofloxacin, or ceftriaxone according to patient and resistance factors.
- MenACWY uses conjugated capsular antigen; MenB uses recombinant proteins.
- Hong Kong uses risk-based rather than universal meningococcal vaccination.
Active Recall - Treatment and Prevention
[1] Lecture slides: GC 051. Fever and confusion_meningitis and encephalitis; suppurative brain infection.pdf (urgent therapy, chemoprophylaxis, and CNS treatment principles) [2] Senior notes: Gen Clerk Anaes + Microbiology Summary.pdf (meningococcal treatment and contact prophylaxis) [3] WHO: Guidelines on meningitis diagnosis, treatment and care (2025) [4] Centre for Health Protection: Updated Recommendations on the Use of Meningococcal Vaccines in Hong Kong (28 July 2025) [5] CDC: Clinical Guidance for Meningococcal Disease (updated June 2026) [6] CDC: Public Health Strategies for Antibiotic-resistant Neisseria meningitidis (accessed July 2026)
Complications and Exam Links
Most acute systemic complications arise from one reinforcing loop:
GC lecture lists meningococcal sepsis complications as meningitis, petechial/purpuric rash, septic shock, DIC, renal failure, and peripheral gangrene. [1]
Disseminated intravascular coagulation is simultaneous pathological clotting and bleeding:
- LOS/cytokines induce endothelial tissue factor.
- Thrombin generation deposits fibrin throughout small vessels.
- Platelets and clotting factors are consumed.
- Natural anticoagulants, including the protein C pathway, are impaired.
- Microthrombi cause skin, renal, adrenal, and limb ischaemia.
- Factor/platelet depletion and damaged vessels cause petechiae, purpura, ecchymoses, and procedural-site bleeding.
| Domain | Finding | Mechanism |
|---|---|---|
| Skin | Rapidly spreading non-blanching purpura, necrosis | Dermal microthrombi plus haemorrhage |
| Blood | Low platelets/fibrinogen, prolonged PT/APTT, high D-dimer | Consumptive coagulopathy and fibrinolysis |
| Kidney | AKI, rarely cortical necrosis | Shock plus renal microthrombi |
| Limbs | Digital ischaemia, peripheral gangrene | Distal microvascular thrombosis, shock, and vasopressor burden |
| Brain | Infarction or haemorrhage | Meningeal vasculitis, thrombosis, DIC |
Protein C is not simply “missing because of the bacterium.” Severe inflammation downregulates thrombomodulin/endothelial protein C receptor, consumes anticoagulant proteins, and suppresses activated-protein-C generation. Loss of this brake permits thrombin production to accelerate.
Meningococcal shock is often refractory because several defects coexist:
- Vasodilation lowers systemic vascular resistance.
- Capillary leak depletes intravascular volume.
- Myocardial depression lowers cardiac output.
- DIC blocks nutritive microvascular flow.
- Adrenal haemorrhage may remove cortisol/aldosterone support.
Consequences include lactic acidosis, AKI, hepatic injury, ARDS, encephalopathy, myocardial dysfunction, limb ischaemia, and death.
Waterhouse-Friderichsen syndrome is acute adrenal failure from bilateral adrenal haemorrhagic necrosis, classically during fulminant meningococcaemia.
The electrolyte triad is mechanistically correct but may be incomplete early in catastrophic sepsis; do not wait for “textbook” hyperkalaemia or imaging. Treat suspected adrenal crisis with stress-dose hydrocortisone while resuscitating and treating infection.
| Complication | Pathophysiology | Clinical result |
|---|---|---|
| Cerebral oedema/raised ICP | BBB injury, cytotoxic swelling, impaired CSF absorption | Headache, vomiting, reduced GCS, herniation |
| Hydrocephalus | Inflammatory exudate blocks CSF absorption/flow | Worsening ICP; enlarged head/bulging fontanelle in infants |
| Cerebral infarction | Leptomeningeal arteritis and thrombosis | Focal deficits, seizures |
| Cranial nerve injury/hearing loss | Basal exudate, labyrinthitis, CN VIII or vascular injury | Sensorineural hearing impairment |
| Seizures/epilepsy | Cortical inflammation, infarction, oedema, metabolic disturbance | Acute seizures and later epilepsy |
| Subdural effusion/empyema or abscess | Local extension of infection | Persistent fever, focal signs, mass effect |
| SIADH | CNS inflammation drives inappropriate ADH release | Dilutional hyponatraemia, worsening oedema and seizures |
Survivors require neurological, developmental/cognitive, and audiological follow-up.
Pericarditis and arthritis may develop during recovery when circulating meningococcal antigens form antibody complexes that deposit in tissues and activate complement. The timing matters:
- Early focal joint infection can be direct septic seeding and needs culture/drainage.
- Later sterile polyarthritis/pericarditis after microbiological improvement suggests immune-complex disease.
Do not assume every recurrent fever is immune-mediated; first exclude persistent infection, abscess, or inadequate therapy.
| Exam stem clue | What the examiner is testing | Best reasoning chain |
|---|---|---|
| Fever + confusion + non-blanching rash | Recognition of meningococcal meningitis/sepsis | Treat immediately; blood culture/PCR; LP only when safe; notify and assess contacts. |
| CSF neutrophils + high protein + low glucose ratio | Pyogenic meningitis interpretation | Use paired serum glucose; do not rely on absolute CSF glucose. CSF interpretation recurs in Fourth Summative papers. [1] |
| Gram-negative diplococci | Organism identification | N. meningitidis in meningitis; distinguish from gonococcus using clinical site and maltose fermentation. |
| Purpura + low platelets + prolonged PT/APTT + low fibrinogen | DIC | LOS → tissue factor → microthrombi → consumption → thrombosis plus bleeding. |
| Shock + bilateral adrenal haemorrhage | Waterhouse-Friderichsen syndrome | DIC causes adrenal haemorrhagic necrosis → acute cortisol/aldosterone deficiency. |
| Recurrent meningococcal infection | Terminal complement deficiency | Test complement pathways; C5-C9 are required for MAC-mediated Neisseria killing. |
| Splenectomy/Howell-Jolly bodies | Encapsulated-organism risk | Vaccinate against meningococcus, pneumococcus, and Hib; recognise OPSI risk. [2] |
| Close household contact | Secondary prevention | Give prompt chemoprophylaxis; vaccination history does not remove the immediate need. |
| Serogroup B vaccine question | Immunology, not list recall | Human-like polysialic capsule is poorly immunogenic → recombinant protein vaccine. |
- Waiting for the rash: invasive disease may be advanced before purpura appears.
- Waiting for LP: antibiotics come first if LP/CT would delay treatment.
- Calling every close-by person a contact: prophylaxis focuses on household/intimate/direct secretion or qualifying prolonged close exposure.
- Using penicillin blindly: narrow only after susceptibility confirmation.
- Treating MenACWY and MenB as interchangeable: their antigen coverage differs.
- Calling meningococcus universally “second most common”: frequency depends on population and vaccine era.
- Equating thrombocytopenia with vasoconstriction: it primarily reflects platelet consumption in systemic coagulation activation.
High Yield Summary
- LOS-driven endothelial injury unifies capillary leak, shock, DIC, purpura, renal injury, and limb ischaemia.
- Waterhouse-Friderichsen syndrome is bilateral adrenal haemorrhagic necrosis causing acute adrenal failure and refractory shock.
- Meningitis can cause raised ICP, infarction, seizures, hydrocephalus, hearing loss, and SIADH.
- Delayed arthritis/pericarditis may be immune-complex mediated, but persistent infection must be excluded.
- Exam answers should connect recognition → immediate ceftriaxone → safe confirmation → notification/contact prophylaxis.
Active Recall - Complications and Exam Links
[1] Lecture slides: GC 051. Fever and confusion_meningitis and encephalitis; suppurative brain infection.pdf (meningococcal sepsis complications and recurrent CSF exam themes) [2] Lecture slides: GC 105. Medically important microbes what every doctor should know.pdf (asplenia and encapsulated-organism exam correlation) [3] Past papers: 2021 Fourth Summative SAQ.pdf (post-BMT/asplenia encapsulated-organism risk) [4] Past papers: 2021 Fourth Summative Assessment MCQ.pdf and 2022 Fourth Summative MCQ.pdf (CSF interpretation) [5] Senior notes: Gen Clerk Anaes + Microbiology Summary.pdf (meningococcal complications and prophylaxis)
Neisseria meningitidis: Integrated Revision Summary
| Domain | Must know |
|---|---|
| Identity | Encapsulated, oxidase-positive Gram-negative diplococcus; human-only nasopharyngeal coloniser |
| Classical laboratory discriminator | Ferments glucose + maltose; gonococcus classically ferments glucose only |
| Colonisation | Type IV pili + Opa/Opc adhesins + IgA protease |
| Bloodstream survival | Capsule, factor H-binding protein, antigenic/phase variation |
| Main inflammatory driver | LOS and LOS-rich outer-membrane blebs |
| Major syndromes | Meningitis; meningococcaemia/septic shock; less often pneumonia, septic arthritis, chronic meningococcaemia |
| Highest-yield hosts | Close secretion contacts, crowded living, asplenia, C5-C9 deficiency/complement blockade, advanced HIV, high-risk travellers, exposed laboratory workers |
| Organism | Gram/morphology | Key discriminator | Major clue |
|---|---|---|---|
| N. meningitidis | Gram-negative diplococci | Glucose + maltose; capsule | Meningitis ± rapidly progressive purpura/sepsis |
| N. gonorrhoeae | Gram-negative diplococci | Glucose only; no polysaccharide capsule | Urethritis/cervicitis, PID, disseminated arthritis-dermatitis |
| S. pneumoniae | Gram-positive lancet diplococci | Alpha-haemolytic, optochin susceptible, bile soluble | Common adult bacterial meningitis; no classic meningococcal purpura |
| H. influenzae | Pleomorphic Gram-negative coccobacilli | X and V factor requirement | Meningitis in susceptible/unimmunised hosts |
| S. suis | Gram-positive cocci | Pig/pork exposure | Hong Kong-relevant meningitis with hearing loss |
| Syndrome | Recognition | Immediate danger |
|---|---|---|
| Meningitis | Fever, headache, neck stiffness, photophobia, vomiting, altered GCS | Cerebral oedema, seizures, infarction, herniation |
| Meningococcaemia | Fever/flu-like prodrome, severe limb/back myalgia, non-blanching petechiae/purpura | Capillary-leak shock, DIC, myocardial dysfunction |
| Waterhouse-Friderichsen | Refractory shock ± hypoglycaemia, hyponatraemia, hyperkalaemia | Bilateral adrenal haemorrhagic necrosis and acute adrenal crisis |
| Delayed immune-complex disease | Arthritis or pericarditis during recovery | Must distinguish sterile inflammation from persistent infection |
Expected bacterial CSF
Raised pressure + neutrophils + high protein + low CSF:serum glucose ratio. Gram-negative intracellular diplococci strongly suggest meningococcus. Culture gives susceptibility; PCR remains useful after antibiotics.
| Intervention | Key point |
|---|---|
| Droplet precautions | Continue until 24 hours of effective antibiotics. |
| Close-contact prophylaxis | Prompt rifampicin, ciprofloxacin, or IM ceftriaxone according to pregnancy, interactions, and resistance/public-health advice. |
| MenACWY | Conjugated capsular polysaccharides A/C/W/Y → T-cell help and memory. |
| MenB | Recombinant surface proteins because group B capsule resembles human polysialic acid and is poorly immunogenic. |
| Hong Kong policy | Risk-based vaccination; no universal childhood programme because incidence is very low. |
| High-risk groups | Asplenia, terminal complement deficiency, advanced HIV, exposed laboratory workers, selected travellers. |
GC 105: classify first — Gram-negative cocci → Neisseria → meningococcus; connect the encapsulated organism to asplenic risk. [1]
GC 051: fever/confusion, non-blanching rash, CSF interpretation, immediate parenteral therapy, and contact chemoprophylaxis are the examinable clinical chain. [2]
- Paired serum glucose prevents misclassification of bacterial CSF.
- Recurrent meningococcal infection points to terminal complement failure.
- Purpura + thrombocytopenia + prolonged clotting + low fibrinogen is DIC.
- Bilateral adrenal haemorrhage + refractory shock is Waterhouse-Friderichsen syndrome.
- Ceftriaxone is empirical; penicillin is susceptibility-directed.
- MenACWY and MenB are complementary, not interchangeable.
- Gram-negative kidney-bean diplococci
- Oxidase positive; glucose + maltose
- Pili, IgA protease, capsule, factor H-binding protein, LOS
- Humans only; nasopharyngeal carriage; close secretion spread
- Meningitis ± meningococcaemia
- Non-blanching rash may be absent early
- DIC, shock, Waterhouse-Friderichsen
- Blood culture/PCR; LP only when safe
- Immediate IV ceftriaxone
- Droplet precautions and urgent contact prophylaxis
- MenACWY conjugate; MenB recombinant proteins
- Notify suspected invasive disease in Hong Kong
High Yield Summary
Think encapsulated Gram-negative diplococcus + maltose + meningitis/purpura. The decisive pathogenesis chain is LOS → endothelial injury → capillary leak + DIC → shock. Do not wait for rash, CT, or LP before ceftriaxone. Confirm with sterile-site culture/PCR, narrow only after susceptibility, notify public health, and protect close contacts.
Active Recall - Neisseria meningitidis
[1] Lecture slides: GC 105. Medically important microbes what every doctor should know.pdf [2] Lecture slides: GC 051. Fever and confusion_meningitis and encephalitis; suppurative brain infection.pdf [3] Centre for Health Protection: Updated Recommendations on the Use of Meningococcal Vaccines in Hong Kong (28 July 2025) [4] WHO: Guidelines on meningitis diagnosis, treatment and care (2025)
Sketchy Micro hooks for Neisseria meningitidis
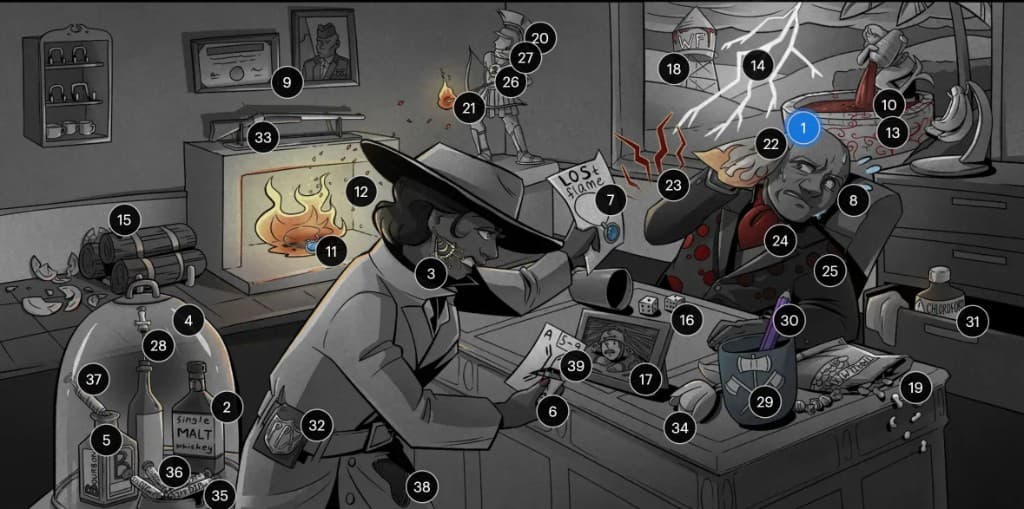
How to Use This Sketchy
The 39 supplied symbols are grouped below by the clinical sequence identity/colonisation → invasion/vascular injury → presentation/complications → diagnosis/treatment → prevention. The Clinically reconciled note concept column is the medical source of truth; the Sketchy meaning is retained as the recall hook.
Important Guardrails
- “Second most common cause” varies by age, country, vaccine era, and outbreak status; do not use it as a universal ranking.
- Ceftriaxone/cefotaxime is the empirical backbone. Penicillin is used only after susceptibility is confirmed.
- Chloramphenicol is a constrained-setting contingency in current WHO guidance, not the routine answer for every β-lactam allergy.
- Close-contact prophylaxis is not defined by time alone: household/intimate/direct secretion exposure matters, and public health performs the final assessment.
- Current MenACWY vaccines are usually conjugate vaccines; carrier proteins vary by product. MenB uses non-capsular protein antigens.
| No. | Visible symbol | Sketchy meaning | Clinically reconciled note concept | Why the association works | Lecture / exam link |
|---|---|---|---|---|---|
| 1 | Blue “General Mater” figure | Neisseria meningitidis, meningococcus | Encapsulated, oxidase-positive Gram-negative diplococcus; human nasopharyngeal pathogen causing meningitis and meningococcaemia. | “General Mater” sounds like the central meningococcal character; the paired kidney-bean diplococci are the diagnostic morphology. | GC 105: Gram-negative cocci → Neisseria. |
| 2 | Single MALT whiskey bottle | Maltose fermentation | Meningococcus ferments glucose and maltose; gonococcus classically ferments glucose only. | MALT → maltose; the “single” bottle helps contrast the carbohydrate tests. | Classic organism-identification discriminator. |
| 3 | Pili earring hanging beside the nose | Pili promote nasopharyngeal colonisation | Type IV pili establish attachment to nasopharyngeal epithelium and undergo antigenic/phase variation. | Hair-like pili beside the nose place attachment at the nasopharynx. | Virulence-factor → portal-of-entry reasoning. |
| 4 | Liquor bottle shaped like a capsule | Protective capsule | Polysaccharide capsule resists complement-dependent opsonisation and phagocytosis, enabling bloodstream survival. | The bottle/capsule encases and protects its contents. | Encapsulated-organism risk in asplenia. |
| 5 | Bourbon bottle inside the capsule | Serogroup B capsule is poorly immunogenic | Group B capsule resembles human polysialic acid, creating immune tolerance; MenB therefore targets surface proteins. | Bourbon = “B”; it sits inside the capsule to specify serogroup B. | Explains MenB vaccine design. |
| 6 | Torn ace playing card | IgA protease | Meningococcal IgA protease cleaves secretory IgA and weakens mucosal immune exclusion. | Torn “ace” sounds like cleaved IgA. | Connect enzyme to mucosal adherence. |
| 7 | Card marked “LOSt flame” | Lipooligosaccharide | LOS is a TLR4-active endotoxin that drives cytokines, endothelial injury, capillary leak, DIC, and shock. | “LOSt” directly cues LOS; the flame cues inflammation. | Central meningococcal sepsis mechanism. |
| 8 | Spreading sweat droplets | Respiratory droplet spread | Transmission requires close exposure to respiratory/throat secretions; casual distant contact is lower risk. | Droplets visibly spread from the person. | Contact history and droplet precautions. |
| 9 | Military portrait beside a diploma | Barracks and college outbreaks | Crowded, prolonged close-contact environments such as military quarters and dormitories facilitate transmission. | Military image + diploma combine the two classic congregate settings. | Outbreak epidemiology; do not equate all classmates with close contacts. |
| No. | Visible symbol | Sketchy meaning | Clinically reconciled note concept | Why the association works | Lecture / exam link |
|---|---|---|---|---|---|
| 10 | Flowing red fountain | Haematogenous invasion | After mucosal traversal, bacteraemia permits meningeal seeding and systemic meningococcaemia. | The flowing red fountain represents organisms spreading through blood. | Explains meningitis and sepsis occurring together or separately. |
| 11 | Burning “LOSt” flame | LOS inflammatory response | LOS-TLR4 signalling releases TNF-α, IL-1, IL-6 and activates endothelium/coagulation. | The LOS flame has become intensely inflammatory. | Mechanism behind abrupt deterioration. |
| 12 | Spreading embers from the flame | LOS-rich blebs amplify inflammation | Outer-membrane vesicles shed LOS, distributing inflammatory stimulus beyond intact bacteria. | Embers spread fire just as blebs spread LOS. | Explains disproportionate endotoxaemia. |
| 13 | Red vines overtaking the fountain | Vascular injury | Endothelial damage causes capillary leak, tissue-factor activation, microthrombi, haemorrhage, and necrosis. | Vines invade and obstruct the red vascular fountain. | Links LOS to purpura fulminans. |
| 14 | Lightning bolt | Capillary leak → shock | Leak plus vasodilation depletes effective circulating volume; myocardial depression and microthrombi worsen shock. | A lightning strike cues sudden cardiovascular collapse. | Meningococcal shock can evolve within hours. |
| 15 | Fallen plates beside stacked firewood | Thrombocytopenia and thrombosis | Platelets are consumed by DIC while widespread fibrin microthrombi obstruct vessels; vasoconstriction is not the primary cause of thrombocytopenia. | Fallen plates = low platelets; stacked wood resembles obstructive thrombi. | Exam correction: consumption produces low platelets. |
| 16 | Rolled dice | Disseminated intravascular coagulation | DIC causes simultaneous microvascular thrombosis and bleeding through platelet/factor consumption. | Dice sounds like DIC. | Purpura + low platelets + prolonged PT/APTT + low fibrinogen. |
| 17 | “Protein C” corporal in the picture | Protein C pathway dysfunction | Endothelial injury, reduced thrombomodulin signalling, and consumption impair activated protein C, removing a physiological anticoagulant brake. | The corporal labelled C cues protein C. | Explains runaway thrombin generation. |
| 18 | “WF” water tower | Waterhouse-Friderichsen syndrome | Bilateral adrenal haemorrhagic necrosis during fulminant meningococcaemia causes acute adrenal insufficiency and refractory shock. | WF initials directly cue the eponym. | Classic sepsis complication. |
| 19 | Falling peanuts/candies and hanging bananas | Hypoglycaemia, hyponatraemia, hyperkalaemia | Loss of cortisol may cause hypoglycaemia; loss of aldosterone causes sodium/volume loss and potassium retention. Early catastrophic disease may not show the complete triad. | Falling sweets = low glucose; falling salty peanuts = low sodium; raised bananas = high potassium. | Treat suspected adrenal crisis without waiting for textbook electrolytes. |
| No. | Visible symbol | Sketchy meaning | Clinically reconciled note concept | Why the association works | Lecture / exam link |
|---|---|---|---|---|---|
| 20 | Meningitis mohawk | Bacterial meningitis | Meningococcus is a major vaccine-preventable cause of acute bacterial meningitis, especially in children and young adults. | The mohawk highlights the meninges/head. | Identify from GN diplococci + meningitic syndrome. |
| 21 | Antibody-shaped flaming arrow | Immune-complex complications | Delayed sterile arthritis or pericarditis can follow antigen-antibody complex deposition; exclude persistent infection first. | Antibody arrow landing in inflamed tissue cues immune-complex injury. | Timing distinguishes immune disease from septic seeding. |
| 22 | Flame-pattern bandana | Febrile flu-like prodrome | Fever, malaise, vomiting, coryzal/pharyngeal symptoms, and systemic illness may precede classic signs. | Flame = fever; bandana gives a flu-like “ill” appearance. | Early disease may look non-specific. |
| 23 | Pain lines around the body | Intense myalgia | Severe limb/back muscle pain can precede rash and reflect inflammation and early tissue hypoperfusion. | Zig-zag pain lines directly cue myalgia. | “Pain out of proportion” is an early warning. |
| 24 | Red necktie | Pharyngitis | Local nasopharyngeal disease may resemble streptococcal pharyngitis; systemic toxicity determines urgency. | A red tie at the throat cues pharyngeal inflammation. | Do not diagnose invasive disease from throat symptoms alone. |
| 25 | Red-spotted jacket | Petechial rash | Dermal microthrombi, endothelial injury, and haemorrhage produce non-blanching petechiae/purpura. Rash may be absent early. | Red spots on clothing mirror skin petechiae. | Glass test; treat fever + new purpura as emergency. |
| 26 | Second-place figure | “Second most common” meningitis cause | Frequency is setting-dependent, not a fixed universal rank. In HK adult exams, pneumococcus is commonly leading; identify meningococcus from morphology, age/outbreak context, and rash. | Second place preserves the supplied mnemonic while the guardrail prevents false generalisation. | Exam asks organism recognition more reliably than global rank. |
| 27 | Neck brace | Fever, headache, neck stiffness | Meningeal inflammation causes headache and reflex painful cervical muscle spasm; altered consciousness or focal signs imply severe disease/complication. | The brace makes neck stiffness visible. | GC 051 core meningitis presentation. |
| No. | Visible symbol | Sketchy meaning | Clinically reconciled note concept | Why the association works | Lecture / exam link |
|---|---|---|---|---|---|
| 28 | Needle through a cork | Lumbar puncture and CSF | When safe, CSF typically shows raised pressure, neutrophils, high protein, low paired glucose ratio, and GN diplococci; culture/PCR confirm. Do not delay antibiotics for LP. | Needle entering the cork cues lumbar puncture. | Paired serum glucose is a recurrent paper theme. |
| 29 | Three-bladed axe | Ceftriaxone | Immediate IV ceftriaxone/cefotaxime is empirical first-line therapy because activity and CSF penetration are reliable. | “Tri-axe” sounds like cef-tri-ax-one. | Give before delayed CT/LP. |
| 30 | Purple pencil | Penicillin | IV benzylpenicillin is effective only when susceptibility is confirmed; it is not the preferred blind empirical monotherapy. | Pencil sounds like penicillin. | Antimicrobial stewardship and resistance guardrail. |
| 31 | Chloroform bottle | Chloramphenicol | Long-acting chloramphenicol is a WHO contingency when ceftriaxone is unavailable in constrained settings, not the routine modern answer for all β-lactam allergy. | Chloroform cues chloramphenicol by name. | Clarify allergy urgently with microbiology/ID advice. |
| 32 | PPx shield | Close-contact prophylaxis | Household/intimate/direct secretion contacts and qualifying prolonged close exposure need urgent public-health assessment; WHO includes context such as more than 8 hours within 1 metre from 7 days before onset to 24 hours after effective treatment. | Shield = prevention after exposure. | Give promptly; vaccination does not replace immediate prophylaxis. |
| 33 | Collector’s rifle | Rifampicin prophylaxis | Rifampicin eradicates nasopharyngeal carriage but has interactions, orange secretions, contraceptive effects, and pregnancy cautions. | Rifle cues “rif-” in rifampicin. | Traditional short-course PEP option. |
| 34 | Flower | Ciprofloxacin prophylaxis | Single-dose ciprofloxacin is convenient where susceptibility supports it; avoid if resistant strains are circulating. | The flower cues “flora” clearance and the supplied ciprofloxacin hook. | Resistance patterns can change PEP choice. |
| No. | Visible symbol | Sketchy meaning | Clinically reconciled note concept | Why the association works | Lecture / exam link |
|---|---|---|---|---|---|
| 35 | Four syringe shooters beneath a capsule | Quadrivalent capsular vaccine | MenACWY targets capsular groups A, C, W, and Y; current products are usually protein-conjugate vaccines that generate immune memory. | Four syringes = four serogroups; capsule overhead = capsular antigen. | MenACWY does not cover group B. |
| 36 | Syringe marked “DIPped” | Carrier-protein conjugation | Capsular polysaccharide linked to a carrier protein recruits T-cell help; some products use diphtheria-derived protein, while carrier choice varies by vaccine. | “DIP” cues diphtheria carrier protein. | Conjugation → class switching, affinity maturation, memory. |
| 37 | Syringe inserted into Bourbon | MenB recombinant protein vaccine | Because group B capsule is poorly immunogenic and human-like, MenB vaccines use recombinant surface proteins/outer-membrane antigens. | Bourbon = B; syringe in it = MenB vaccination. | Distinguish antigen strategy from MenACWY. |
| 38 | Spleen-shaped hole in the coat | Vaccinate in asplenia | Functional/anatomical asplenia impairs clearance of encapsulated organisms; meningococcal vaccination is indicated alongside pneumococcal and Hib prevention. | Missing spleen-shaped patch depicts asplenia. | GC 105 and post-BMT/Howell-Jolly body exam link. |
| 39 | “MAC’s 5–9” card | Vaccinate in terminal complement deficiency | C5-C9 form MAC; deficiency or complement blockade causes recurrent invasive Neisseria risk and warrants vaccination plus specialist prevention planning. | The card explicitly binds MAC to 5–9. | Recurrent meningococcus → test CH50/AH50. |
High Yield Summary
Read the scene as a causal story: maltose-fermenting encapsulated diplococcus attaches to the nose → LOS-rich bacteraemia injures vessels → meningitis, purpura, DIC, shock, and adrenal haemorrhage → diagnose without delaying ceftriaxone → protect contacts and vaccinate by serogroup/risk.