Breast Cancer
Breast cancer is a malignant neoplasm arising from the epithelial cells of the breast ducts or lobules, with the potential for local invasion and distant metastasis.
Breast cancer is a malignant neoplasm arising from the epithelial cells lining the terminal duct-lobular unit (TDLU) of the breast. It encompasses a heterogeneous group of diseases — from pre-invasive (in-situ) carcinomas confined within the basement membrane to invasive carcinomas that penetrate through the basement membrane into surrounding stroma and have metastatic potential.
Break down the terminology:
- "Carcinoma" = malignancy of epithelial origin (as opposed to sarcoma which is mesenchymal).
- "In situ" (Latin: "in place") = malignant cells that have not breached the basement membrane.
- "Invasive" = malignant cells have breached the basement membrane and can access lymphovascular spaces.
The TDLU is the functional unit of the breast — the site where milk is produced (lobule) and drained (terminal duct). This is the epicentre of almost all breast pathology, both benign and malignant.
2. Epidemiology
- Breast cancer is the most common malignancy in women worldwide (surpassed lung cancer in 2020 per GLOBOCAN data) [1][2].
- Lifetime risk in Western countries: approximately 1 in 8 women.
- Higher incidence in Caucasians compared to Asians and Africans, though the gap is narrowing as Asian countries undergo epidemiological transition (Westernised diet, later childbearing, decreased breastfeeding) [1].
- Male-to-female ratio ≈ 1:100 (some sources quote 1:2000 for overall population risk; the ratio of actual cases is ~1:100) [1][2].
| Parameter | Detail |
|---|---|
| Incidence in females | 1st most common cancer in females [1][2] |
| Overall incidence (both sexes) | 3rd most common cancer [1] |
| Mortality in females | 3rd most common cause of cancer death [1] |
| Median age at diagnosis | ~55 years (younger than Western data — peak in 40s–50s in HK) [2] |
| Lifetime risk (HK) | ~1 in 16 [2] |
| Trend | Incidence rising steadily; attributed to Westernised lifestyle, later childbearing, reduced breastfeeding, and increased mammographic detection |
HK-Specific Point
Women in Hong Kong tend to develop breast cancer at a younger age (around the 40s) compared to Western populations where the peak is in the 60s–70s. This has implications for screening (starting earlier) and imaging (younger women have denser breasts, making USG an important adjunct to mammography) [1][3].
3. Anatomy & Function of the Breast
The breast sits on the anterior chest wall overlying the pectoralis major (and partly serratus anterior), extending from the 2nd to 6th rib vertically and from the sternal edge to the mid-axillary line horizontally. The axillary tail of Spence extends superolaterally towards the axilla — important clinically because tumours here can be mistaken for axillary lymphadenopathy.
The breast is divided into four quadrants by a vertical and horizontal line through the nipple:
| Quadrant | Proportion of breast tissue | Frequency of carcinoma |
|---|---|---|
| Upper outer quadrant (UOQ) | Most breast tissue | ~60% of breast cancers [4] |
| Upper inner quadrant (UIQ) | — | ~12% |
| Lower outer quadrant (LOQ) | — | ~10% |
| Lower inner quadrant (LIQ) | — | ~6% |
| Central / sub-areolar | — | ~12% |
Why is the UOQ the most common site? Simply because it contains the most glandular tissue (the bulk of the breast parenchyma is concentrated superolaterally, including the axillary tail).
The TDLU consists of:
- Lobules (acini) — milk-producing glandular units
- Terminal ducts — drain each lobule
- Lactiferous ducts — converge towards the nipple (15–20 per breast), each draining a lobe
- Lactiferous sinuses — dilated segments just behind the nipple that store milk
Two cell layers line the ducts and lobules:
- Inner luminal epithelial cells — secrete milk; give rise to most carcinomas
- Outer myoepithelial cells — contractile cells that squeeze milk out; sit on the basement membrane
The key distinction between in-situ and invasive carcinoma is whether the malignant cells have breached through the myoepithelial cell layer and basement membrane.
Understanding lymphatic drainage is critical for staging and surgical planning:
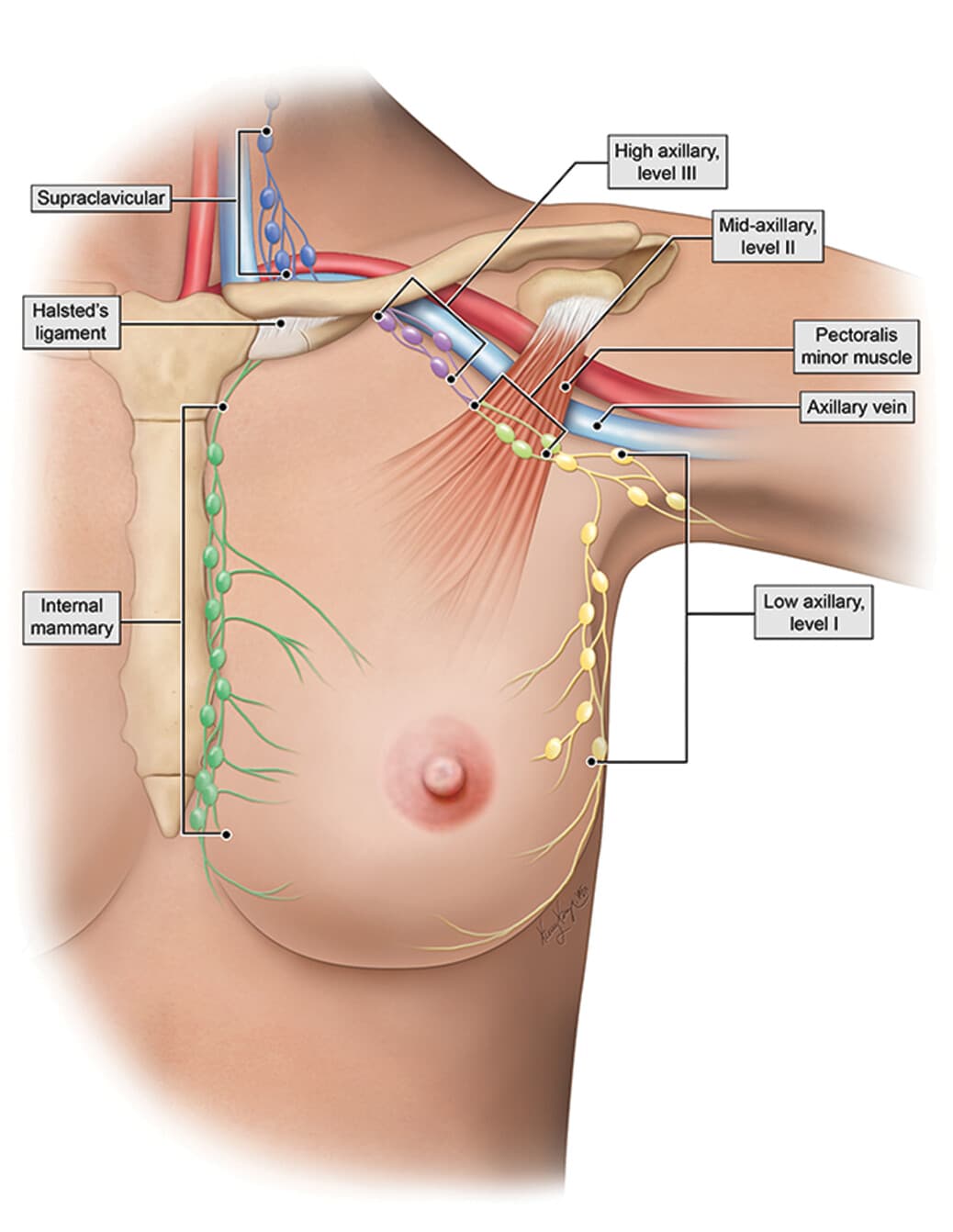
| Drainage route | Breast region drained | Clinical relevance |
|---|---|---|
| Axillary lymph nodes (Levels I–III) | Lateral tumours (outer quadrant) and central lesions | Most common route of regional spread; Level I = lateral to pectoralis minor, Level II = behind pec minor, Level III = medial to pec minor (infraclavicular) |
| Internal mammary (parasternal) nodes | Medial tumours (inner quadrant) and central lesions | Along internal thoracic artery; less accessible surgically |
| Supraclavicular nodes | Secondary spread from axillary or internal mammary chains | Involvement = N3c = Stage IIIC (advanced disease) |
| Interpectoral (Rotter's) nodes | Between pectoralis major and minor | Removed during Level II axillary dissection |
Lateral tumours in the outer quadrant and centrally located lesions drain primarily to axillary lymph nodes. Upper and lower inner quadrant tumours drain to internal mammary lymph nodes. [1]
Sentinel lymph node (SLN): The first lymph node to which cancer cells are most likely to spread from a primary tumour, usually the node closest to the tumour. A negative SLN biopsy indicates that cancer has likely not spread to regional lymph nodes, and full axillary lymph node dissection (ALND) can be avoided — sparing the patient morbidity from lymphoedema [1].
- Arterial: Internal thoracic artery (perforating branches), lateral thoracic artery, thoraco-acromial artery, posterior intercostal arteries
- Venous: Corresponding veins — importantly, the vertebral venous plexus (Batson's plexus) provides a valve-less route for haematogenous metastasis to the spine and pelvis (explaining why bone is the most common site of distant metastasis)
The breast is an endocrine target organ:
- Oestrogen → stimulates ductal proliferation
- Progesterone → stimulates lobular/alveolar development
- Prolactin → stimulates milk production
- Oxytocin → stimulates myoepithelial contraction (milk let-down)
This hormonal dependence is fundamental to understanding both the aetiology (prolonged oestrogen exposure → increased risk) and treatment (anti-oestrogen therapy) of breast cancer.
4. Etiology & Risk Factors
Think of breast cancer risk factors in a structured framework: Demographics → Genetics → Hormonal (endogenous & exogenous) → Medical history → Lifestyle → Radiation.
| Factor | Detail | Mechanism |
|---|---|---|
| Age | Risk increases with age; most cases diagnosed > 50 | Accumulation of somatic mutations over time |
| Sex | Female >> Male (M:F ≈ 1:100) [2] | Oestrogen-driven proliferation of breast epithelium in females |
| Ethnicity | Higher in Caucasians; increasing in Asians | Genetic and lifestyle factors |
4.2 Genetic / Hereditary Risk Factors (~10% of breast cancers)
BRCA1 and BRCA2 are the most common hereditary breast cancer genes [5][6].
- Mode of inheritance: Autosomal dominant with variable penetrance [1]
- Normal function: Both are tumour suppressor genes involved in homologous recombination DNA repair (specifically, repair of double-strand DNA breaks)
- Pathophysiology ("two-hit hypothesis"):
- First hit = germline mutation (inherited, present in all cells)
- Second hit = somatic mutation or loss of the remaining normal allele
- When both alleles are knocked out → loss of DNA repair capacity → genomic instability → accumulation of further mutations → malignant transformation [1]
| BRCA1 | BRCA2 | |
|---|---|---|
| Chromosome | 17q21 | 13q12 |
| Breast cancer risk by age 70 | ~65% (51–75%) [5] | ~45% (33–54%) [6] |
| Second primary breast cancer | ~40–60% lifetime [5] | High (lower than BRCA1) |
| Ovarian cancer risk | ~39% (22–51%) [5] | ~11% (4–18%) [6] |
| Male breast cancer | Uncommon | ~6% lifetime risk [6] |
| Prostate cancer | Increased risk [5] | Increased risk (~1.5–3 fold) [6] |
| Pancreatic cancer | Possible | Increased risk (~1.5–3 fold) [6] |
| Other associated cancers | Colon [5], fallopian tube, peritoneum | Laryngeal, bile duct, stomach, colon (minimal), melanoma [6] |
| Typical molecular subtype | Triple-negative (basal-like) [2] | ER+/HER2– more common |
BRCA Mutation Carrier Characteristics
Suspect BRCA mutation when you see [1]:
- Breast cancer diagnosed at early age (< 50)
- History of both breast and ovarian cancer in the same patient
- Family cases of breast and ovarian cancer
- Bilateral breast cancer
- Male breast cancer (especially BRCA2)
- Triple-negative breast cancer
Management of BRCA carriers: prophylactic bilateral mastectomy, bilateral salpingo-oophorectomy (BSO), and PARP1 inhibitors (e.g., olaparib — PARP inhibitors exploit "synthetic lethality" in BRCA-mutant cells that are already deficient in homologous recombination; blocking the remaining DNA repair pathway [PARP-mediated base excision repair] forces the cell into apoptosis) [2].
| Syndrome | Gene | Mechanism | Associated cancers |
|---|---|---|---|
| Li-Fraumeni syndrome | TP53 germline mutation | p53 is the "guardian of the genome" — loss leads to failure of cell cycle arrest and apoptosis in response to DNA damage | Breast cancer, sarcoma, brain tumours, adrenocortical cancer, leukaemia [1][2] |
| Cowden syndrome | PTEN mutation | PTEN is a phosphatase that negatively regulates PI3K/Akt pathway; loss → uncontrolled cell growth | Breast, thyroid, endometrial cancer; multiple hamartomas [2] |
| Hereditary diffuse gastric cancer | CDH1 (E-cadherin) gene mutation | Loss of cell–cell adhesion → predisposition to diffuse (signet ring) gastric cancer and lobular breast cancer | Diffuse gastric cancer, lobular breast cancer [1] |
| Peutz-Jeghers syndrome | STK11/LKB1 mutation | Tumour suppressor involved in cell polarity and energy sensing (AMPK pathway) | GI hamartomatous polyps, breast, ovary, pancreas [2] |
4.3 Hormonal Risk Factors
The overarching principle: prolonged and/or increased exposure to oestrogen drives proliferation of breast epithelial cells, increasing the chance of acquiring somatic mutations and developing hormone receptor-positive breast cancer [1][5].
| Factor | Why it increases risk |
|---|---|
| Early menarche ( < 12 years) [5] | Longer duration of cyclic oestrogen exposure |
| Late menopause ( > 55 years) [5] | Same — more ovulatory cycles |
| Nulliparity [5] | No interruption of menstrual cycling by pregnancy; no terminal differentiation of breast lobules |
| No breastfeeding [1] | Breastfeeding suppresses ovulation (via prolactin-mediated inhibition of GnRH) → reduces cumulative oestrogen exposure; also promotes terminal differentiation of lobular cells, making them more resistant to malignant transformation |
| Late age of first pregnancy ( > 30) [5] | Undifferentiated breast tissue exposed to oestrogen for longer before first full-term pregnancy induces terminal differentiation |
| Oestrogen-secreting ovarian tumour (e.g., granulosa cell tumour) | Direct exogenous oestrogen production |
Key concept: A full-term pregnancy before age 30 is protective because it induces terminal differentiation of breast lobular cells (Type 3 → Type 4 lobules), which are more genetically stable and less susceptible to carcinogenic transformation. Nulliparity or late first pregnancy means the breast retains immature, undifferentiated Type 1 and Type 2 lobules for longer — these are the cells most vulnerable to malignant change.
| Factor | Detail |
|---|---|
| Combined oral contraceptive pills (COC) [3][5] | Small increase in risk during use and shortly after; risk returns to baseline ~10 years after cessation |
| Hormone replacement therapy (HRT) [3][5] | Combined oestrogen-progestogen HRT increases risk; risk increases with duration of use; oestrogen-only HRT (in post-hysterectomy women) has a smaller or negligible increased risk |
Obesity risk depends on menopausal status [1]:
| Menopausal status | Effect of obesity | Mechanism |
|---|---|---|
| Pre-menopausal | Decreased risk | Obesity causes anovulation → less cyclic oestrogen peaks (oestrogen synthesis is primarily ovarian in pre-menopausal women) |
| Post-menopausal | Increased risk | After menopause, the ovaries cease oestrogen production. The primary source of oestrogen becomes peripheral adipose tissue via the aromatase enzyme (converts adrenal androgens to oestrone). More adipose tissue → more aromatase → more oestrogen → increased breast cancer risk |
This is also why aromatase inhibitors (e.g., anastrozole, letrozole) are used as treatment in post-menopausal ER+ breast cancer — they block this peripheral conversion.
Physical inactivity also increases risk, likely through obesity-related and insulin resistance mechanisms [5][3].
| Factor | Detail |
|---|---|
| Personal history of breast cancer | Increased risk of contralateral breast cancer [1] |
| Prior benign breast disease with atypia | Atypical ductal hyperplasia (ADH): 4–5× increased relative risk [1]; Atypical lobular hyperplasia (ALH): similar risk |
| Proliferative fibrocystic changes | Increased risk (moderate/florid hyperplasia, especially with atypia) [5] |
| LCIS | Premalignant condition — marker and precursor for bilateral invasive carcinoma (~1%/year) [5][7] |
| DCIS | Precursor to invasive ductal carcinoma of the same breast (~1%/year) [2] |
Relative Risk of Breast Cancer from Benign Breast Disease
American College of Pathologists Consensus Statement [4]:
| Risk Category | Lesions |
|---|---|
| No increased risk | Adenosis, apocrine metaplasia, cysts, duct ectasia, fibroadenoma, fibrosis, mild hyperplasia, mastitis, periductal mastitis, squamous metaplasia |
| Slightly increased (1.5–2×) | Moderate or florid hyperplasia (solid or papillary), papilloma with fibrovascular core |
| Moderately increased (5×) | Atypical hyperplasia (ductal or lobular) |
| Insufficient data | Solitary papilloma of lactiferous sinus, radial scar |
| Factor | Mechanism |
|---|---|
| Smoking [5] | Carcinogens in tobacco smoke (aromatic amines, polycyclic aromatic hydrocarbons) can form DNA adducts in breast tissue; also anti-oestrogenic effects may partly counterbalance this — net effect is a modest increase in risk |
| Alcohol [1] | Increases circulating oestrogen levels, generates acetaldehyde (a carcinogen), impairs folate metabolism (needed for DNA methylation and repair) |
| Diet [5] | High-fat, Westernised diets associated with higher risk (likely mediated through obesity) |
Exposure to therapeutic ionising radiation — particularly chest/mediastinal radiation at a young age (e.g., mantle radiation for Hodgkin lymphoma) — significantly increases breast cancer risk. The younger the age at exposure, the higher the risk (developing breast tissue is more radiosensitive) [1][5].
A brief but important mention [2][6]:
| Feature | Detail |
|---|---|
| Incidence | M:F ≈ 1:100 |
| Average age at diagnosis | 65 years |
| Risk factors | BRCA2 carriers, increased oestrogen exposure (oestrogen therapy, liver disease), radiation, Klinefelter's syndrome (47,XXY) — extra X chromosome → hypogonadism + relative oestrogen excess |
| Management | Mastectomy + SLNB/ALND (if clinically positive LN) |
5. Pathophysiology — Multi-Step Carcinogenesis
Breast cancer arises through a stepwise progression of genetic and epigenetic alterations:
- Initiation: A genetic insult (inherited or acquired) causes a mutation in a proto-oncogene or tumour suppressor gene (e.g., TP53, PIK3CA, BRCA1/2 loss, HER2 amplification)
- Promotion: Hormonal stimulation (especially oestrogen) drives proliferation of initiated cells, expanding the clone
- Progression: Additional mutations accumulate (loss of cell cycle control, angiogenesis activation, evasion of apoptosis) → in-situ carcinoma
- Invasion: Disruption of the basement membrane (loss of myoepithelial cell integrity, upregulation of matrix metalloproteinases) → invasive carcinoma
- Metastasis: Invasion of lymphovascular spaces → lymphatic spread (regional LN) and haematogenous spread (distant organs)
| Mode | Details |
|---|---|
| Direct spread | Into chest wall (pectoralis, intercostal muscles, ribs), skin and subcutaneous tissues |
| Lymphatic spread | Axillary LN (most common), internal mammary LN, supraclavicular LN |
| Haematogenous spread | Bone > Liver > Lung > Brain > Ovaries > Adrenals > Pleura [1][2] |
Why is bone the most common site of distant metastasis? Breast cancer cells have tropism for the bone marrow microenvironment — they express CXCR4 (chemokine receptor) that binds to CXCL12 (SDF-1) produced by bone marrow stromal cells. Additionally, the vertebral venous plexus (Batson's plexus) provides a direct, valveless venous route from the breast/thoracic wall to the vertebral column.
6. Classification
6.1 Histological Classification
Malignant cells confined within the basement membrane (i.e., no stromal invasion).
| Feature | Ductal Carcinoma In Situ (DCIS) | Lobular Carcinoma In Situ (LCIS) |
|---|---|---|
| Frequency | ~20% of all breast cancers [2] | Rare (incidental finding) |
| Pathology | Malignant cells within TDLU (ductal predominant) without invasion; Low grade: non-comedo (e.g., cribriform); High grade: comedo necrosis (central necrosis → dystrophic calcification) | Malignant cells within TDLU (lobular predominant) without invasion; loss of E-cadherin (cell adhesion molecule) |
| Clinical features | Asymptomatic, non-palpable; usually unifocal [2] | Asymptomatic, non-palpable; usually multifocal + multicentric [2] |
| Mammography | Microcalcifications (especially in comedo type — the necrotic debris calcifies) | Usually NAD (incidental finding on biopsy for other reasons) [2] |
| Cancer risk | Precursor to invasive ductal carcinoma of the same breast (~1%/year) [2] | Precursor AND marker of bilateral invasive carcinoma (ductal or lobular, ~1%/year) [2] |
| Grading | Van Nuys Prognostic Index (considers size, margin, grade, age) [2] | — |
| Management | BCS (2mm margin) + RT if high risk (first line if disease limited to one quadrant and cosmetically acceptable); Mastectomy + SLNB (SLNB because altered lymphatic drainage after mastectomy makes it impossible to perform SLNB later if IDC is found — 10–20% chance); Adjuvant: tamoxifen/AI if ER/PR+ [2] | Classical LCIS: close observation; Non-classical (pleomorphic) LCIS: more aggressive → surgical excision [2] |
Why SLNB with Mastectomy for DCIS?
A common point of confusion: "If DCIS is non-invasive, why do SLNB?" The answer is that mastectomy destroys the lymphatic drainage patterns of the breast. If the final mastectomy specimen reveals an occult invasive focus (which occurs in 10–20% of cases), you can no longer perform an accurate SLNB afterwards. So you do it at the time of mastectomy as a "safety net." [2]
| Subtype | Frequency | Key Features | Prognosis |
|---|---|---|---|
| Invasive ductal carcinoma, no special type (NOS) | ~80% [5][7] | Most common; forms a hard, stellate mass with desmoplastic stroma; various grades | Variable; depends on grade and stage |
| Invasive lobular carcinoma (ILC) | ~3–8% [2][7] | E-cadherin mutation → loose, diffuse infiltrating pattern ("Indian file" single-cell pattern) → more difficult to detect clinically and on mammography; usually ER+ only; associated with post-menopausal HRT use; tends to be multifocal, multicentric, bilateral; metastasises to unusual sites (meninges, GI tract, peritoneum) [1] | Similar to IDC overall; short-term outcomes may be more favourable [1] |
| Good-prognosis subtypes | Tubular, medullary, mucinous (colloid), papillary [1][7] | Better prognosis | |
| Poor-prognosis subtypes | Mixed ductal/lobular, metaplastic, micropapillary [1] | Worse prognosis | |
| Inflammatory breast cancer (IBC) | Rare | See below | Very poor |
Inflammatory Breast Cancer (IBC) [1]:
By definition T4d in TNM staging. A rare, aggressive form that resembles mastitis clinically and radiologically but is NOT a true inflammatory process.
The mechanism: tumour cells invade and obstruct the dermal lymphatic channels of the breast → lymphatic obstruction → oedema of overlying skin → peau d'orange (skin resembling an orange peel due to tethering at the sites of sweat gland/hair follicle openings while surrounding skin is oedematous).
Diagnostic criteria [1]:
- Rapid onset of breast erythema, oedema, peau d'orange, or warm breast ± underlying palpable mass
- Erythema occupying at least 1/3 of the breast
- Duration of history no more than 6 months
- Pathological confirmation of invasive carcinoma
Key distinguishing point: Mastitis → associated with fever and leukocytosis; IBC is NOT associated with these (it is not a true infection/inflammation) [1].
Paget's Disease of the Nipple [1]:
- "Paget" cells = malignant intraepithelial adenocarcinoma cells migrating from an underlying carcinoma into the epidermis of the nipple
- Characterised by eczematoid changes and ulcerated lesions of the nipple-areolar complex
- Almost ALWAYS (~80%) associated with an underlying breast cancer, which is typically HER2-positive [1]
- Presents with pain, burning, pruritus, palpable breast mass, bloody nipple discharge, or nipple inversion
- Diagnosis: full-thickness wedge biopsy of the nipple showing Paget cells
- Treatment: excision of the underlying cancer + nipple-areolar complex (mastectomy or BCT + whole-breast irradiation) [1]
This is a clinically crucial classification because it determines treatment strategy [1][2]:
| Subtype | IHC Definition | Frequency | Treatment | Prognosis |
|---|---|---|---|---|
| Luminal A | HR+/HER2−/Ki67 low | ~40% | Endocrine therapy alone (± cytotoxics if high nodal burden) [2] | Best prognosis |
| Luminal B (HER2−) | HR+/HER2−/Ki67 high | ~20% | Endocrine therapy ± cytotoxic therapy [2] | Intermediate |
| Luminal B (HER2+) | HR+/HER2+ | ~10% | Cytotoxics + anti-HER2 + hormonal therapy [2] | Intermediate |
| HER2-positive (non-luminal) | HR−/HER2+ | ~15% [1] | Cytotoxics + anti-HER2 therapy (e.g., trastuzumab); NO response to hormonal treatment [1] | Poor prognosis |
| Triple-negative (basal-like) | HR−/HER2− | ~15% [1] | Cytotoxic therapy (platinum-based); PARP inhibitors if BRCA-mutant; immunotherapy (pembrolizumab if PD-L1+); NO response to Herceptin or hormonal treatment [1] | Poor prognosis |
Understanding the Molecular Subtypes
Why do these subtypes matter? They dictate which therapeutic "weapons" you can use:
- ER/PR+ → You can use endocrine therapy (tamoxifen, aromatase inhibitors) because the tumour depends on oestrogen for growth.
- HER2+ → You can use anti-HER2 therapy (trastuzumab/Herceptin, pertuzumab) because the tumour overexpresses HER2 receptors driving proliferation.
- Triple-negative → You have no targeted receptor to exploit → relies on cytotoxic chemotherapy, though PARP inhibitors are now available for BRCA-mutant cases and immune checkpoint inhibitors (pembrolizumab) for PD-L1+ tumours.
Ki67 is a nuclear antigen that marks proliferating cells. High Ki67 = more aggressive, faster-growing tumour = more likely to respond to chemotherapy (because chemo targets rapidly dividing cells) but also carries a worse prognosis.
Key receptors explained:
- ER (Oestrogen Receptor): A nuclear transcription factor. When oestrogen binds → activates gene transcription promoting cell proliferation. Tamoxifen is a selective oestrogen receptor modulator (SERM) that competitively blocks oestrogen binding.
- PR (Progesterone Receptor): Expression is oestrogen-driven; PR+ confirms a functioning ER pathway. PR+ tumours have even better prognosis among HR+ cancers.
- HER2 (Human Epidermal growth factor Receptor 2): A transmembrane tyrosine kinase receptor (ErbB2/neu). Amplification → constitutive activation of downstream RAS-MAPK and PI3K-Akt pathways → uncontrolled proliferation. Trastuzumab ("Herceptin") is a monoclonal antibody that binds the extracellular domain of HER2, blocking signalling and marking the cell for immune-mediated destruction (ADCC).
The TNM staging system classifies breast cancer based on:
T — Primary Tumour:
| Stage | Description |
|---|---|
| Tis | Carcinoma in situ (DCIS, Paget's without associated mass) |
| T1 | ≤ 2 cm (T1mi ≤ 0.1 cm, T1a > 0.1–0.5 cm, T1b > 0.5–1 cm, T1c > 1–2 cm) |
| T2 | > 2–5 cm |
| T3 | > 5 cm |
| T4 | Any size with direct extension to chest wall (T4a), skin oedema/ulceration/satellite nodules (T4b), both (T4c), inflammatory carcinoma (T4d) |
N — Regional Lymph Nodes:
| Stage | Description |
|---|---|
| N0 | No regional LN metastasis |
| N1 | Movable ipsilateral axillary LN (Level I–II) |
| N2 | Fixed/matted ipsilateral axillary LN (N2a) or ipsilateral internal mammary LN without axillary LN involvement (N2b) |
| N3 | Ipsilateral infraclavicular LN (N3a), ipsilateral internal mammary + axillary LN (N3b), ipsilateral supraclavicular LN (N3c) |
M — Distant Metastasis:
| Stage | Description |
|---|---|
| M0 | No distant metastasis |
| M1 | Distant metastasis present (including contralateral supraclavicular LN) |
Stage Grouping:
| Stage | TNM | 5-Year Survival (HK) |
|---|---|---|
| Stage I | T1 N0 M0 | 97.5% [1] |
| Stage II | T0–1 N1, T2 N0–1, T3 N0 | 87.8% [1] |
| Stage III | T0–2 N2, T3 N1–2, T4, any N3 | 66.2% [1] |
| Stage IV | Any T, Any N, M1 | 19.3% [1] |
The AJCC 8th edition also introduced a Prognostic Stage that incorporates tumour grade, ER, PR, HER2 status, and genomic assays (e.g., Oncotype DX) — this can upstage or downstage patients relative to anatomic staging alone.
7. Clinical Features
| Symptom | Pathophysiological Basis |
|---|---|
| Painless breast lump (most common presenting complaint) | Malignant proliferation forms a mass; breast cancers are typically painless because they grow insidiously without stretching the breast capsule rapidly (unlike infection/inflammation). Pain can occur with larger tumours or inflammatory type |
| Nipple discharge (especially unilateral, single-duct, bloody) [2] | Tumour eroding into or arising from a duct → disrupts duct lining → bloody discharge. Serous/serosanguinous discharge may also occur. The high-risk features (unilateral, single duct, bloody) point towards an intraductal lesion (either papilloma or DCIS/invasive cancer) rather than bilateral physiological discharge |
| Nipple retraction/inversion (new onset) | Tumour invading and fibrosis of the subareolar lactiferous ducts → tethering and retraction of the nipple. Must distinguish from longstanding congenital inversion (benign) |
| Skin changes — peau d'orange | Tumour cells block dermal lymphatic channels → lymphatic oedema of the skin → skin pits at sweat gland/hair follicle openings (which are tethered by Cooper's ligaments), creating the "orange peel" appearance |
| Skin dimpling / tethering | Tumour invades or causes fibrotic reaction in Cooper's ligaments (suspensory ligaments that connect the breast parenchyma to the skin and chest wall) → shortening of these ligaments → dimpling of overlying skin, especially on raising arms |
| Skin ulceration | Advanced local disease — tumour erodes through skin (T4b) |
| Nipple eczema (Paget's disease) | Malignant cells (Paget cells) migrate from an underlying ductal carcinoma into the nipple epidermis → eczematous, crusting, erythematous change of the nipple-areolar complex [1] |
| Breast pain / mastalgia | Uncommon in breast cancer; when present, suggests inflammatory breast cancer (dermal lymphatic obstruction), rapid tumour growth, or nerve invasion. Non-cyclical, unilateral, focal pain warrants investigation [2] |
| Axillary lump | Lymphatic metastasis to axillary lymph nodes → may present as the primary complaint (sometimes the primary breast tumour is occult) |
| Constitutional symptoms | Weight loss, bone pain, shortness of breath [2] → suggest advanced/metastatic disease (bone metastasis, lung metastasis, liver metastasis) |
7.2 Signs
On physical examination (performed with patient at 45°) [2]:
| Sign | Pathophysiological Basis |
|---|---|
| Asymmetry | Tumour mass distorting breast contour |
| Skin changes — erythema, oedema, peau d'orange, dimpling, ulceration, satellite skin nodules | As described above — lymphatic obstruction, Cooper's ligament invasion, direct skin invasion |
| Nipple changes — the "5 Ds" [2]: Deviation, Discolouration, Dermatitis (Paget's), Depression (retraction), Discharge | Tumour traction on ducts (deviation, depression), epidermis invasion (dermatitis/Paget's), duct erosion (discharge), local inflammation (discolouration) |
| Surgical scars | Previous breast or axillary surgery |
A malignant breast mass classically has the following characteristics [1][2]:
| Feature | Malignant (Breast Cancer) | Benign (e.g., Fibroadenoma) |
|---|---|---|
| Consistency | Hard (desmoplastic stromal reaction around tumour) | Rubbery/firm |
| Border | Irregular, ill-defined (infiltrative growth pattern) | Well-defined, smooth |
| Surface | Irregular | Smooth |
| Tenderness | Usually non-tender | Non-tender or mildly tender |
| Mobility | Fixed to skin or underlying muscle (late sign — tumour invades Cooper's ligaments/pectoralis fascia) | Highly mobile ("breast mouse") |
| Site | Most commonly upper outer quadrant (~60%) [4] | Any quadrant |
Testing fixation:
- Skin fixation: Pinch the skin over the mass — if the mass is fixed to skin, the skin will dimple/pucker
- Chest wall/muscle fixation: Ask the patient to press hands on hips (contracts pectoralis major) — if the mass is fixed to the muscle, it becomes less mobile with contraction
The axillary lymph nodes are examined in five groups [2]:
- Anterior (pectoral) — along the lateral border of pectoralis major
- Posterior (subscapular) — along the lateral border of the scapula
- Medial (central) — high up against the chest wall
- Lateral (humeral) — along the medial aspect of the humerus
- Apical — at the apex of the axilla
Comment on: number, site, size, consistency, tenderness, fixation [2].
Involved nodes feel hard, non-tender, matted (fixed to each other), or fixed to adjacent structures. Also examine the supraclavicular fossa and infraclavicular region for lymphadenopathy.
| Site | Signs to elicit |
|---|---|
| Bone | Bony tenderness (spine, pelvis, long bones), pathological fractures |
| Liver | Hepatomegaly, jaundice, ascites |
| Lung/Pleura | Decreased breath sounds (effusion), crackles |
| Brain | Focal neurological deficits, signs of raised ICP |
| Term | Definition | Implication for Surgery |
|---|---|---|
| Multifocal | ≥ 2 foci within a limited area (usually same quadrant) | Not a contraindication to breast-conserving therapy (BCT) |
| Multicentric | ≥ 2 foci in different quadrants | Contraindication to BCT → mastectomy required |
8. Screening
The CEWG uses a risk-stratified approach rather than blanket annual screening:
- Average risk: Women aged 44–69 with certain combinations of risk factors may consider mammography every 2 years after discussion of benefits and harms [9].
- Moderate risk: Mammography every 2 years may be considered [9].
- High risk: Annual mammography is generally advised (starting age depends on risk profile), with specialist follow-up [9].
- Routine monthly scheduled breast self-examination (BSE) is no longer recommended for average-risk women.
- Routine clinical breast examination (CBE) as a screening test in asymptomatic average-risk women is also not recommended.
- Preferred strategy: breast awareness (knowing normal baseline breast appearance/feel) and prompt medical review for any new change.
| Guideline / Context | Recommendation (average risk) |
|---|---|
| Hong Kong CEWG | Consider biennial mammography for selected women aged 44–69 after individualized risk discussion |
| USPSTF (2024) | Biennial mammography age 40–74 |
| ACS | Age 40–44: option for annual mammogram; 45–54: annual; ≥55: biennial or continue annual |
Dense Breast Tissue and Supplemental Imaging
Criteria for referral for genetic counselling [1]:
- Personal history:
- Breast cancer diagnosed at age ≤ 50
- Triple-negative breast cancer
- Male breast cancer (BRCA2)
- Family history:
- ≥ 2 relatives with breast cancer, one diagnosed at age ≤ 50
- ≥ 3 relatives with breast cancer at any age
- Previous identified BRCA1/2 mutation in family
Principles of genetic testing [1]:
- Always test the AFFECTED individual first
- Only if a mutation is identified, then test unaffected family members
- NEVER test an unaffected individual first — because a negative result from a family where no mutation has been identified is uninformative (other predisposition genes may exist that haven't been identified yet)
| Category | Factors Associated with Poor Prognosis |
|---|---|
| Patient | Extreme of age (very young or very old), smoking |
| Tumour size | Large (higher T stage) |
| Nodal status | More nodes involved = worse |
| Metastasis | Presence of distant metastasis |
| Grade | Poorly differentiated (Grade 3) |
| Proliferation | High Ki67 (detected by immunohistochemistry) |
| Histological subtype | IDC, ILC, mixed ductal/lobular, metaplastic, micropapillary |
| Receptor status | Absence of ER/PR expression (cannot use endocrine therapy), HER2 overexpression (aggressive biology, though now targetable with trastuzumab) |
When assessing a patient with a breast complaint, use this systematic framework [2][3]:
Important questions in history-taking (must know!) [2]:
- Mass: Onset & progression, any cyclical changes / mastalgia
- Nipple: Discharge / retraction
- Skin: Itchiness, erythema, dimpling / peau d'orange
- Constitutional symptoms: Weight loss, bone pain, SOB
- Risk factors of malignancy:
- Family history: BRCA — any CA breast / ovary / prostate / pancreas [3]
- Past medical history: Prior breast disease (e.g., DCIS), prior breast/chest RT [3]
- Oestrogen exposure: Age of menarche, age of menopause, parity, breastfeeding, use of COC/HRT [3]
- First/second degree relative (age of onset) [3]
- Hormonal risk: menarche/menopause [3]
- Gestational history [3]
- Breastfeeding history [3]
- Previous breast screening (if any) [3]
High Yield Summary
Breast Cancer — Key Points:
-
Definition: Malignant neoplasm of breast epithelium (TDLU). In-situ vs. invasive depends on basement membrane breach.
-
Epidemiology (HK): 1st most common cancer in females, 3rd overall; median age ~55 (younger than West); lifetime risk 1:16.
-
Risk Factors — "Oestrogen Exposure" is the unifying theme: Early menarche, late menopause, nulliparity, no breastfeeding, late first pregnancy, COC/HRT, obesity (post-menopausal).
-
Genetics: BRCA1/2 (autosomal dominant tumour suppressor genes for DNA repair); Li-Fraumeni (TP53); Cowden (PTEN); CDH1 → lobular cancer.
-
BRCA1: ~65% breast cancer risk by 70, ~39% ovarian; associated with triple-negative subtype. BRCA2: ~45% breast cancer risk by 70, ~11% ovarian; associated with male breast cancer (~6%).
-
Pathology: IDC NOS (80%) > ILC (3–8%) > Special types. DCIS = precursor to IDC; LCIS = marker/precursor for bilateral invasive cancer.
-
Molecular Subtypes: Luminal A (best prognosis, endocrine therapy), Luminal B, HER2+ (anti-HER2 therapy), Triple-negative (worst prognosis, chemo/PARP/immunotherapy).
-
Clinical Features: Hard, irregular, fixed, non-tender mass in UOQ; nipple discharge (unilateral, bloody, single duct = high risk); peau d'orange (dermal lymphatic obstruction); skin dimpling (Cooper's ligament invasion); nipple retraction (duct fibrosis/invasion).
-
Paget's Disease: Eczematoid nipple change + underlying breast cancer (usually HER2+). IBC: T4d, peau d'orange ≥ 1/3 breast, < 6 months history, NOT true infection.
-
Screening (Current): Emphasize breast awareness and early assessment of new breast changes. Routine monthly BSE is not recommended for average-risk women. Use risk-based mammography (e.g., CEWG risk-stratified approach in HK; USPSTF biennial screening age 40–74).
-
Genetic Testing: Test affected individual first → only test unaffected relatives if mutation found.
Active Recall - Breast Cancer: Definition to Clinical Features
[1] Senior notes: felixlai.md (Breast cancer sections III, I, XIV, XV) [2] Senior notes: maxim.md (Sections 8.2, 8.3, 8.6, Breast carcinoma, DCIS/LCIS, Clinical features) [3] Lecture slides: GC 181. Breast mass breast cancer; benign breast diseases; mammography; breast cancer screening.pdf (pp. 8, 11, 33) [4] Senior notes: maxim.md (ACP Consensus table on benign breast disease risk; quadrant pie chart) [5] Lecture slides: The Management of breast cancer_Prof A Kwong 20_2_2020.pdf (pp. 30, 31, 33) [6] Lecture slides: The Management of breast cancer_Prof A Kwong 20_2_2020.pdf (p. 32) [7] Lecture slides: GC 181. Breast mass breast cancer; benign breast diseases; mammography; breast cancer screening.pdf (p. 33) [8] AJR: Axillary Lymph Node Anatomy and Imaging-Based Features. https://ajronline.org/doi/10.2214/AJR.19.22022 [9] Hong Kong Cancer Information Website (cancer.gov.hk). Breast cancer page with CEWG screening guidance: https://www.cancer.gov.hk/en/hong_kong_cancer/common_cancers_in_hong_kong/breast_cancer.html [10] U.S. Preventive Services Task Force. Breast Cancer: Screening (Final Recommendation Statement, 2024): https://www.uspreventiveservicestaskforce.org/uspstf/recommendation/breast-cancer-screening [11] American Cancer Society. Recommendations for the Early Detection of Breast Cancer: https://www.cancer.org/cancer/types/breast-cancer/screening-tests-and-early-detection/american-cancer-society-recommendations-for-the-early-detection-of-breast-cancer.html
Differential Diagnosis of Breast Cancer
The differential diagnosis of breast cancer really means: "A patient presents with a breast complaint — what could it be other than cancer, and how do I systematically work through the possibilities?" The approach differs depending on the presenting complaint: a breast lump, nipple discharge, nipple/skin change, or mastalgia. We will cover each systematically, explain why each mimicker can look like cancer, and clarify the distinguishing features.
Before diving in, understand the conceptual scaffold. Breast pathology can be classified under the ANDI framework (Aberrations of Normal Development and Involution) [2][8]:
- Development (15–25 years): Fibroadenoma, juvenile hypertrophy
- Cyclical changes (25–55 years): Fibrocystic changes, cyclical mastalgia, nodularity
- Involution ( > 35–55 years): Cysts, duct ectasia, sclerosing adenosis
Superimposed on this physiological framework are neoplastic (benign and malignant), infective/inflammatory, and miscellaneous conditions. The key clinical question is always: Is this cancer or not? — which is why the triple assessment (clinical + radiological + pathological) exists.
2. Differential Diagnosis by Presenting Complaint
The DDx depends heavily on age and characteristics of the lump [2]:
| Young ( < 35) | Older ( > 35) | |
|---|---|---|
| Soft | Fibrocystic changes | Fibrocystic changes |
| Firm | Fibroadenoma | Carcinoma |
| Fat necrosis | Fat necrosis (bruising history) | |
| Lipoma | Lipoma | |
| Breast cyst (tense, fluctuant) | Phyllodes tumour (freely mobile) |
Why does age matter? Because the pre-test probability of malignancy changes dramatically with age. In a 20-year-old, a firm mobile lump is overwhelmingly likely to be a fibroadenoma. In a 55-year-old, the same lump mandates urgent triple assessment to exclude carcinoma. The background incidence of breast cancer rises exponentially with age (accumulation of somatic mutations + longer cumulative oestrogen exposure).
Now let us go through each differential in detail.
The most common benign tumour of the breast [1][2].
| Feature | Detail | Why / Mechanism |
|---|---|---|
| Nature | Benign solid tumour containing glandular and fibrous tissue (fibro = fibrous; adeno = glandular; -oma = tumour) | Proliferation of both stromal and epithelial components of the TDLU [1][2] |
| Age | Reproductive age (15–35) | Likely a hormonally-dependent neoplasm — increases in size during pregnancy or with oestrogen-based OCP; persists during reproductive years; decreases in size or regresses after menopause [1] |
| Clinical presentation | "Breast mouse" — a highly mobile, well-defined, rubbery, non-tender mass [1] | The tumour is encapsulated within its own pseudocapsule and sits freely within breast tissue, hence the extreme mobility (slides under your finger like a mouse running away) |
| Distinguishing from cancer | Mobile (cancer is fixed), smooth borders (cancer is irregular), non-tender, does NOT cause skin changes or nipple retraction | Cancer invades Cooper's ligaments (dimpling, fixation) and ducts (retraction) — fibroadenoma does not |
| Cancer risk | Simple fibroadenoma: NO increased risk; Complex fibroadenoma (with papillary apocrine changes, ductal hyperplasia, sclerosing adenosis): higher risk [1] | Complex histological changes indicate increased proliferative activity within the lesion |
| Giant fibroadenoma | Defined as > 10 cm; CANNOT be distinguished from Phyllodes tumour on examination or imaging → must excise [1] | Both are fibroepithelial lesions; the stroma in Phyllodes is more cellular and can become malignant |
| Management | Conservative if < 2 cm with concordant imaging; wide local excision if symptomatic, > 2 cm, or increasing in size [1][2] | Not necessary to excise every biopsy-proven fibroadenoma — surgery can cause scarring and breast deformity |
| Feature | Detail | Why / Mechanism |
|---|---|---|
| Nature | Epithelial-lined fluid-filled cavity derived from the TDLU [1][8] | Fluid accumulates due to distension and obstruction of the efferent ductule of the TDLU [1] |
| Age | Young to perimenopausal women | Part of the involutionary spectrum — lobular involution with cystic dilation |
| Clinical presentation | Soft, fluctuant, well-defined, mobile lump; may be tender (especially with acute enlargement causing sudden-onset pain) [1][8] | Rapid distension of the cyst wall stretches pain fibres |
| Distinguishing from cancer | USG: simple anechoic fluid-filled structure with posterior acoustic enhancement — definitively benign. Complex cysts (with internal echoes/septae/solid component) need further workup | Cancer is a solid mass on USG; a simple cyst is never cancer |
| Management | Reassurance; aspiration (therapeutic and diagnostic — if blood-stained aspirate, recurrent, or radiologically suspicious → cytology and further workup) [2][8] | If the cyst disappears completely after aspiration and the fluid is not bloody, it is benign. Recurrence or solid component → excision |
The most common benign disorder of the breast [1][8].
| Feature | Detail | Why / Mechanism |
|---|---|---|
| Nature | NOT a disease but a spectrum of histopathological changes: stromal fibrosis, macro/microcysts, apocrine metaplasia, hyperplasia, adenosis [1] | Result of hormonal imbalance — oestrogen predominance over progesterone causing exaggerated cyclical changes [1] |
| Age | Reproductive (premenopausal) | Driven by menstrual cycle hormonal fluctuations |
| Clinical presentation | Cyclical painful mass/nodularity (worse before menses, improves after onset of menstrual flow); serosanguinous nipple discharge possible [1][8] | Oestrogen-driven proliferation and oedema in the first half of the cycle → engorgement and tenderness pre-menstrually; regression with progesterone withdrawal |
| Distinguishing from cancer | Cyclical variation (cancer lumps do NOT wax and wane with menstrual cycle); bilateral and diffuse rather than a single discrete hard mass | Cancer grows progressively; fibrocystic changes fluctuate |
| Cancer risk | Depends on histology (see ACP table [4]): no increased risk for simple cysts, fibrosis, mild hyperplasia; slightly increased (1.5–2×) for moderate/florid hyperplasia; moderately increased (5×) for atypical hyperplasia (ductal or lobular) [4] | Atypia = cells are acquiring pre-malignant features (abnormal architecture and cytology) |
| Management | Reassurance, avoid caffeine, evening primrose oil, analgesics, COC (to suppress cyclical hormonal fluctuation) [8] | — |
"Phyllodes" from Greek phyllon = leaf — refers to the characteristic leaf-like architecture on histology [1][2].
| Feature | Detail | Why / Mechanism |
|---|---|---|
| Nature | Fibroepithelial tumour (aka serocystic disease of Brodie) — classified as benign, borderline, or malignant [1][2] | Similar to fibroadenoma but with more cellular stroma that can undergo malignant transformation |
| Age | Older women ( > 40) [2] | Unlike fibroadenoma which peaks in youth |
| Clinical presentation | Smooth, painless, mobile mass — can grow very large rapidly [2] | Rapid stromal proliferation → fast growth distinguishes it from the slowly growing fibroadenoma |
| Distinguishing from cancer | Mobile (cancer is fixed), smooth surface; but can be malignant — and malignant Phyllodes metastasises via blood (haematogenous), NOT lymphatics → ALND is NOT required [2] | Sarcomatous stroma spreads haematogenously like other sarcomas, not via lymphatic routes like carcinomas |
| Axillary lymphadenopathy | Occurs in ~20% but is usually reactive (not metastatic) [1] | The large tumour causes local inflammation → reactive nodal hyperplasia |
| Management | Wide local excision with margin of at least 1 cm (mastectomy if adequate margin cannot be achieved) [2] | Wide margins are essential because of the high local recurrence rate; unlike fibroadenoma, simple enucleation is inadequate |
Phyllodes vs Fibroadenoma — Key Distinction
Giant fibroadenoma ( > 10 cm) CANNOT be distinguished from Phyllodes tumour on physical examination or imaging [1]. If you cannot differentiate, you must excise. On core needle biopsy, features favouring Phyllodes include: increased stromal cellularity, mitoses, stromal overgrowth, leaf-like architecture, and fragmentation [1].
| Feature | Detail | Why / Mechanism |
|---|---|---|
| Nature | Ischaemic necrosis of fat lobules [8] | Disrupted blood supply to fat → necrosis → inflammatory repair → fibrosis → hard lump |
| Risk factors | Trauma, iatrogenic (e.g., breast reconstruction, surgery, radiation) [8] | Direct physical damage to adipose tissue |
| Clinical presentation | Mimics carcinoma clinically: painless lump with skin dimpling, nipple retraction [8] | Fibrosis from fat necrosis tethers Cooper's ligaments and ducts, producing the same signs as cancer |
| Imaging | Mimics carcinoma radiologically — spiculated mass, calcifications [8] | Dystrophic calcification in necrotic fat; surrounding fibrosis creates spiculated margins |
| Diagnosis | Core biopsy to differentiate from cancer [8] — shows foamy macrophages, giant cells, fibrosis, fat globules surrounded by inflammatory infiltrate | The only way to be certain is tissue diagnosis |
| Management | Reassurance, analgesics [8] | Self-limiting; no treatment needed once cancer is excluded |
| Feature | Detail |
|---|---|
| Nature | Benign tumour of mature adipose tissue |
| Clinical presentation | Soft, well-defined, non-tender, mobile subcutaneous mass |
| Distinguishing from cancer | Soft consistency (cancer is hard); superficial and mobile; on imaging, fat density with thin capsule |
| Management | Conservative unless symptomatic → excision |
| Condition | Key Points |
|---|---|
| Sclerosing adenosis / Radial scars | Pathological diagnosis: lobular lesions with increased fibrosis [2]; can mimic carcinoma both clinically and on mammography → core biopsy to differentiate [2] |
| Adenoma | Benign glandular tumour, older age; can mimic carcinoma [2] |
| Diabetic (DM) mastopathy | Occurs in premenopausal women with Type 1 DM; hard mass from lymphocytic infiltration and fibrosis; does NOT increase breast cancer risk [1]; autoimmune-mediated |
| Pseudoangiomatous stromal hyperplasia (PASH) | Benign stromal proliferation; can present as a firm mass; biopsy to exclude angiosarcoma [1] |
| Idiopathic granulomatous mastitis (IGM) | Rare benign inflammatory disease mimicking carcinoma; young parous women; self-limiting (resolves 9–12 months); NO increased cancer risk; diagnosis of exclusion after excluding TB, sarcoidosis; biopsy shows granulomatous lesions centred on lobules [1] |
Nipple discharge is the second most common breast complaint. The critical question is: Is this physiological or pathological? [1][2]
History-taking for nipple discharge [2]:
- True nipple discharge? (from the nipple orifice, not skin)
- Unilateral or bilateral?
- Colour of discharge?
- Recent pregnancy/breastfeeding?
- Single duct or multiple ducts?
- Spontaneous or expressible?
| Feature | Likely Benign | Suspicious for Malignancy |
|---|---|---|
| Laterality | Bilateral | Unilateral |
| Number of ducts | Multiple | Single duct |
| Colour | Milky, yellow, green | Bloody or serosanguinous |
| Spontaneity | Only with expression | Spontaneous |
| Colour | Differential Diagnosis | Mechanism |
|---|---|---|
| Milky (bilateral, multiple ducts) | Physiological (pregnancy, lactation), Galactorrhoea (hyperprolactinaemia: prolactinoma, antipsychotics like haloperidol/risperidone, antiemetics like metoclopramide/domperidone, hypothyroidism, CKD) [1] | Prolactin drives milk production; any cause of elevated prolactin → bilateral milky discharge. Drug-induced: dopamine normally inhibits prolactin release from the anterior pituitary; dopamine antagonists (antipsychotics, metoclopramide) remove this inhibition → hyperprolactinaemia |
| Yellow/green/black (multicoloured) | Ductal ectasia [1][8] | Abnormal dilatation of subareolar ducts with accumulation of lipid-rich secretions → "creamy, cheesy" discharge; can be green/blue/black depending on duration and oxidation of lipid material |
| Serous/serosanguinous | Intraductal papilloma (most common cause of pathological nipple discharge) [1][2], fibrocystic changes, DCIS | Papilloma: muscularis arteries supply the peduncle but lymphatics/veins are compromised → increased vascular pressure → transudate into duct lumen [1] |
| Bloody | Intraductal papilloma (bleeding from friable papilloma surface), CA breast/DCIS, fibrocystic changes with active intraductal component [1][2] | Tumour or papilloma erodes into blood vessels within the duct wall → haemorrhagic discharge |
Malignancy is the underlying cause in 5–15% of cases of pathological nipple discharge, and the most common malignancy associated is DCIS [1].
Investigations for nipple discharge [2]:
- Triple assessment
- ± Nipple discharge cytology
- ± Ductogram / ductoscopy (to localise intraductal lesion before microdochectomy)
| Condition | Presentation | Mechanism | How to Distinguish from Cancer |
|---|---|---|---|
| Paget's disease of the nipple [1][3][9] | Eczematous changes involving the nipple; unilateral; associated with malignancy within the same breast (~80%); malignant epithelial (Paget) cells infiltrate and proliferate in the epidermis, causing thickening of the nipple and areolar skin [9] | Malignant intraepithelial adenocarcinoma cells migrate from underlying ductal carcinoma into nipple epidermis via lactiferous ducts | This IS cancer (or associated with cancer). Not a mimic but a special presentation of breast cancer. Diagnosed by full-thickness wedge biopsy showing Paget cells [1]. Mammography mandatory to look for associated mass and exclude synchronous cancers [1] |
| Nipple eczema (dermatitis) | Bilateral, involves areola more than nipple, itchy, responds to topical steroids | Contact dermatitis or atopic eczema — allergen-mediated immune response | Bilateral involvement and areolar predominance favours eczema. Paget's is unilateral, centred on the nipple, does not respond to steroids, and progressively worsens |
| Duct ectasia | Nipple retraction (from periductal fibrosis), "blue breast" (cyst with dark fluid), multicoloured discharge [8] | Dilated subareolar ducts → inflammation → fibrosis → nipple retraction and periductal mastitis | NOT associated with increased cancer risk [1]; nipple retraction from duct ectasia is often bilateral and gradual, while cancer-related retraction is unilateral and progressive |
| Inflammatory breast cancer (IBC) [1][2] | Painful swollen breast with erythema, oedema, peau d'orange involving at least 1/3 of breast; T4d | Invasion of local dermal lymphatic ducts by tumour → lymphatic obstruction → cutaneous oedema [2] | IBC resembles mastitis but is NOT a true inflammatory process — no fever, no leukocytosis (unlike mastitis which has both) [1]. If "mastitis" does not respond to antibiotics within 1–2 weeks → must biopsy to exclude IBC |
| Lactational mastitis | Tender, swollen, erythematous breast in a breastfeeding woman; fever, leukocytosis; may progress to abscess [1] | S. aureus (most common) or streptococci enter through nipple fissures → infection of breast tissue → suppurative inflammation [8] | Fever + leukocytosis + lactational context → mastitis. Responds to antibiotics. If no response → consider abscess or IBC |
| Mondor's disease | Palpable subcutaneous cord along the breast/chest wall; chest pain [8] | Superficial sclerosing thrombophlebitis of breast/chest wall veins (thoraco-epigastric vein most common, also lateral thoracic, superior epigastric) [8] | The palpable cord is diagnostic; no breast mass; self-limiting |
Paget's Disease vs. Nipple Eczema
A classic exam trap. Paget's = unilateral, centred on the nipple, does NOT respond to steroids, progressively worsens, associated with underlying carcinoma. Eczema = usually bilateral, involves the areola more than the nipple, responds to topical steroids. When in doubt, biopsy [9].
| Type | Most Common Cause | Other Differentials | Approach |
|---|---|---|---|
| Cyclical (worsens pre-menstrually, improves after menses) | Fibrocystic changes (most common) [2] | Normal physiological | Cyclical or bilateral diffuse pain: no imaging required; reassurance, conservative (NSAID) [2] |
| Non-cyclical (constant, no relationship to cycle) | Acute mastitis, fibroadenoma, inflammatory breast cancer [2] | Costochondritis (Tietze syndrome), fat necrosis, breast cyst (acute enlargement), diabetic mastopathy | Non-cyclical / unilateral / focal pain: USG / mammogram to exclude malignancy [2] |
Why is breast cancer usually painless? Most breast cancers grow insidiously within the parenchyma without acutely stretching the breast capsule or involving pain-sensitive structures. Exceptions include inflammatory breast cancer (dermal lymphatic obstruction → rapid oedema → stretching → pain) and locally advanced cancers invading the chest wall or intercostal nerves.
3. Pre-malignant Conditions (High-Risk Lesions)
These deserve special mention because they sit on the continuum between benign and malignant — they are not yet cancer but significantly increase the risk and may harbour occult malignancy [1][5]:
| Feature | Detail | Why / Mechanism |
|---|---|---|
| Definition | Proliferative lesions with cellular atypia arising from breast ducts (ADH) or lobules (ALH) [1] | Represent an intermediate step between normal hyperplasia and carcinoma in situ — cells show architectural distortion and cytological atypia but do not fully meet criteria for CIS |
| ADH pathology | Proliferation of uniform epithelial cells with monomorphic round nuclei filling part but not entirely the involved duct [1] | If the duct is completely filled with atypical cells → DCIS. ADH = partially involved |
| ALH pathology | Monomorphic, evenly spaced dyshesive cells filling part but not entirely the involved lobule [1] | If the lobule is completely filled → LCIS. ALH = partially involved |
| Cancer risk | ADH: 4–5× increased relative risk of invasive breast cancer [1]; ALH: similar risk [1] | Cells have already acquired some pre-malignant mutations; further hits can complete the transformation |
| Critical management point | If atypical hyperplasia found on core needle biopsy → excisional biopsy MUST be performed to rule out associated malignancy [1][2] | Core needle biopsy samples only a small portion of the lesion. There may be adjacent DCIS or invasive cancer that was missed by the needle. Excisional biopsy examines the entire lesion |
| If excision shows malignancy | Manage according to final histology (DCIS/IDC, LCIS/ILC) [1] | — |
| If excision shows no malignancy | Two options: (1) Surveillance with imaging + physical exam, or (2) Chemoprevention with tamoxifen [1] | Tamoxifen blocks ER → reduces oestrogen-driven proliferation → reduces risk of progression to invasive cancer |
| Ongoing management | Avoidance of OCP and HRT; yearly mammography; twice-yearly breast exam; SERMs or aromatase inhibitors [1] | Remove exogenous oestrogen sources that fuel proliferation |
Already covered in detail in the Classification section, but worth reiterating in the DDx context:
- DCIS: precursor to invasive ductal carcinoma (~1%/year). Mammographic microcalcifications. Manage with surgery ± RT ± endocrine therapy [2][3][7]
- LCIS: premalignant condition rather than true cancer [7][9] — a marker and precursor for bilateral invasive carcinoma (~1%/year). Usually an incidental finding. Classical LCIS → observation; pleomorphic LCIS → excision [2]
LCIS — A Premalignant Condition, NOT Cancer
Lobular carcinoma in-situ (LCIS) is really a premalignant condition rather than cancer [7][9]. Despite the name "carcinoma," classical LCIS is managed conservatively with observation because it is a marker of increased bilateral risk rather than a direct precursor at that specific site. This is fundamentally different from DCIS, which IS a direct precursor to ipsilateral IDC.
From the lecture slides (GC 181) [3]:
DDx of breast mass:
- Benign:
- Fibroadenoma
- Cysts
- Phyllodes tumour (Benign)
- Others (skin lesions etc)
- Malignant:
- Carcinoma
- In situ
- Invasive
- Phyllodes tumour (Malignant)
| Condition | Age | Consistency | Mobility | Tenderness | Key Distinguishing Feature | Cancer Risk |
|---|---|---|---|---|---|---|
| Fibroadenoma | 15–35 | Rubbery/firm | Most mobile | Non-tender | "Breast mouse"; regresses post-menopause | Simple: nil; Complex: increased |
| Breast cyst | Premenopausal | Soft, fluctuant | Mobile | ± Tender | Disappears on aspiration; anechoic on USG | Nil |
| Fibrocystic changes | Premenopausal | Nodular | — | Cyclical tenderness | Waxes and wanes with cycle | Depends on histology |
| Phyllodes tumour | > 40 | Firm | Mobile | Non-tender | Rapid growth; leaf-like histology | Can be malignant |
| Fat necrosis | Any | Hard | Variable | Non-tender | Mimics cancer clinically + radiologically; trauma history | Nil |
| Lipoma | Any | Soft | Mobile | Non-tender | Subcutaneous; fat density on imaging | Nil |
| Sclerosing adenosis | Any | Hard | — | — | Mimics cancer on imaging | Nil |
| ADH/ALH | Any | — | — | — | Usually incidental on biopsy; 5× risk | Yes (high risk) |
| DCIS | Any | Non-palpable | — | — | Microcalcifications on mammogram | Precursor to IDC |
| LCIS | Any | Non-palpable | — | — | Incidental finding; loss of E-cadherin | Marker/precursor bilateral |
| IDC | > 40 | Hard | Fixed | Non-tender | Irregular, spiculated, skin/nipple changes | — (IS cancer) |
| ILC | Older | Hard but diffuse | Variable | Non-tender | Difficult to detect (Indian file pattern); E-cadherin negative | — (IS cancer) |
| IBC | Any | Oedematous | — | Painful | Peau d'orange ≥ 1/3 breast; erythema; no fever | — (IS cancer, T4d) |
| Paget's disease | Any | ± Underlying mass | — | ± Tender | Unilateral nipple eczema; Paget cells on biopsy | ~80% underlying cancer |
| Mastitis | Lactating | Indurated | — | Very tender | Fever + leukocytosis; responds to antibiotics | Nil |
| Duct ectasia | Older ( > 50) | Subareolar mass | — | — | Multicoloured cheesy discharge; nipple retraction | Nil |
| Intraductal papilloma | Perimenopausal | Small/non-palpable | — | — | Bloody nipple discharge (most common cause) | Slightly increased |
| IGM | Young parous | Hard | — | Tender | Mimics cancer; diagnosis of exclusion; self-limiting | Nil |
High Yield Summary — Differential Diagnosis of Breast Cancer
-
DDx of breast lump by age: Young → fibroadenoma, cyst, fibrocystic changes. Old → carcinoma, Phyllodes tumour. Fat necrosis and lipoma at any age.
-
Fibroadenoma = most common benign tumour; "breast mouse" — highly mobile, rubbery, well-defined; hormonally dependent; simple type = no cancer risk.
-
Phyllodes tumour = fibroepithelial; can be malignant; metastasises via blood NOT lymphatics → ALND not required; excise with ≥ 1 cm margin.
-
Fat necrosis = mimics cancer clinically AND radiologically → core biopsy mandatory to differentiate.
-
Nipple discharge: Most common pathological cause = intraductal papilloma. Suspicious features: unilateral, single duct, bloody, spontaneous. Malignancy in 5–15% of pathological discharge (most commonly DCIS).
-
Paget's disease = unilateral nipple eczema + underlying cancer (~80%, usually HER2+). DDx from bilateral nipple eczema (dermatitis).
-
IBC vs. mastitis: IBC = peau d'orange ≥ 1/3 breast, erythema, NO fever/leukocytosis; Mastitis = fever + leukocytosis, responds to antibiotics.
-
ADH/ALH = high-risk lesions (4–5× risk); if found on core biopsy → MUST do excisional biopsy to rule out adjacent malignancy.
-
LCIS = premalignant condition, NOT true cancer; marker of bilateral risk; observe unless pleomorphic type.
-
Triple assessment (clinical + radiological + pathological) resolves virtually all diagnostic dilemmas.
Active Recall - Differential Diagnosis of Breast Cancer
References
[1] Senior notes: felixlai.md (Sections on fibroadenoma, breast cysts, fibrocystic changes, Phyllodes tumour, duct ectasia, mastitis, IGM, nipple discharge, ADH/ALH, Paget's disease, IBC, breast cancer clinical features) [2] Senior notes: maxim.md (Sections 8.2, 8.3, 8.6, breast carcinoma clinical features, DCIS/LCIS, benign breast tumours, inflammatory/non-inflammatory breast conditions) [3] Lecture slides: GC 181. Breast mass breast cancer; benign breast diseases; mammography; breast cancer screening.pdf (pp. 20, 33, 34) [4] Senior notes: maxim.md (ACP Consensus table on relative risk from benign breast disease) [5] Lecture slides: The Managment of breast cancer_Prof A Kwong 20_2_2020.pdf (pp. 30, 33) [7] Lecture slides: GC 181. Breast mass breast cancer; benign breast diseases; mammography; breast cancer screening.pdf (p. 33) [8] Senior notes: maxim.md (Sections 8.5 inflammatory/non-inflammatory breast conditions, Mondor's disease) [9] Lecture slides: GC 181. Breast mass breast cancer; benign breast diseases; mammography; breast cancer screening.pdf (p. 34)
Diagnosis of Breast Cancer — Diagnostic Criteria, Algorithm & Investigation Modalities
The diagnosis of breast cancer is never made on the basis of a single test. It relies on the Triple Assessment — a synergistic combination of three independent pillars, each compensating for the weaknesses of the others [10][11]:
| Pillar | Modality | Sensitivity (alone) |
|---|---|---|
| 1. Clinical | History and physical examination | 50–85% [10] |
| 2. Radiological | Mammography ± USG (± MRI) | ~90% [10] |
| 3. Pathological | FNA cytology or core needle biopsy (histology) | ~91% [10] |
Combined sensitivity of triple assessment: 99.6%; specificity: 93% [10].
Key rules [10]:
- Triple Assessment is positive if ANY one of the above is positive
- Triple Assessment is negative ONLY when ALL THREE are negative
- If findings do not all correlate → further investigations or monitoring is necessary
Why does this work so well? Each component catches what the others miss. A small tumour may be non-palpable clinically but visible on mammogram (microcalcifications). A tumour in dense breast tissue may be mammographically occult but palpable or visible on USG. And imaging alone cannot distinguish a benign from malignant lesion with certainty — tissue diagnosis resolves ambiguity. The triple assessment is essentially a Bayesian system: the post-test probability after three concordant negative results is extremely low.
2. Pillar 1 — Clinical Assessment
Already covered in detail in the Clinical Features section, but the key diagnostic elements are summarised here for completeness:
- Mass: onset, progression, cyclical changes
- Nipple: discharge (colour, unilateral/bilateral, single/multiple duct), retraction
- Skin: dimpling, peau d'orange, erythema, itchiness
- Constitutional symptoms: weight loss, bone pain, SOB (metastatic disease)
- Risk factor assessment: family history (BRCA — CA breast/ovary/prostate/pancreas), personal history (breast disease, chest RT), oestrogen exposure (menarche, menopause, parity, breastfeeding, COC/HRT)
- Positioning: 45° or sitting
- Exposure: Clavicle to upper abdomen, both breasts and axillae
Inspection:
- Size, symmetry, scars (3 Ss) [1]
- Skin changes: ulceration, dimpling, peau d'orange, erythema
- Nipple changes — the 5 Ds: Deviation, Discolouration, Dermatitis, Depression (retraction), Discharge [1]
Palpation of breast (start with normal side):
- Comment on: site, size, shape, border, surface, consistency, tenderness, mobility (to skin and to pectoralis muscle) [2]
- Include axillary tail
Palpation of axilla:
- Five groups: anterior, posterior, medial, lateral, apical [2]
- Comment on: number, site, size, consistency, tenderness, fixation [2]
Examination for metastatic disease [1]:
- Examine liver for hepatomegaly
- Examine bone for bone tenderness
- Examine lungs for effusion
- Neurological examination if brain metastasis suspected
3. Pillar 2 — Radiological Assessment
Mammography (mammo = breast; -graphy = imaging) uses low-dose X-rays to produce images of breast tissue. It is the primary imaging modality for early detection of breast cancer [1][2].
When to use mammography:
- Only for females > 35 years — because younger women have denser breasts (more glandular tissue, less fat), reducing mammographic sensitivity ("finding a white tumour in a white background") [2]
- Can be performed in pregnant women with shielding [2]
- Always perform bilateral mammography when breast cancer is suspected (to detect synchronous contralateral breast cancer) [2][4]
| View | Description | What it best shows |
|---|---|---|
| Craniocaudal (CC) | X-ray beam from above, breast compressed top-to-bottom | Inner vs. outer quadrant (mediolateral localisation) |
| Mediolateral oblique (MLO) | X-ray beam angled 45° from medial to lateral | Axillary tail, axillary lymph nodes, upper outer quadrant in detail; upper vs. lower half (line perpendicular to pectoralis major); pectoralis major involvement [2] |
Why these two views? Together they provide two perpendicular projections that allow triangulation of a lesion's position within the breast. The CC view shows medial-lateral location; the MLO view shows superior-inferior location and uniquely captures the axillary tail (where many cancers occur).
How to present a mammogram [2] (important!):
- Breast tissue appropriate for age (comment on density)
- Views: CC and MLO
- Location of mass — MLO: upper vs. lower half; CC: outer vs. inner quadrant
- Features of malignancy
Mammographic Features — Benign vs. Malignant [1]:
Mass features:
- Spiculated (stellate) opacity with irregular borders → suggests malignancy [1][2]
- Architectural distortion (e.g., tent sign) → suggests malignancy [2]
- Smooth, well-circumscribed mass → suggests benign
Calcification features [1]:
| Benign features | Malignant features | |
|---|---|---|
| Content | Rim-like calcification | Pleomorphic (irregular shapes and sizes) |
| Large coarse calcifications | ||
| Smooth round or oval calcifications | ||
| Distribution | Vascular and skin calcification | Linear branching microcalcifications (following duct distribution — cancer growing along ducts deposits calcium in a linear pattern) |
| Clustered microcalcifications ( > 5/mm²) [1] |
Why do cancers cause microcalcifications? In DCIS especially, malignant cells within ducts undergo necrosis (particularly in the comedo subtype). The necrotic debris undergoes dystrophic calcification — calcium phosphate deposits in dead tissue. These tiny calcifications ( < 0.5 mm) are often the earliest mammographic sign of DCIS, visible before a palpable mass develops. This is why mammographic screening saves lives — it catches cancer at the pre-invasive stage.
Other malignant mammographic signs [2]:
- Pectoralis major involvement (only assessable on MLO view)
- Skin thickening / tethering
- Nipple involvement
Mammographic advantages [2]:
- Gold standard for breast cancer screening
- More sensitive for calcifications than USG
- Less operator-dependent than USG
- Used for annual screening
Mammographic limitations [1][2]:
- Can only depict a mass as abnormal or suspicious but cannot make definitive diagnosis [1]
- Obscuration of borders and extent of primary tumour by dense breast tissues (reduced sensitivity in young, dense breasts) [1]
- Limited localisation; difficult to see chest wall and axilla [2]
- Radiation exposure (small dose)
| Feature | Detail |
|---|---|
| Role | Diagnostic follow-up of an abnormal screening mammogram; first imaging study in young women ( < 35) or women who are pregnant or lactating [1]; for all patients as adjunct [2] |
| Advantages | Improved sensitivity and specificity combined with mammogram, especially in young women with dense breast tissue [2]; distinguishes cysts from solid lesions; guides FNAC, biopsy, and clipping before neoadjuvant chemotherapy; assesses axillary lymph nodes [2]; no radiation |
| Limitations | NOT useful as screening (alone); operator-dependent; cannot pick up most calcifications [2] |
USG Features — Benign vs. Malignant [1]:
| Feature | Benign | Malignant |
|---|---|---|
| Shape | Wider-than-taller (ellipsoid) | Taller-than-wide (fir-tree shape) |
| Margin | Smooth margins; macrolobulation | Spiculated or angular margins; microlobulation |
| Echogenicity | Hyperechogenicity; thin echogenic capsule | Hypoechogenicity |
| Calcification | Absent | Internal calcification; posterior acoustic shadowing |
| Vascularity | Absent | Central vascularity |
Mnemonic for suspicious USG features: "SHIT CME" [2] — same features used for thyroid nodule assessment: Solid, Hypoechoic, Irregular margins, Taller-than-wide, Calcification (micro), Microlobulation, Extra-thyroidal extension (in breast context = chest wall invasion).
USG assessment of axillary lymph nodes [2]:
- Suspicious LN feature: loss of fatty hilum (normal LN has a central hyperechoic fatty hilum; metastatic replacement obliterates this)
Roles of USG in characterising masses [1]:
- Simple cyst (anechoic, posterior acoustic enhancement, well-defined walls) → no further intervention due to low cancer risk
- Indeterminate cyst → aspiration under USG guidance
- Intracystic mass → aspiration or biopsy
- Solid mass → characterise as benign or malignant; absence of flow on Doppler does NOT exclude malignancy [1]
| Feature | Detail |
|---|---|
| Characteristics | High sensitivity but low specificity; better characterisation of soft tissues without radiation [1] |
| Routine use | NOT routinely performed in the workup of an undiagnosed breast mass [1][2] |
| Concern | Unnecessary biopsies may be performed due to false positives (low specificity) [2] |
Indications for breast MRI [1][2]:
- Equivocal results from mammogram or USG
- Assessment of patients with breast implants (implants obscure tissue on mammogram)
- Identify patients with clinically occult tumour presenting with positive axillary LN (unknown primary) [2]
- Suspected multicentric or bilateral malignancy, especially invasive lobular carcinoma (ILC) (ILC is notorious for being mammographically and clinically occult due to its diffuse infiltrating pattern)
- Determine extent of disease accurately, especially chest wall involvement (not fully included on mammographic projections)
- Identify extent of residual disease after excision with positive margins
- Pre-operative evaluation to improve surgical planning (help surgeons obtain clean margins)
- Monitor results of neoadjuvant therapy (assess tumour shrinkage)
- Screening in high-risk patients (genetic predisposition, e.g., BRCA carriers)
- Paget's disease with negative mammogram [2]
MRI malignant features [1]:
- Spiculated or irregular margins
- Rim-like enhancement
- Heterogeneous internal enhancement
- Enhancing internal septa
- More rapid uptake of contrast is characteristic of malignant mass (nearly all invasive breast carcinomas enhance on gadolinium-contrast MRI; some benign lesions also enhance — hence low specificity) [1]
BI-RADS is a standardised reporting system applicable to both mammographic and ultrasound findings [1][10][11]. It translates subjective radiological impressions into a universally understood risk category that dictates the next management step:
| BI-RADS Category | Assessment | Likelihood of Malignancy | Management |
|---|---|---|---|
| 0 | Incomplete assessment | N/A | Recall for additional imaging [1][10] |
| 1 | Negative (normal) | 0% | Routine screening [1][10] |
| 2 | Benign | 0% | Routine screening [1][10] |
| 3 | Probably benign | > 0% but ≤ 2% ( < 2% malignant) | Short-interval (6-month) follow-up with surveillance mammography [1][10] |
| 4 | Suspicious abnormality | > 2% to < 95% | Tissue diagnosis (biopsy) [1][10] |
| 4A: low suspicion | *** > 2% to ≤ 10%*** | ||
| 4B: moderate suspicion | *** > 10% to ≤ 50%*** | ||
| 4C: high suspicion | *** > 50% to < 95%*** | ||
| 5 | Highly suggestive of malignancy | ≥ 95% | Tissue diagnosis (biopsy) [1][10] |
| 6 | Known biopsy-proven malignancy | N/A | Surgical excision when clinically appropriate [1][10] |
BI-RADS — The Decision-Maker
BI-RADS is the bridge between imaging and action. The key thresholds to remember:
- BI-RADS 3 = probably benign → 6-month follow-up (don't biopsy yet, but don't ignore)
- BI-RADS 4 = suspicious → BIOPSY (this is where most diagnostic biopsies are triggered)
- BI-RADS 5 = almost certainly malignant → BIOPSY (but still need tissue confirmation before definitive surgery)
- BI-RADS 6 = already proven → proceed to definitive treatment planning
Once breast cancer is diagnosed, staging investigations are needed to determine the extent of disease [1][2][4]:
| Investigation | Target | When to perform |
|---|---|---|
| CXR | Lung metastasis | All patients with invasive cancer |
| USG abdomen | Liver metastasis | Baseline; if LFT abnormal |
| Bone scan (99mTc-MDP) | Bone metastasis | If symptoms (bone pain), elevated ALP/Ca²⁺, or locally advanced disease |
| PET-CT | Whole-body staging — detects distant metastases | Patients with stage IIIA or above regardless of symptoms; patients with symptoms of metastasis [1][4] |
| CT abdomen | Liver, adrenal, ovarian metastasis | When further characterisation needed |
| CT or MRI brain | Brain metastasis | If neurological symptoms present |
PET-CT indications [1]:
- Workup for metastasis in patients presenting with locally advanced (T3 or greater, N2/3, M0) or inflammatory breast cancer
- Patients presenting with symptoms of metastasis
- Patients with stage IIIA or above regardless of symptoms
- LFT — liver metastasis (elevated transaminases, ALP, bilirubin)
- Calcium and phosphate (CaPO₄) — bone metastasis (hypercalcaemia from osteolytic metastases)
- Tumour markers: CA 15.3, CEA — not diagnostic but useful for monitoring treatment response and recurrence [4]
4. Pillar 3 — Pathological Assessment (Tissue Diagnosis)
This is the definitive pillar. No matter how suspicious the clinical and radiological findings, you cannot definitively diagnose breast cancer without tissue confirmation [10].
| Method | Needle Size | What It Provides | Advantages | Disadvantages | When to Use |
|---|---|---|---|---|---|
| FNAC (Fine Needle Aspiration Cytology) | 21–23G | Cytological diagnosis (individual cells) | No LA needed, smaller needle, quick, less painful [2] | Cannot assess architecture (cannot distinguish in-situ from invasive); cannot determine grade or receptor status [2] | Low-risk lesions (e.g., non-palpable mass, equivocal mammogram); simple cysts [2] |
| Core needle biopsy (CNB) — FIRST LINE [2] | 9–14G | Histological diagnosis (tissue core with architecture) | Architectural assessment, tumour grading, receptor status (ER/PR/HER2) [2] | Requires local anaesthesia, larger needle, more painful | BI-RADS 4 or above; any suspicious lesion [2] |
| Excisional biopsy | N/A (surgical) | Complete removal of lesion | Definitive; complete architectural assessment | Invasive procedure, may alter breast cosmesis | When core biopsy reveals a suspicious but not diagnostic lesion; clinical-pathological discordance [2] |
FNAC vs. Core Biopsy — Why Core Biopsy is First Line
Think of it this way: FNAC gives you individual cells — like looking at scattered leaves. Core biopsy gives you a tissue core — like looking at a branch with leaves still attached. To determine whether cancer is in-situ (confined within the duct/lobule) or invasive (breached through the basement membrane), you NEED to see the architecture (the relationship of cells to the basement membrane). FNAC cannot provide this. Core biopsy can also provide tumour grade and receptor status (ER, PR, HER2) — essential for treatment planning.
If the lesion is cystic:
- Lump disappears after aspiration + clear fluid → no further investigation needed
- Residual thickening after aspiration OR blood-stained fluid → proceed to core biopsy
If the lesion is solid (FNAC result):
- Benign → observe or excise
- Atypical → core needle biopsy (need architecture)
- Malignant → treat as cancer
For non-palpable masses detected on screening:
| Guidance Method | Description |
|---|---|
| USG-guided | Real-time visualisation; most commonly used |
| Stereotactic (X-ray guided) | Uses mammographic coordinates to target microcalcifications not visible on USG |
| Tomosynthesis-guided (3D mammogram) | Multiple X-ray projections; better localisation than 2D stereotactic |
| MRI-guided | For lesions only visible on MRI |
| Vacuum-assisted core biopsy | Increases yield by obtaining larger tissue samples through suction [2] |
When excisional biopsy is needed for a non-palpable lesion, the surgeon needs guidance to find it:
| Technique | Description | Considerations |
|---|---|---|
| Hook-wire localisation (HWL) | Wire with hook inserted into the lesion under mammographic/USG guidance pre-operatively | Problems: extensive normal tissue removal, wire protrudes outside skin (risk of dislodgement), risk of broken wire [2] |
| Radioactive seed localisation (RSL) | ¹²⁵I-labelled titanium seed inserted 0–5 days prior to surgery [2] | More convenient timing; seed stays in place |
| Radio-opaque lesion localisation (ROLL) | ⁹⁹ᵐTc-labelled albumin-based colloid injected within 24h of surgery [2] | Used in centres with nuclear medicine facilities |
| Magseed localisation | Non-radioactive magnetic seed [2] | No radiation handling; can be placed weeks before surgery |
| On-table USG | Intra-operative real-time ultrasound guidance [2] | Useful for USG-visible lesions |
Every newly diagnosed breast cancer MUST be tested for ER, PR, and HER2 status — for both therapeutic and prognostic purposes [1][11]:
| Receptor | How Assessed | Positive Definition | Why It Matters |
|---|---|---|---|
| ER (Oestrogen Receptor) | Immunohistochemistry (IHC) | ER positive: ER in > 1% of tumour cells by IHC [1] | Determines eligibility for endocrine therapy (tamoxifen, aromatase inhibitors) |
| PR (Progesterone Receptor) | IHC | PR positive: PR in > 1% of tumour cells by IHC [1] | PR expression is oestrogen-driven → confirms functional ER pathway; PR+ further refines prognosis within HR+ group |
| HER2 | IHC and/or FISH | IHC 3+: uniform intense membrane staining of ≥ 10% of tumour cells [1] OR FISH positive: HER2/CEP17 ratio ≥ 2.0 OR ratio < 2.0 with average HER2 copy number ≥ 6 signals/cell [1] | Determines eligibility for anti-HER2 therapy (trastuzumab); prognostic (HER2+ = more aggressive but targetable) |
| Ki67 | IHC | Percentage of proliferating cells; cut-off varies (typically ≥ 20% = high) | Distinguishes Luminal A (low Ki67) from Luminal B (high Ki67); high Ki67 = more aggressive but more chemo-responsive |
HER2 biochemistry and clinical significance [1]:
- HER2 = Human Epidermal growth factor Receptor 2 (erbB2 gene)
- HER2 gene amplification is the primary mechanism for HER2 protein overexpression
- HER2 is a transmembrane tyrosine kinase receptor. Attachment of epidermal growth factor to HER2 receptors stimulates proliferation of breast cancer cells
- HER2 protein overexpression in breast cancer is associated with [1]:
- Higher risk of recurrence
- Higher mortality
- Relative resistance to hormonal treatment
- Less benefit from some forms of chemotherapy
IHC Scoring for HER2:
| Score | Interpretation | Action |
|---|---|---|
| 0 or 1+ | Negative | No anti-HER2 therapy |
| 2+ | Equivocal | Reflex FISH testing to determine gene amplification |
| 3+ | Positive | Anti-HER2 therapy indicated |
Sample pathology report interpretation [11]: A report stating "ER Negative, PR Negative, HER2 Score 0" with Ki67 60% describes a triple-negative breast cancer with high proliferative index — the most aggressive subtype with the fewest targeted therapeutic options. E-cadherin positive confirms ductal (not lobular) differentiation. Negative p63 staining confirms absence of myoepithelial cells around invasive foci, confirming invasiveness [11].
5. Diagnostic Criteria — Specific Entities
There is no single "diagnostic criterion" — it is diagnosed by the combination of:
- Clinical suspicion (hard, irregular, fixed mass ± skin/nipple changes)
- Radiological suspicion (BI-RADS 4 or 5)
- Histological confirmation on core needle biopsy showing malignant epithelial cells that have invaded through the basement membrane into the stroma
- Usually asymptomatic and non-palpable — detected by mammographic microcalcifications (linear branching or clustered pleomorphic) [1]
- Occasionally palpable (especially if large or high-grade)
- Histology: Malignant cells within TDLU with ductal predominance, WITHOUT invasion through basement membrane
- Grading: Low, Intermediate, High Grade [5][7]
- High-grade (comedo) DCIS: central necrosis → dystrophic calcification → the characteristic mammographic microcalcifications
- Prognostic: Van Nuys Prognostic Index (considers size, margin width, grade/necrosis, age) [2] — guides treatment intensity
- NO symptoms or findings on physical examination AND mammography in most cases [1]
- Incidental finding on breast biopsy performed for another reason [1]
- Usually multifocal + multicentric + bilateral [1]
- Easily missed by mammography (rarely associated with microcalcifications) [1]
- E-cadherin NEGATIVE on IHC — this stain is used to clarify borderline cases between DCIS and LCIS (DCIS is E-cadherin positive; LCIS is negative due to loss of this cell-cell adhesion molecule) [1]
- LCIS is NOT considered cancer or a pre-invasive lesion by itself — removed from AJCC staging system. Rather, it is an indicator of increased risk (~1%/year) for cancer in either breast [1]
Diagnostic criteria (all must be met):
- Rapid onset of breast erythema, oedema, peau d'orange or warm breast ± underlying palpable mass
- Erythema occupying at least 1/3 of the breast
- Duration of history no more than 6 months
- Pathological confirmation of invasive carcinoma (skin punch biopsy showing tumour emboli in dermal lymphatics is characteristic but not required)
- Full-thickness wedge biopsy of the nipple showing Paget cells (malignant intraepithelial adenocarcinoma cells within the nipple epidermis)
- Mammography mandatory to look for associated mass and exclude synchronous cancers or widespread calcification [1]
After triple assessment, all three pillars must be reviewed together for concordance [10]:
| Scenario | Interpretation | Action |
|---|---|---|
| All three concordant BENIGN | True negative; cancer extremely unlikely | Routine follow-up |
| All three concordant MALIGNANT | True positive; diagnosis established | Proceed to staging and treatment |
| Any discordance (e.g., clinically suspicious but biopsy benign) | Findings do not correlate → further investigation needed [10] | Repeat biopsy (preferably excisional), consider MRI, MDT discussion |
| Triple assessment positive if ANY one is positive [10] | Cannot dismiss malignancy | Must resolve with tissue diagnosis |
The Golden Rule of Triple Assessment
Never dismiss a clinically suspicious lump just because the mammogram or initial biopsy is negative. The sensitivity of each component alone is imperfect. If there is discordance between any two pillars, you must investigate further — usually with repeat/excisional biopsy. Triple Assessment is positive if ANY one of the three is positive [10].
| Investigation | Key Benign Findings | Key Malignant Findings | Role |
|---|---|---|---|
| Mammography | Smooth round mass, rim-like calcification, large coarse calcification | Spiculated mass, pleomorphic microcalcifications, linear branching calcifications, clustered calcifications > 5/mm², architectural distortion, skin thickening | Primary screening and diagnostic imaging |
| USG | Wider-than-taller, smooth margins, hyperechoic, thin capsule, no vascularity; simple cyst = anechoic + posterior enhancement | Taller-than-wide, spiculated/angular margins, hypoechoic, internal calcification, posterior acoustic shadowing, central vascularity | Adjunct to mammography; first-line in young women; guide biopsies |
| MRI | Smooth margins, slow uniform enhancement | Spiculated margins, rim-like enhancement, heterogeneous internal enhancement, rapid contrast uptake | Not routine; for specific indications (ILC extent, occult primary, implants, treatment monitoring) |
| Core biopsy | Normal/benign histology (fibroadenoma, fibrocystic changes) | Invasive carcinoma with grade, receptor status (ER/PR/HER2/Ki67) | Definitive diagnosis; provides all information for treatment planning |
| FNAC | Benign cells; cyst fluid | Malignant cells (but no architecture) | Quick assessment; simple cysts; low-risk lesions |
| PET-CT | No FDG-avid lesions | FDG-avid primary and metastatic lesions | Staging for locally advanced/metastatic disease |
| Bone scan | Normal uptake | Multifocal increased uptake (hot spots) | Detecting skeletal metastases |
| Bloods | Normal | Elevated ALP/Ca (bone met), elevated transaminases (liver met), elevated CA15.3/CEA | Staging and monitoring |
High Yield Summary — Diagnosis of Breast Cancer
-
Triple Assessment = Clinical + Radiological + Pathological. Combined sensitivity 99.6%, specificity 93%. Positive if ANY one is positive. Negative only when ALL three are negative.
-
Mammography: Primary imaging for > 35 years; CC + MLO views; malignant features = spiculated mass, pleomorphic/linear branching microcalcifications, architectural distortion. Not sensitive in dense breasts.
-
USG: First-line for < 35 years, pregnant, lactating; distinguishes cyst from solid; guides biopsy. Malignant = taller-than-wide, hypoechoic, spiculated, central vascularity.
-
BI-RADS: Standardised reporting. BI-RADS 4–5 → tissue diagnosis (biopsy). BI-RADS 3 → 6-month follow-up.
-
Core needle biopsy = first-line for tissue diagnosis. Provides architecture, grade, receptor status. FNAC only for low-risk/cystic lesions.
-
Receptor testing (ER/PR/HER2/Ki67) is mandatory for all new diagnoses — determines molecular subtype and guides therapy.
-
HER2: IHC 3+ or FISH-amplified = positive. IHC 2+ = equivocal → reflex FISH. HER2+ = higher recurrence, higher mortality, but targetable with trastuzumab.
-
MRI: High sensitivity, low specificity. Not routine. Indications: occult primary with positive axillary LN, ILC extent, implants, treatment response monitoring.
-
Staging: CXR (lung), USG abdomen (liver), bone scan (bone), PET-CT (stage ≥ IIIA or symptomatic), bloods (LFT, Ca/PO₄, CA15.3, CEA).
-
Discordance between any pillars → further investigation (repeat/excisional biopsy). Never dismiss a suspicious lesion on incomplete assessment.
Active Recall - Diagnosis of Breast Cancer
References
[1] Senior notes: felixlai.md (Sections on mammography, ultrasound, MRI, PET-CT, histopathological diagnosis, receptor testing, DCIS, LCIS, clinical examination, IBC diagnostic criteria, Paget's disease) [2] Senior notes: maxim.md (Sections 8.3 clinical and radiological assessment, pathological assessment, FNAC approach, excisional biopsy localisation techniques, BI-RADS, DCIS/LCIS, staging investigations) [4] Senior notes: maxim.md (Staging investigations — bloods, tumour markers, imaging) [5] Lecture slides: The Managment of breast cancer_Prof A Kwong 20_2_2020.pdf (p. 33 — histological types) [7] Lecture slides: GC 181. Breast mass breast cancer; benign breast diseases; mammography; breast cancer screening.pdf (p. 33 — breast cancers classification) [10] Lecture slides: The Managment of breast cancer_Prof A Kwong 20_2_2020.pdf (p. 10 — Triple Assessment) [11] Lecture slides: GC 181. Breast mass breast cancer; benign breast diseases; mammography; breast cancer screening.pdf (p. 31 — sample pathology report); The Managment of breast cancer_Prof A Kwong 20_2_2020.pdf (p. 16 — BI-RADS)
Management of Breast Cancer — Algorithm, Treatment Modalities, Indications & Contraindications
Before diving into specifics, understand the two fundamental goals of breast cancer treatment and the therapeutic "weapons" available [12][13]:
Goals:
- Locoregional control → Surgery + Radiotherapy
- Systemic control → Chemotherapy + Hormonal therapy + Targeted therapy
Choice of treatment depends on [12]:
- Type of initial surgical treatment
- Age / menopausal status
- Tumour size
- Number of involved lymph nodes
- Tumour grade
- Oestrogen / Progesterone receptor status
- HER2 gene amplification
- Gene signatures
Think of it as two parallel battlefields: the local battlefield (the breast and axilla — controlled by the surgeon and radiation oncologist) and the systemic battlefield (micrometastatic disease anywhere in the body — controlled by the medical oncologist with drugs). Both must be addressed for cure.
3. Surgical Management — The Local Battlefield
Surgery for breast cancers has two components that are planned independently [13][14]:
- Breast surgery — what to do with the primary tumour
- Axillary surgery — what to do with the lymph nodes
- Oncological outcome (complete removal of cancer with negative margins)
- Cosmetic outcome (preserve as much normal tissue as possible)
Surgical strategy combinations [14]:
- Mastectomy + SLNB
- Mastectomy + Axillary Dissection (MRM)
- Breast Conserving Surgery (BCS) + SLNB
- BCS + Axillary Dissection
BCT = Breast Conservation Surgery (BCS/Wide Local Excision/Lumpectomy) + Post-operative breast irradiation [1][12]
This is the preferred approach when feasible because it allows women with invasive breast cancer to preserve the breast with good cosmetic result [1] while achieving equivalent survival to mastectomy (proven in multiple randomised trials — NSABP B-06, Milan I).
Principles:
- Complete surgical removal of tumour with negative surgical margins [1]
- Negative margin defined as "no ink on tumour" [2] — meaning no tumour cells at the inked cut surface
- Adjuvant radiotherapy is COMPULSORY in BCT to eliminate subclinical foci of disease in the ipsilateral breast [1]
Selection criteria for BCS [1]:
- Tumour ≤ T2 ( ≤ 5 cm) without chest wall or skin involvement
- Appropriate tumour-to-breast ratio (cosmetically acceptable result after excision)
- Tumour is NOT multicentric
- Absence of distant metastasis
- Patient MUST agree to post-operative radiotherapy
Contraindications to BCS [1][2][12] (must know!):
| Contraindication | Why |
|---|---|
| Multicentric disease (different quadrants) [12] | Cannot encompass multiple separate tumour foci in a single excision with acceptable cosmesis |
| High tumour-to-breast ratio ( > 20%) [2][12] | BCS will not result in a good cosmetic result [12]; adequate resection would cause significant deformity (can be downstaged by neoadjuvant chemo) [2] |
| Diffuse malignant-appearing microcalcifications on imaging [1][2] | Suggests widespread DCIS throughout the breast; cannot achieve clear margins with limited excision |
| Persistently positive margins after multiple re-excision attempts [1][2] | Indicates diffuse/extensive disease not amenable to conservation |
| Inflammatory breast cancer [2] | Tumour cells diffusely infiltrate dermal lymphatics throughout the breast → cannot achieve local control with limited excision |
| Tumour too close to or involving NAC [2][12] | Cancer underneath nipple or nipple involvement [12] |
| Where radiation therapy is contraindicated [12]: | |
| — Pregnancy (1st/2nd trimester) [12] | Radiation is teratogenic; possible in 3rd trimester (defer RT until after delivery) [1] |
| — Prior history of therapeutic radiation to the affected chest wall/breast [1][12] | Combined doses would be excessively high → unacceptable toxicity |
| — Connective tissue disease (e.g., SLE, scleroderma, Sjögren's) [2][12] | Poor skin/tissue healing; fistula formation; abnormal fibrotic response to radiation |
| Patient choice (refuses adjuvant RT) [2] | BCT without RT has unacceptably high local recurrence rate |
| Prophylactic intent (e.g., BRCA carrier) [2] | Prophylactic mastectomy removes all breast tissue to maximise risk reduction |
Relative contraindication [12]:
- Multifocal disease (same quadrant) — may still be resectable in a single excision if feasible
Indications [2]:
- Contraindication to BCS (any of the above)
- Patient choice (desire to avoid post-operative radiation, further screening, or biopsy)
- Prophylaxis for patients with BRCA1/2 mutations or hereditary breast-ovarian syndrome [1]
- Similar efficacy to BCS (mastectomy does not improve survival over BCT — it simply removes more tissue) [2]
Types of Mastectomy:
| Type | What Is Removed | What Is Preserved | Indications | Contraindications |
|---|---|---|---|---|
| Simple (total) mastectomy | All breast tissue + nipple-areolar complex (NAC) | Axillary contents, pectoral muscles | Clinically node-negative (SLNB performed separately) [1] | — |
| Skin-sparing mastectomy | Breast parenchyma + NAC | Overlying breast skin envelope + inframammary fold [1] | Therapeutic mastectomy with immediate reconstruction (DCIS, Stage I–III invasive); prophylactic mastectomy [1] | Inflammatory breast cancer (cancer cells in dermal lymphatics — keeping the skin risks leaving cancer behind) [1] |
| Nipple-areolar sparing mastectomy | Breast parenchyma + major ducts from nipple lumen | NAC dermis and epidermis + skin envelope [1] | Small-to-moderate breasts with minimal ptosis; tumour < 2 cm with tumour-to-NAC distance > 2 cm; prophylactic mastectomy [1] | Inflammatory breast cancer; Paget's disease of the nipple; nipple changes or discharge [1] |
| Modified radical mastectomy (MRM) | Whole breast + overlying skin + axillary LN (Level I + II) [2] | Pectoral muscles | Clinically node-positive disease [2] | — |
| Radical mastectomy (Halsted) | Breast + skin + pectoralis major + axillary LN | — | Not performed in modern practice due to excessive morbidity without survival benefit [2] | — |
Why did we move away from radical mastectomy? Halsted in the 1890s believed cancer spread in an orderly centrifugal fashion — remove more tissue, better cure. The Fisher hypothesis (1970s) revolutionised thinking: breast cancer is a systemic disease from early on, and local control (whether by mastectomy or BCT + RT) combined with systemic therapy determines survival, not the extent of surgery alone. This is why BCT achieves equivalent survival to mastectomy.
Practical surgical details [2]:
- Drains: Jackson-Pratt drain (closed suction) — placed through separate stab wounds inferolateral to main incision; ± 2nd drain at axilla if MRM
- Remove drains if output < 30 mL/day × 2 days [2]
- Locally advanced cases: may require removal of part of pectoralis muscle for margin; place clips in anticipation of subsequent RT; positive margin → adjuvant RT [2]
| Timing | Detail |
|---|---|
| Immediate reconstruction | Performed at the time of mastectomy. Advantages: superior cosmetic results, reduced surgical costs, reduced psychosocial impact of breast loss, spares another surgery [1] |
| Delayed reconstruction | Indicated in patients requiring post-operative radiotherapy [1] (RT causes fibrosis and contracture of reconstructed tissue, compromising cosmetic result) |
Methods:
- Autologous tissue flaps — e.g., TRAM (transverse rectus abdominis myocutaneous) flap, DIEP (deep inferior epigastric perforator) flap, latissimus dorsi flap
- Implant-based [13]:
- One-stage: Permanent implant inserted at time of mastectomy
- Two-stage: Tissue expander placed at mastectomy → gradually inflated → replaced with permanent implant [1]
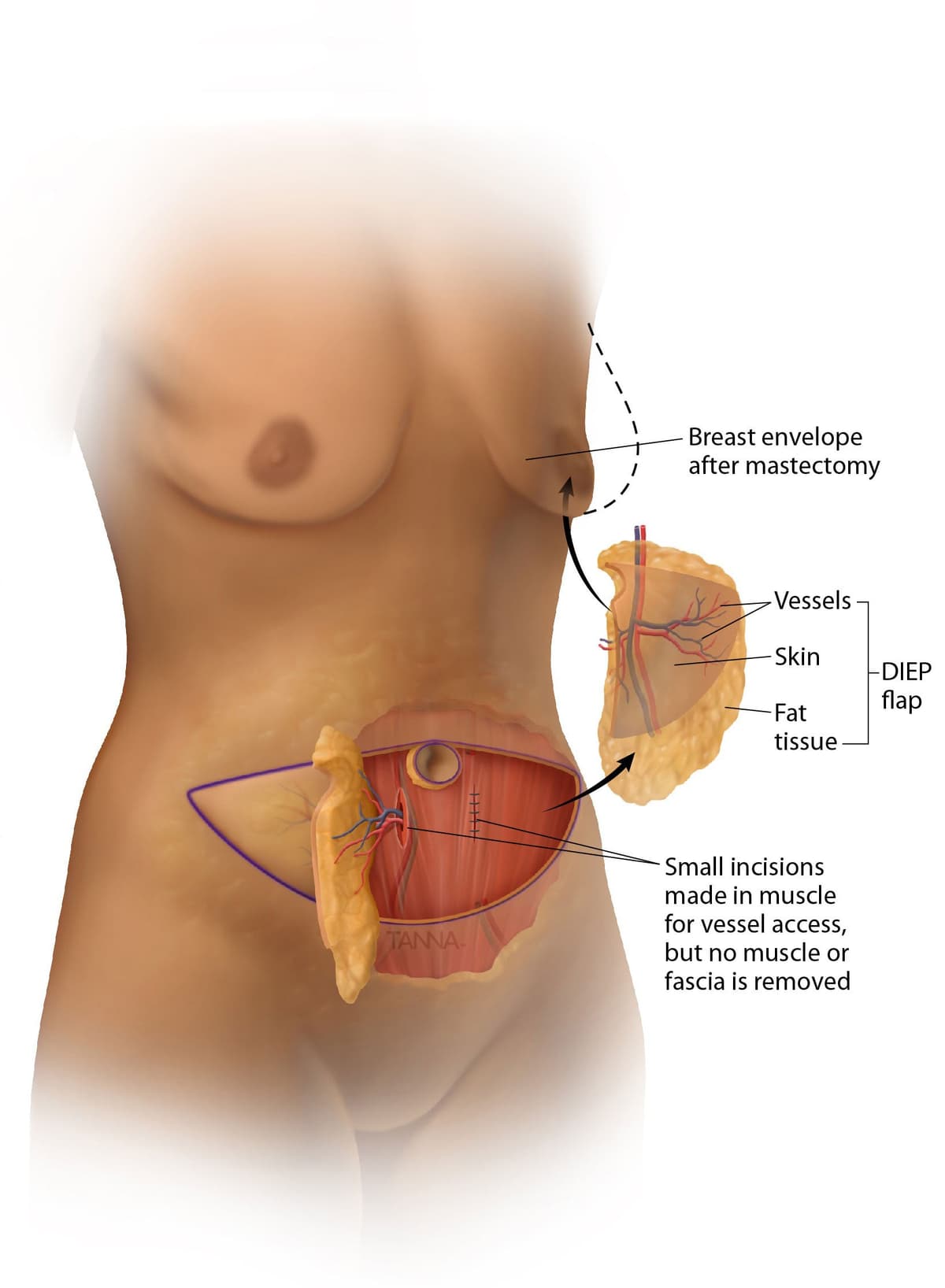
4. Axillary Management — The Lymph Node Question
The axilla is managed independently from the breast. The key question is: Are the lymph nodes involved? [1]
The sentinel LN is the first draining LN group — the "gatekeeper" of the rest of the axillary LN [2][12].
Purpose: To find the first lymph node which drains the tumour [12]. If the sentinel node is negative, the remainder of the axilla is overwhelmingly likely to be negative too, and the patient is spared the morbidity of full axillary dissection.
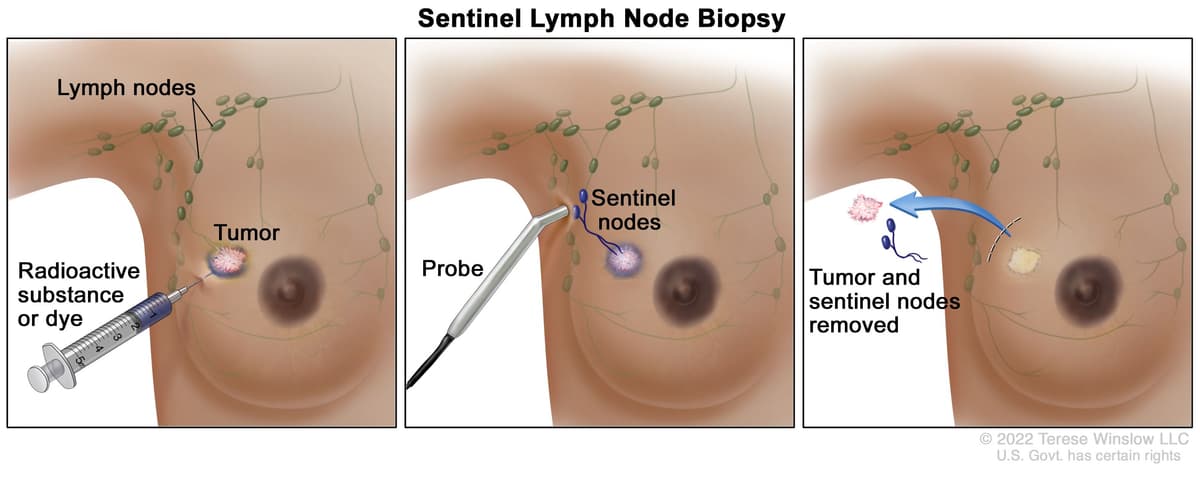
- Early breast cancer with clinically negative nodes (for staging the axilla with less morbidity than ALND)
- Early stage (T1 or T2) cancer [1]
- DCIS with planned mastectomy (because SLNB cannot be done after mastectomy if occult invasive cancer is found — the lymphatic drainage is permanently altered) [1]
- DCIS with suspicious features (suspicion of harbouring synchronous invasive cancer: > 5 cm, palpable mass, high-grade/comedo) [1]
Contraindications [1]:
- Absolute:
- Clinically positive nodes (should proceed directly to ALND)
- Inflammatory breast cancer (T4d) (should be treated with ALND)
- Relative:
- Tumour > 5 cm (T3)
- Tumour with chest wall or skin involvement (T4a–T4c)
- Previous breast or axillary procedures (disruption of lymphatic drainage → increased false-negative rate)
- Dual tracer injection to intradermal / subareolar / intratumoral region [2]:
- Injection should not be close to axilla (avoids interference) and lateral to previous scars (may block lymphatic drainage) [2]
- Remove maximum 3–4 sentinel LN [2] (HK practice: up to 4) [1]
- Frozen section of the LN to be done intraoperatively [12] — if positive, can proceed to ALND in the same operation
SLN Identification [1]:
- By blue dye: any blue node or any non-blue node with blue afferent lymphatic
- By radioactivity: remove the node with highest radioactive count (gamma probe); subsequent nodes removed by the "10% rule" — all nodes with > 10% of the ex vivo count of the hottest node should also be removed [1]
Results and management [2]:
| SLNB Finding | Management |
|---|---|
| No metastasis | No further axillary surgery |
| Micrometastasis (≤ 2 mm) | No further axillary surgery |
| Macrometastasis ( > 2 mm) × 1–2 LN, with planned RT (BCS) | Completion ALND NOT required (per ACOSOG Z0011 trial) [12] — with Z0011 study, for suitable patients with minimal tumour load in the axillary LN and receiving breast conservation surgery and radiation, axillary dissection may not be necessary [12] |
| Macrometastasis × ≥ 3 LN | Axillary dissection [2] |
| Extra-nodal extension | Axillary dissection [2] |
| Sentinel LN not found | Axillary dissection [2] |
Limitations of SLNB [2]:
- False-negative rate: 9.8% (NSABP B-32 trial)
- Only 75% of lymphatics drain to axilla (some drain to internal mammary chain)
- Skip metastases possible
New advancements [2]: ICG (indocyanine green fluorescence), SPIO (supra-paramagnetic iron oxide) — non-radioactive alternatives.
- Clinically positive nodes (by palpation / USG axilla)
- Positive sentinel LN (per criteria above — all patients receiving mastectomy without radiation with any macrometastasis; > 2 positive SLNs in BCT patients)
- Inflammatory breast cancer (T4d) [2]
- Standard: Level I (lateral to pec minor) + Level II (deep to pec minor) — typically yields ≥ 10 lymph nodes [1]
- Level III dissection is NOT indicated unless grossly positive Level III nodes — increases morbidity significantly without improving survival; skip metastasis to Level III is rare [1][2]
Structures to preserve [1]:
- Thoracodorsal artery, vein, and nerve
- Long thoracic nerve
Complications of ALND [2] — remember the 4 nerves:
| Complication | Mechanism |
|---|---|
| Seroma | Disruption of lymphatic channels → fluid collection |
| Long thoracic nerve injury | Winged scapula (denervation of serratus anterior → inability to protract scapula → medial border protrudes) |
| Thoracodorsal nerve injury | Weakness of latissimus dorsi → weak adduction and internal rotation of shoulder |
| Medial pectoral nerve injury | Denervation of pectoralis major → wasting |
| Intercostobrachial nerve injury | Paraesthesia of axilla, medial arm, and lateral chest wall (this is a sensory nerve — T2 intercostal branch that crosses the axilla; almost always sacrificed in ALND) |
| Upper limb lymphoedema | Disruption of axillary lymphatic drainage → chronic limb swelling; management = pneumatic compression device [2] |
| Upper limb lymphangiosarcoma | Stewart-Treves syndrome — rare malignant transformation in chronically lymphoedematous limb (years after ALND) [2] |
5. Adjuvant (Systemic) Therapy — The Systemic Battlefield
All patients must be assessed for adjuvant therapies [2]. The decision depends on:
- Patient factors: age, menopausal status, medical comorbidities (especially cardiac and renal), family/social situation
- Tumour factors: size, axillary LN status, ER/PR/HER2 status, tumour histology and grading (Ki67), resection margin, operation performed (BCS vs MRM), genomic studies
5.1 Chemotherapy
Given before surgery in operable disease [12][15]:
- Reduce size of tumour → increase breast conservation surgery rate [15]
- Improve local control and long-term outcome [15]
- Especially if complete pathological response (pCR) — likely to translate to improvement of long-term outcome [15]
- Provide prognostic information (response to neoadjuvant therapy predicts outcome) [2]
- Allow addition of different adjuvant regimens [2]
- Locally advanced (T3 or Stage III) cancer that is inoperable [2]
- Large operable tumour that may be converted from mastectomy to BCS [2]
- Limited node-positive (cN1) cancer — conversion from cN1 to cN0 may potentially avoid ALND and convert to SLNB with regional nodal irradiation [1]
- HER2-positive or triple-negative breast cancer — these subtypes are expected to receive chemotherapy at some point and are associated with higher likelihood of response (higher pCR rates) [1]
Practical point [2]: Mark the location of tumour with metal clip / radioactive seed before starting neoadjuvant therapy — in case the tumour becomes undetectable after treatment (excellent response), the surgeon needs to know where to operate.
Disadvantages of neoadjuvant therapy [2]:
- No proven overall survival benefit compared to adjuvant therapy (same drugs, different timing)
- May upstage if no response to treatment (tumour grows during treatment → opportunity for surgery may be lost)
Current subtype-specific approach [19][20]:
- TNBC stage II–III: pembrolizumab with neoadjuvant chemotherapy, followed by adjuvant pembrolizumab after surgery. Immune-related adverse events can be severe/permanent, and there are no data supporting routine pembrolizumab combined with adjuvant capecitabine or olaparib.
- TNBC cT1a/bN0: do not routinely offer neoadjuvant therapy outside a clinical trial.
- HER2-positive, node-positive or high-risk node-negative: neoadjuvant chemotherapy plus trastuzumab; pertuzumab may be added with trastuzumab.
- HR-positive / HER2-negative: neoadjuvant chemotherapy can be used when chemotherapy is already indicated; post-menopausal patients may receive neoadjuvant aromatase inhibitor therapy to improve local treatment options.
Traditional chemotherapy backbone: anthracycline/taxane-based regimens such as doxorubicin + cyclophosphamide followed by paclitaxel remain common where appropriate [1][19].
Rationale [1]:
- ↓ Risk of recurrence
- ↓ Breast cancer mortality rate
Indications [1]:
| Subtype | Indication for Adjuvant Chemo |
|---|---|
| ER/PR+, HER2− | High recurrence score (RS) by Gene Expression Profiling (OncotypeDX) — chemo benefit likely outweighs risk; see below |
| ER/PR−, HER2− (triple negative) | Chemotherapy backbone; add pembrolizumab for stage II–III disease when eligible, and consider capecitabine for residual HER2-negative/TNBC disease after standard neoadjuvant therapy [19][20] |
| HER2+ | Chemo with anti-HER2 therapy; residual invasive disease after neoadjuvant chemo + HER2 therapy should receive adjuvant T-DM1 [19] |
Regimens [1]:
| Regimen | Components | Notes |
|---|---|---|
| Anthracycline-based | Doxorubicin + Cyclophosphamide + Paclitaxel (ACT) | First-line; most commonly used |
| Taxane-based | Cyclophosphamide + Docetaxel | Indicated in patients with cardiac disease (anthracyclines are cardiotoxic) |
| CMF | Cyclophosphamide + Methotrexate + Fluorouracil | Conventional regimen before the era of anthracyclines [1]; rarely used now |
This deserves special mention because it is the key tool that determines whether many ER+/HER2− patients benefit from chemotherapy [1][21]:
- Well-validated gene expression profile to predict chemotherapy benefit for women with ER+ breast cancer and either limited or no nodal involvement
- Performed on formalin-fixed, paraffin-embedded tissue of the excised invasive component
- Provides a Recurrence Score (RS). Older cutoffs used low/intermediate/high groupings, but current practice is more nuanced after TAILORx/RxPONDER:
| Patient group | OncotypeDX implication |
|---|---|
| Node-negative, age > 50 | RS < 26: little/no chemotherapy benefit; endocrine therapy alone is usually appropriate. RS ≥ 26: offer chemoendocrine therapy [21] |
| Node-negative, age ≤ 50 | RS < 16: little/no chemotherapy benefit. RS 16–25: chemoendocrine therapy may be offered. RS ≥ 26: offer chemoendocrine therapy [21] |
| Post-menopausal, 1–3 positive nodes | OncotypeDX may guide decisions; RS 0–25 generally no chemotherapy benefit, RS ≥ 26 → chemoendocrine therapy [21] |
| Pre-menopausal, 1–3 positive nodes | Do not use OncotypeDX to withhold chemotherapy; RxPONDER showed chemotherapy benefit even with RS 0–25 [21] |
| ≥ 4 positive nodes | Evidence is insufficient to use OncotypeDX routinely to decide against chemotherapy [21] |
Why is this important? Without genomic profiling, many ER+ patients received chemotherapy "just in case." OncotypeDX can spare many post-menopausal node-negative or limited node-positive ER+/HER2− patients unnecessary chemotherapy. In pre-menopausal node-positive disease, however, chemotherapy benefit cannot be safely excluded using a low RS alone.
NO role of neoadjuvant radiotherapy in breast cancer treatment [1].
5.2.1 Adjuvant Radiotherapy
- ↓ Locoregional recurrence rate
- ↓ Breast cancer mortality rate
| Type | Indications | Complications |
|---|---|---|
| Whole Breast Radiation Therapy (WBRT) | ALL patients undergoing BCS (compulsory component of BCT) [1][2]; Post-mastectomy patients with high-risk features: node+ ≥ 4 involved LN; node− T2 with high-grade, high-risk receptor biology, or lymphovascular invasion; T3 or T4 primary; positive surgical margins [1][2] | Short-term: skin fibrosis, telangiectasia, arm oedema; Long-term: rib fracture, cardiotoxicity, pulmonary fibrosis/pneumonitis, lymphoedema, RT-induced secondary malignancy [1][2] |
| Regional Nodal Irradiation | Node+ ≥ 4 involved LN; node− T2 with high-risk features; T3/T4 primary [1] | Lymphoedema, axillary fibrosis [1] |
Why is RT compulsory after BCS? The surgeon removes the macroscopic tumour, but microscopic disease (subclinical foci) may remain in the surrounding breast tissue. RT sterilises these residual foci, reducing local recurrence from ~30–40% (BCS alone) to ~5–10% (BCS + RT) — making BCT equivalent to mastectomy.
Indicated in ALL ER/PR+ cases unless contraindicated [2].
Rationale: Breast cancers that express ER depend on oestrogen for proliferation. Blocking this pathway → tumour growth arrest and apoptosis. This is the longest-duration adjuvant treatment — total treatment for 5–10 years [2].
| Agent | Class | Mechanism | Who Can Receive | Side Effects |
|---|---|---|---|---|
| Tamoxifen | SERM (Selective Oestrogen Receptor Modulator) | Competitively binds ER in breast tissue → blocks oestrogen from activating proliferative gene transcription. However, acts as an oestrogen agonist in the endometrium and bone | Pre- and post-menopausal women | Weight gain, hot flushing, ↑ risk of endometrial carcinoma (agonist effect in uterus), VTE (DVT/PE) [2] |
| Aromatase Inhibitors (AIs) — letrozole, anastrozole, exemestane | Aromatase inhibitor | Blocks the enzyme aromatase that converts adrenal androgens to oestrogen in peripheral adipose tissue. In post-menopausal women, this is the primary oestrogen source (ovaries are inactive) | Post-menopausal women ONLY (in pre-menopausal women, ovarian oestrogen production is NOT dependent on aromatase in adipose tissue — so AIs alone are ineffective) | Osteoporosis/fractures (oestrogen is protective for bone), arthralgia, cardiovascular risk [2] |
| GnRH analogues (e.g., goserelin) | GnRH agonist → ovarian suppression | Continuous GnRH stimulation → desensitisation of pituitary → ↓ LH/FSH → ↓ ovarian oestrogen production | Pre-menopausal women (combined with tamoxifen or exemestane for greater efficacy — SOFT, TEXT trials) [2] | Menopausal symptoms, osteoporosis |
| Bilateral oophorectomy | Surgical ovarian ablation | Permanent removal of ovarian oestrogen source | Pre-menopausal (rarely done now) [2] | Surgical menopause |
Hormonal therapy is NOT given concurrently with chemotherapy [2]. Why? Tamoxifen arrests breast cancer cell proliferation (G1 arrest). Chemotherapy targets rapidly dividing cells. If you stop cells from dividing (tamoxifen) and then give chemo (which kills dividing cells), the chemo won't work as well — the cancer cells are "hidden" in quiescence. So chemo first, then endocrine therapy sequentially.
AIs are more effective than tamoxifen in post-menopausal women [2], but both remain valid options. The choice depends on side-effect profile and patient tolerance.
5.4 Targeted Therapy
Trastuzumab (Herceptin) [1][2][19]:
- Total duration: 1 year with regular cardiac function monitoring [19]
- Indicated for HER2+ breast cancer — defined by IHC 3+ or ISH/FISH-amplified. Strongly recommended with chemotherapy for node-positive disease and node-negative tumours > 1 cm [19]
- Mechanism: Monoclonal antibody targeting the extracellular domain of HER2 receptor → blocks downstream signalling (RAS-MAPK, PI3K-Akt) → also triggers antibody-dependent cellular cytotoxicity (ADCC)
- Side effects: Cardiotoxicity [2] — not used concurrently with anthracyclines (both are cardiotoxic; sequential use reduces cardiac risk); hypersensitivity reactions [2]
Additional HER2-directed options [19]:
- Pertuzumab may be added to trastuzumab-based chemotherapy, especially for node-positive HER2+ disease.
- T-DM1 (trastuzumab emtansine) for 14 cycles should be offered if residual invasive HER2+ disease remains after standard neoadjuvant chemotherapy plus HER2-targeted therapy.
- Neratinib may be used as extended adjuvant therapy in selected early-stage HER2+ patients, particularly HR-positive and node-positive patients, but diarrhoea prophylaxis is essential and no OS benefit has been shown.
- Lapatinib is not used routinely in the adjuvant setting.
- Olaparib — indicated for selected high-risk germline BRCA1/2 carriers with HER2-negative early breast cancer after completion of local therapy and chemotherapy [2][18]
- Mechanism: BRCA-mutant cells are already deficient in homologous recombination DNA repair. PARP inhibitors block the remaining base excision repair pathway → synthetic lethality (cancer cells cannot repair DNA by any mechanism → accumulation of lethal DNA damage → apoptosis). Normal cells with one functioning BRCA allele survive.
- Abemaciclib for 2 years plus endocrine therapy may be offered to HR+/HER2−, node-positive, high-risk early breast cancer meeting monarchE-type criteria: ≥ 4 positive axillary nodes, or 1–3 positive nodes plus grade 3 disease, tumour ≥ 5 cm, or Ki-67 ≥ 20% [19].
- Ribociclib for 3 years plus endocrine therapy may be offered to selected anatomic stage II–III HR+/HER2− patients at high risk of recurrence based on NATALEE; benefits, toxicity, cost, and patient preference should be weighed, especially in lower-risk node-negative disease [19].
- Mechanism: CDK4/6 drive G1→S cell cycle progression; inhibiting them arrests proliferation of ER+ cancer cells (which are particularly dependent on cyclin D-CDK4/6 pathway)
Bisphosphonates / Denosumab [1][2]:
- Osteoclast inhibitors — indicated for palliation in patients with bone metastasis [1]
- Bisphosphonates (e.g., pamidronic acid, zoledronic acid): reduce bone resorption → improve symptoms of bone pain, reduce skeletal-related events (SREs), improve QOL [1]
- SREs = pathological fractures, spinal cord compression, hypercalcaemia of malignancy [1]
- Denosumab (RANKL monoclonal antibody) [1][2]: RANKL is the ligand that activates osteoclasts; blocking it → potent osteoclast inhibition
| Stage | Neoadjuvant | Surgery | Adjuvant Systemic | Adjuvant RT |
|---|---|---|---|---|
| DCIS (Stage 0) | None | Van Nuys Index: Low = WLE; Intermediate = WLE + RT; High = Mastectomy + SLNB [1]. Margin ≥ 2 mm [1]. ALND NOT indicated for pure DCIS [1] | ER/PR+ DCIS → Tamoxifen/AI (reduces recurrence/contralateral cancer, no survival benefit) [1]. No chemo. No targeted therapy [1] | If intermediate score + BCT [1] |
| LCIS | None | Prophylaxis: Bilateral simple mastectomy + reconstruction (selected high-risk); otherwise close surveillance [1] | Chemoprevention: Tamoxifen [1] | — |
| Early (Stage I–II) | Consider if large tumour convertible from mastectomy to BCS [2]; offer neoadjuvant systemic therapy for high-risk HER2+ or TNBC when residual disease would guide adjuvant therapy [19] | BCS + SLNB (preferred if eligible) OR Mastectomy ± reconstruction + SLNB/ALND [1] | ± Chemo (genomic assay/clinical risk for ER+/HER2−), endocrine therapy (all ER/PR+), anti-HER2 therapy (HER2+), ± pembrolizumab (eligible TNBC), ± olaparib (high-risk gBRCA HER2−), ± CDK4/6 inhibitor (high-risk HR+/HER2−) [1][2][19][20][21] | After BCS (WBRT) [1]; after mastectomy if high-risk features [1] |
| Locally advanced (Stage III) | Neoadjuvant systemic therapy: TNBC chemo + pembrolizumab; HER2+ chemo + trastuzumab ± pertuzumab; HR+/HER2− chemo or selected endocrine therapy [19][20] | BCS or Mastectomy (depending on response) + SLNB or ALND [1] | Response-adapted: T-DM1 for residual HER2+; pembrolizumab continuation for eligible TNBC; capecitabine for selected residual HER2−/TNBC; olaparib for selected high-risk gBRCA HER2−; endocrine/CDK4/6 for high-risk HR+/HER2− | Post-mastectomy RT (high-risk); post-BCS WBRT [1] |
| Metastatic (Stage IV) | — | Palliative — surgery not for cure; may be used for local symptom control (e.g., fungating tumour) | Hormonal therapy (ER/PR+), Chemo (organ metastasis: liver, lung), Targeted therapy (HER2), Bone therapy (bisphosphonates/denosumab for bone mets), ± Immunotherapy (TNBC PD-L1+) [2] | Palliative RT — brain metastasis, cord compression, SVCO, painful bone mets [2]; steroids for brain met [2] |
| Complication | Mechanism / Explanation |
|---|---|
| Seroma | Lymphatic/serosanguinous fluid collection in dead space after tissue removal |
| Haematoma | Surgical bleeding |
| Wound infection | Contamination of surgical site |
| Skin flap / NAC necrosis (if reconstruction) | Compromised blood supply to the thin skin flaps |
| Arm/shoulder pain, numbness, frozen shoulder | Nerve injury + post-operative immobility |
| Phantom breast syndrome | Altered chest wall sensation that may persist years after surgery [2] — similar to phantom limb pain; the brain's somatosensory cortex retains a "map" of the breast |
High Yield Summary — Management of Breast Cancer
-
BCT = BCS + RT (compulsory). Equivalent survival to mastectomy. Margin = "no ink on tumour."
-
Contraindications to BCS: Multicentric disease, high tumour-breast ratio, diffuse microcalcifications, persistent positive margins, IBC, C/I to RT (pregnancy, prior RT, CTD), patient refusal of RT.
-
SLNB: For clinically node-negative early stage. Dual tracer (Tc-99m + blue dye). Max 3–4 nodes. If 1–2 positive SLN + planned RT (BCS) → ALND may NOT be needed (Z0011).
-
ALND: Clinically positive nodes, ≥ 3 positive SLN, IBC. Standard = Level I + II. Level III only if grossly positive.
-
Neoadjuvant systemic therapy: Locally advanced/inoperable; downstage to enable BCS; mark tumour with clip/seed. Stage II–III TNBC should receive chemo + pembrolizumab followed by adjuvant pembrolizumab; high-risk HER2+ should receive chemo + trastuzumab ± pertuzumab.
-
Adjuvant chemo/response-adapted therapy: Use OncotypeDX carefully for ER+/HER2− decisions; residual HER2+ after neoadjuvant therapy → T-DM1; residual HER2−/TNBC may receive capecitabine; high-risk gBRCA HER2− → olaparib.
-
Hormonal therapy (5–10 years): All ER/PR+. Tamoxifen (pre/post-menopausal); AI (post-menopausal only, more effective); GnRH agonist (pre-menopausal). NOT concurrent with chemo.
-
HER2 therapy: Trastuzumab-based therapy for HER2+ disease, usually total 1 year with cardiac monitoring; add pertuzumab for selected higher-risk disease; T-DM1 if residual invasive disease after neoadjuvant HER2 therapy.
-
Palliative: Bone mets → bisphosphonates/denosumab. Brain mets/cord compression/SVCO → RT ± steroids.
-
ALND complications: Long thoracic nerve (winged scapula), thoracodorsal nerve (weak shoulder adduction/IR), intercostobrachial nerve (paraesthesia medial arm), lymphoedema, Stewart-Treves syndrome.
Active Recall - Management of Breast Cancer
References
[1] Senior notes: felixlai.md (Sections on BCT, mastectomy types, breast reconstruction, lymph node management, SLNB, ALND, chemotherapy, radiotherapy, hormonal therapy, targeted therapy, bisphosphonates, DCIS/LCIS management, gene expression profiling, treatment by stage) [2] Senior notes: maxim.md (Sections on BCS, mastectomy, axillary management, SLNB, ALND, adjuvant therapy assessment table, neoadjuvant therapy, palliative therapy, complications) [12] Lecture slides: The Managment of breast cancer_Prof A Kwong 20_2_2020.pdf (pp. 37, 39, 42, 55, 68) [13] Lecture slides: GC 181. Breast mass breast cancer; benign breast diseases; mammography; breast cancer screening.pdf (pp. 32, 36) [14] Lecture slides: GC 181. Breast mass breast cancer; benign breast diseases; mammography; breast cancer screening.pdf (p. 44) [15] Lecture slides: The Managment of breast cancer_Prof A Kwong 20_2_2020.pdf (p. 68) [16] Image credit: Cleveland Clinic (Jackson-Pratt drain image) [17] Image credit: Christiana Care (TRAM flap image) [18] Image credit: National Cancer Institute (SLNB image) [19] ASCO Guideline: Selection of Optimal Adjuvant Chemotherapy and Targeted Therapy for Early Breast Cancer, rapid updates through 2024; reviewed 2026. [20] ASCO Guideline: Neoadjuvant Chemotherapy, Endocrine Therapy, and Targeted Therapy for Breast Cancer, including pembrolizumab rapid update; reviewed 2026. [21] ASCO Guideline: Biomarkers for Adjuvant Endocrine and Chemotherapy in Early-Stage Breast Cancer.
Complications of Breast Cancer
Complications in breast cancer arise from three sources: (1) the disease itself (local progression and distant metastasis), (2) surgical treatment, and (3) adjuvant therapies (radiotherapy, chemotherapy, hormonal therapy, targeted therapy). Understanding these complications from first principles — knowing why each one happens — is far more valuable for exams and clinical practice than rote memorisation.
1. Complications of the Disease Itself
| Complication | Pathophysiological Mechanism |
|---|---|
| Skin ulceration / fungating tumour | Advanced tumour erodes through dermis → necrotic, malodorous, bleeding wound. Occurs when tumour outgrows its blood supply (central necrosis) and invades the overlying skin |
| Peau d'orange | Tumour cells obstruct dermal lymphatic channels → lymphatic oedema of skin → pitting at hair follicle/sweat gland openings (tethered by Cooper's ligaments while surrounding skin swells) [1] |
| Skin dimpling / tethering | Tumour invades or fibroses Cooper's ligaments → shortening → retraction of overlying skin |
| Nipple retraction | Tumour invades and fibroses subareolar ducts → pulls nipple inward |
| Arm lymphoedema from axillary obstruction | Advanced tumour or matted nodal disease obstructs axillary lymphatic drainage (distinct from post-surgical lymphoedema) |
| Brachial plexus involvement | Locally advanced tumour or nodal mass invades the brachial plexus (C5–T1 roots) → arm pain, weakness, paraesthesia, and eventually paralysis |
| Chest wall invasion | Direct tumour extension into pectoralis major/minor, intercostal muscles, or ribs → pain, fixation, and potential pathological rib fractures |
Breast cancer metastasises to: Bone > Liver > Lung > Brain > Ovaries > Adrenals > Pleura [1][4].
| Site | Complications | Mechanism | Presentation |
|---|---|---|---|
| Bone (most common site) | Pathological fractures; spinal cord compression; hypercalcaemia of malignancy | Breast cancer cells produce PTHrP (parathyroid hormone-related peptide) and activate RANKL → osteoclastic bone resorption → lytic lesions → structural weakness (fractures) + release of calcium into blood (hypercalcaemia). Vertebral metastases → epidural extension → spinal cord compression | Bone pain (back, pelvis, long bones), fractures from minimal trauma, progressive leg weakness/sensory loss/bladder dysfunction (cord compression), confusion/constipation/polyuria (hypercalcaemia) |
| Liver | Hepatic failure; biliary obstruction; portal hypertension | Progressive replacement of hepatic parenchyma with tumour → loss of metabolic, synthetic, and excretory function; mass effect on bile ducts/portal vessels | Jaundice, nausea/vomiting, abdominal pain, hepatomegaly, ascites, raised LFT [1] |
| Lung / Pleura | Malignant pleural effusion; lymphangitis carcinomatosa; airway obstruction | Tumour cells in pleural lymphatics → impaired lymphatic drainage → fluid accumulation; tumour obstructing bronchi → collapse/infection; lymphangitic spread along pulmonary lymphatics → diffuse interstitial infiltrate | Dyspnoea, cough, reduced breath sounds (effusion), progressive breathlessness at rest (lymphangitis) [1] |
| Brain | Raised intracranial pressure; focal neurological deficits; seizures | Metastatic deposits act as space-occupying lesions → cerebral oedema → raised ICP; destruction of functional cortex/tracts; irritation of cortex → seizures | Headache (worse in morning), vomiting, papilloedema, hemiparesis, speech disturbance, personality change |
| Ovaries / Peritoneum | Malignant ascites; ovarian mass; bowel obstruction (especially ILC — metastasises to unusual locations including meninges, GI tract, and peritoneum) [1] | Peritoneal carcinomatosis → impaired peritoneal fluid absorption → ascites; tumour encasement of bowel → obstruction |
Skeletal-related events (SREs) are a specifically defined set of bone metastasis complications: pathological fractures, spinal cord compression, and hypercalcaemia of malignancy [1]. These are the target outcomes for bone-protective agents (bisphosphonates, denosumab).
Hypercalcaemia of Malignancy — First Principles
Breast cancer causes hypercalcaemia through two mechanisms:
- Humoral hypercalcaemia: Tumour cells secrete PTHrP → acts on PTH receptors in kidney (↑ Ca reabsorption, ↑ phosphate excretion) and bone (↑ osteoclast activity) → ↑ serum calcium
- Local osteolytic hypercalcaemia: Tumour cells in bone directly activate osteoclasts (via RANKL, IL-6, etc.) → bone destruction → calcium release
Symptoms mnemonic — "Stones, Bones, Groans, and Psychic Moans":
- Stones = renal stones, nephrocalcinosis, polyuria (calcium overwhelms tubular reabsorption)
- Bones = bone pain, fractures
- Groans = constipation, nausea, vomiting, pancreatitis
- Psychic Moans = confusion, depression, lethargy, coma
| Complication | Mechanism |
|---|---|
| SIADH (Syndrome of Inappropriate ADH Secretion) | Ectopic ADH production by tumour → water retention → hyponatraemia (dilutional) [1] |
| Hypercalcaemia | PTHrP secretion (as above) |
| Hypercoagulable state (Trousseau syndrome) | Cancer cells express tissue factor and release procoagulant microparticles → activation of coagulation cascade → DVT, PE, migratory superficial thrombophlebitis |
2. Complications of Surgical Treatment
| Timing | Complication | Mechanism / Explanation |
|---|---|---|
| General | Wound infection [1] | Bacterial contamination of surgical site; risk increased by haematoma, seroma, diabetes, obesity |
| Bleeding and haematoma [1] | Intra-operative vessel injury or post-operative coagulopathy → blood collection in surgical dead space | |
| Anaesthetic complications [1] | General anaesthesia-related: aspiration, bronchospasm, anaphylaxis, cardiac events | |
| Specific — Early | Seroma [1][2] | Collection of serous fluid in the surgical dead space. After mastectomy, the breast tissue is removed leaving a large potential space between skin flaps and chest wall. Disrupted lymphatic and blood capillaries leak fluid into this space. Untreated seroma → delayed wound healing, wound infection, dehiscence, flap necrosis, and poor cosmetic outcomes. Management: insertion of drains (Jackson-Pratt closed-suction drains) or percutaneous aspiration [1][2] |
| Skin flap necrosis [1][2] | Thin skin flaps created during mastectomy may have compromised blood supply (especially at the distal edges) → ischaemic necrosis. Full-thickness necrosis requires surgical debridement ± skin grafting [1]. Risk increased in smokers, diabetics, and after skin-sparing procedures | |
| NAC necrosis (if nipple-sparing) [2] | Blood supply to the preserved nipple-areolar complex can be compromised by the surgery → ischaemic necrosis. Risk increases with large, ptotic breasts | |
| Specific — Late | Post-mastectomy pain syndrome [1] | Burning, aching, and tight constriction of axilla, upper arm, and chest wall [1]. Mechanism: neuropathic pain from intercostal nerve injury during surgery (nerves cut or stretched when elevating skin flaps); also phantom breast pain (see below). Can be chronic and debilitating |
| Phantom breast syndrome [1][2] | Altered chest wall sensation; exact cause is unknown [1]; might persist years after surgery [2]. Analogous to phantom limb pain — the somatosensory cortex retains a neural representation of the breast; deafferentation → aberrant signalling interpreted as sensation from the absent breast | |
| Arm morbidity [1][2] | Arm or shoulder pain, swelling, numbness, stiffness [1]. Causes include nerve injury, lymphoedema, immobility-related frozen shoulder (adhesive capsulitis) |
ALND carries significantly more morbidity than SLNB — this is precisely why SLNB was developed: suitable for early-stage cancers to avoid full axillary dissection which has complications [12].
| Complication | Mechanism | Clinical Consequence |
|---|---|---|
| Seroma [2] | Disruption of lymphatic channels during dissection → lymphatic fluid accumulates in the axillary space | Fluctuant swelling in axilla; requires aspiration or drainage |
| Long thoracic nerve injury [2] | Nerve runs along the chest wall on the surface of serratus anterior; vulnerable during dissection of Level I–II nodes | Winged scapula — serratus anterior is paralysed → medial border of scapula protrudes posteriorly, especially when pushing against a wall. Why? Serratus anterior protracts and rotates the scapula; without it, the scapula cannot be held against the thoracic cage |
| Thoracodorsal nerve injury [2] | Nerve runs with thoracodorsal vessels posterior to axillary vein | Weakness of latissimus dorsi → impaired shoulder adduction and internal rotation (difficulty pulling arm down or behind back) |
| Medial pectoral nerve injury [2] | Nerve pierces pectoralis minor to supply pectoralis major; courses through Level II nodal tissue | Wasting of pectoralis major → cosmetic deformity of anterior chest wall, weakness of shoulder adduction |
| Intercostobrachial nerve injury [2] | T2 intercostal nerve branch crosses the axilla; almost always sacrificed in ALND [2] | Paraesthesia (numbness/tingling) of axilla, medial arm, and lateral chest wall [2]. This is so common that patients should be warned pre-operatively |
| Upper limb lymphoedema [2] | Removal of axillary lymph nodes disrupts the lymphatic drainage of the arm → lymph fluid accumulates in subcutaneous tissue → chronic swelling | Progressive, often irreversible limb swelling; discomfort; recurrent cellulitis (stagnant lymph = culture medium for bacteria); skin thickening. Management: pneumatic compression device [2], compression garments, manual lymphatic drainage, skin care |
| Upper limb lymphangiosarcoma (Stewart-Treves syndrome) [2] | Chronic lymphoedema → sustained lymphatic stasis → chronic inflammatory microenvironment → malignant transformation of lymphatic endothelium after years to decades | Rare but devastating — angiosarcoma arising in a chronically lymphoedematous limb. Typically presents as purple/bruise-like patches or nodules on the swollen arm, years after mastectomy + ALND. Very poor prognosis |
Stewart-Treves Syndrome
This is a classic exam point: lymphangiosarcoma arising in a chronically lymphoedematous upper limb after mastectomy and axillary dissection. The latency period is typically 5–15 years after surgery. It highlights why minimising axillary surgery (using SLNB instead of ALND when appropriate) is so important — it is not just about numbness and stiffness; chronic lymphoedema carries the risk of a lethal secondary malignancy.
2.3 Complications of Breast Reconstruction [2]
| Complication | Detail |
|---|---|
| Mechanical: migration, malposition, exposure, rupture [2] | Majority of ruptures are often silent — present with changes in breast shape/volume, capsular contracture, palpable lumps (breast or axilla), and pain [2]. Silicone leakage can migrate to axillary lymph nodes (palpable lumps in axilla that may mimic recurrence) |
| Implant infection [2] | Bacterial colonisation of the implant surface (biofilm). Managed by antibiotics ± explantation and irrigation of the pocket → closure over closed-suction drainage [2] |
| Capsular contracture [2] | The body forms a fibrous capsule around any foreign body (normal immune response). When this capsule contracts excessively → painful, fibrous capsule around implant → palpable distortion of breast [2]. Especially common post-infection or post-radiation (radiation accelerates fibrosis). Graded by Baker classification (I = soft/natural → IV = hard/painful/distorted) |
| Breast implant-associated anaplastic large-cell lymphoma (BIA-ALCL) [2] | A rare but important complication. ALK-negative, CD30-positive T-cell lymphoma arising around textured breast implants. Typically presents as a late seroma (fluid collection around the implant years after insertion). Disease confined to the capsule: capsulectomy alone is curative. Disseminated disease: adjuvant chemotherapy (cyclophosphamide, doxorubicin, vincristine, prednisone) or anti-CD30 therapy (brentuximab vedotin) [2] |
| Flap | Specific Complication | Mechanism |
|---|---|---|
| TRAM flap | Abdominal hernia / bulge [2] | Harvest of rectus abdominis muscle weakens the anterior abdominal wall |
| Donor site seroma/infection | Large soft tissue harvest site | |
| DIEP flap | Complete flap loss [2] | Requires microsurgery (inferior epigastric vessels anastomosed to internal mammary vessels); risk of failed micro-anastomosis → flap ischaemia → loss [2]. Longer operative time |
| LD flap | Limited range of motion at shoulder [2] | Latissimus dorsi is sacrificed; functionally significant in athletes/manual workers |
3. Complications of Adjuvant Therapies
| Timing | Complication | Mechanism |
|---|---|---|
| Short-term | Breast/chest wall skin fibrosis [1][2] | Radiation damages dermal fibroblasts → excessive collagen deposition → skin thickening, tightness, telangiectasia (dilated superficial blood vessels — radiation damages endothelium → compensatory angiogenesis with fragile vessels) |
| Arm oedema [1] | Radiation to axilla/supraclavicular field damages remaining lymphatic channels → impaired drainage → oedema (synergistic with surgical lymphatic disruption from ALND) | |
| Radiation dermatitis | Acute inflammatory response of the skin to ionising radiation — erythema, desquamation, occasionally moist desquamation | |
| Long-term | Rib fracture [1] | Radiation-induced osteonecrosis of underlying ribs → weakened bone → insufficiency fractures (especially left-sided treatment involving lower ribs) |
| Cardiotoxicity [1][2] | Especially with left-sided breast RT — the heart is in the radiation field. Radiation damages coronary artery endothelium → accelerated atherosclerosis; damages myocardium → fibrosis → cardiomyopathy; pericardial inflammation → pericarditis/effusion. Modern techniques (deep inspiratory breath-hold, IMRT, proton therapy) aim to minimise cardiac dose | |
| Pulmonary fibrosis or pneumonitis [1][2] | Radiation damages alveolar epithelium and pulmonary endothelium → inflammatory pneumonitis (weeks to months) → pulmonary fibrosis (months to years) | |
| Secondary RT-induced malignancy [1][2] | Radiation is carcinogenic — can induce secondary cancers (sarcomas, contralateral breast cancer, lung cancer) in the irradiated field. Typically appears ≥ 5–10 years after RT. Risk is small but non-zero and must be weighed against benefit | |
| Regional nodal irradiation | Lymphoedema; axillary fibrosis [1] | Same lymphatic damage mechanism as above; compounded if ALND also performed |
| Agent / Regimen | Key Side Effects | Mechanism |
|---|---|---|
| General (all chemo) | Myelosuppression (neutropenia, anaemia, thrombocytopenia), nausea/vomiting, alopecia, mucositis, fatigue, immunosuppression | Chemotherapy targets all rapidly dividing cells — bone marrow, GI mucosa, hair follicles are collateral damage |
| Anthracyclines (doxorubicin) | Cardiotoxicity (dose-dependent, cumulative) | Generates reactive oxygen species → direct myocyte damage; also topoisomerase IIβ-mediated DNA damage in cardiomyocytes → irreversible myocyte death → dilated cardiomyopathy. Cumulative dose limit typically ~450–550 mg/m² |
| Cyclophosphamide | Haemorrhagic cystitis | Metabolite acrolein is excreted by kidneys and damages bladder urothelium. Prevented by adequate hydration and mesna (binds acrolein in urine) |
| Taxanes (paclitaxel, docetaxel) | Peripheral neuropathy (sensory > motor), myalgias/arthralgias | Stabilises microtubules → disrupts axonal transport in peripheral nerves → neuropathy |
| Methotrexate | Mucositis, hepatotoxicity, myelosuppression | Folate antagonist → inhibits dihydrofolate reductase → impaired DNA synthesis in all rapidly dividing cells. Rescued with leucovorin (folinic acid) |
| Agent | Key Side Effects | Mechanism |
|---|---|---|
| Tamoxifen [2] | Weight gain; hot flushes; ↑ risk of endometrial carcinoma; VTE (DVT/PE) [2] | Tamoxifen is a SERM — it blocks ER in breast (therapeutic) but activates ER in endometrium → endometrial proliferation → ↑ risk of endometrial hyperplasia/cancer. Activates ER in liver → ↑ clotting factors (especially Factor V, fibrinogen) → pro-thrombotic state → VTE |
| Aromatase Inhibitors (letrozole, anastrozole, exemestane) [2] | Osteoporosis / fractures; arthralgia; cardiovascular risk [2] | Complete oestrogen deprivation in post-menopausal women. Oestrogen is protective for bone (inhibits osteoclasts, promotes osteoblasts); removing it → accelerated bone loss → osteoporosis → fractures. Also removes cardioprotective effects of oestrogen |
| GnRH agonists (goserelin) | Menopausal symptoms (hot flushes, vaginal dryness), osteoporosis | Chemical ovarian suppression → iatrogenic menopause → oestrogen deficiency symptoms |
Why does tamoxifen cause endometrial cancer but aromatase inhibitors do not? Tamoxifen has tissue-specific effects — it is an ER antagonist in the breast but an ER agonist in the endometrium and liver. AIs, on the other hand, do not activate ER anywhere — they simply reduce the amount of oestrogen available. So the endometrium is deprived of oestrogen stimulus and actually atrophies. This is why AIs carry a fracture risk (bone also lacks oestrogen) but NOT an endometrial cancer risk.
| Agent | Key Side Effects | Mechanism |
|---|---|---|
| Trastuzumab (Herceptin) [2] | Cardiotoxicity (reduced LVEF, heart failure); hypersensitivity reactions [2] | HER2 receptors are expressed on cardiomyocytes and are involved in cardiac repair and stress response. Blocking HER2 with trastuzumab → impaired cardiac stress response → cardiomyopathy. Unlike anthracycline cardiotoxicity, trastuzumab cardiotoxicity is typically reversible and not dose-dependent (does not cause myocyte death; rather, impairs function). Not used concurrently with anthracyclines (combined cardiotoxicity would be excessive) [2] |
| PARP inhibitors (olaparib) | Myelosuppression (anaemia, neutropenia), nausea, fatigue, risk of MDS/AML (rare) | PARP is involved in DNA repair in all cells; inhibiting it in bone marrow progenitors → impaired repair → myelosuppression; in rare cases, genomic instability → secondary haematological malignancy |
| CDK4/6 inhibitors (abemaciclib) | Diarrhoea, neutropenia, fatigue | CDK4/6 drives cell cycle in many tissues; GI epithelium and bone marrow are affected |
| Agent | Key Side Effects | Mechanism |
|---|---|---|
| Bisphosphonates (zoledronic acid, pamidronic acid) | Osteonecrosis of the jaw (ONJ); renal toxicity; flu-like reaction | ONJ: bisphosphonates are concentrated in bone and suppress osteoclast activity → impaired bone remodelling → jaw (high turnover bone exposed to oral flora via dental procedures) → necrosis. Renal: direct tubular toxicity, especially with rapid IV infusion |
| Denosumab | Osteonecrosis of the jaw; hypocalcaemia | RANKL blockade → profound osteoclast inhibition → impaired calcium mobilisation from bone → hypocalcaemia (must supplement calcium and vitamin D). ONJ mechanism similar to bisphosphonates |
| Timeline | Surgical | RT | Systemic Therapy |
|---|---|---|---|
| Immediate / Early | Bleeding, haematoma, wound infection, seroma, skin flap/NAC necrosis, nerve injuries (ALND) | Radiation dermatitis, fatigue | Myelosuppression, nausea, alopecia, mucositis |
| Intermediate | Frozen shoulder, wound dehiscence | Pneumonitis | Peripheral neuropathy (taxanes), haemorrhagic cystitis (cyclophosphamide) |
| Late / Chronic | Post-mastectomy pain syndrome, phantom breast syndrome, lymphoedema, Stewart-Treves syndrome | Skin fibrosis/telangiectasia, rib fracture, cardiotoxicity, pulmonary fibrosis, RT-induced malignancy | Cardiotoxicity (anthracyclines, trastuzumab), endometrial cancer (tamoxifen), VTE (tamoxifen), osteoporosis (AIs), ONJ (bisphosphonates), BIA-ALCL (implants) |
5. Prognosis [1]
| Category | Poor Prognostic Factors |
|---|---|
| Patient factors | Extreme of age (very young or very old); smoking |
| Tumour size | Large tumour size (higher T stage) |
| Nodal status | Greater number of nodal involvement (N). N0: 5-year survival ~70%. More nodes → worse survival [2] |
| Metastasis | Presence of metastatic disease (M1) |
| Grade | Poorly differentiated (Grade 3) |
| Proliferation | High Ki67 (detected by IHC) — indicates rapid tumour cell division |
| Histological subtype | IDC, ILC, mixed ductal/lobular, metaplastic, micropapillary (poor prognosis subtypes); tubular, medullary, mucinous, papillary (good prognosis subtypes) [1] |
| Receptor status | Absence of ER and PR expression (no endocrine therapy option); HER2 overexpression (aggressive biology, though now targetable) [1] |
| Stage | 5-Year Survival |
|---|---|
| Stage I | 97.5% |
| Stage II | 87.8% |
| Stage III | 66.2% |
| Stage IV | 19.3% |
The dramatic drop from Stage I (97.5%) to Stage IV (19.3%) underscores why early detection through screening is so impactful. The biological behaviour is the same cancer — the difference is whether you catch it before or after it has spread systemically.
High Yield Summary — Complications of Breast Cancer
Disease complications:
- Local: Skin ulceration, peau d'orange, dimpling, nipple retraction, chest wall invasion, brachial plexus invasion.
- Metastatic: Bone (pathological fractures, cord compression, hypercalcaemia), liver (hepatomegaly, jaundice), lung (effusion, dyspnoea), brain (raised ICP, focal neurology).
- SREs = pathological fractures + cord compression + hypercalcaemia.
Surgical complications: 4. Mastectomy: Seroma (most common specific), skin flap necrosis, post-mastectomy pain, phantom breast, arm morbidity. 5. ALND — 4 nerves: Long thoracic (winged scapula), thoracodorsal (weak adduction/IR), medial pectoral (pec major wasting), intercostobrachial (medial arm paraesthesia). Plus lymphoedema and Stewart-Treves syndrome (lymphangiosarcoma). 6. Implant: Capsular contracture, rupture (often silent), BIA-ALCL (ALK−, CD30+; capsulectomy curative if localised).
Therapy complications: 7. RT: Skin fibrosis, rib fracture, cardiotoxicity (left-sided), pulmonary fibrosis, secondary malignancy. 8. Anthracyclines: Dose-dependent irreversible cardiotoxicity. Trastuzumab: Reversible cardiotoxicity (not concurrent with anthracyclines). 9. Tamoxifen: Endometrial cancer, VTE (ER agonist effect in uterus/liver). AIs: Osteoporosis/fractures (no endometrial cancer risk). 10. Bisphosphonates/Denosumab: ONJ, hypocalcaemia (denosumab).
Active Recall - Complications of Breast Cancer
References
[1] Senior notes: felixlai.md (Sections on complications of mastectomy, ALND complications, radiotherapy complications, metastatic disease, prognostic factors, 5-year survival, breast reconstruction, IBC, ILC metastasis patterns) [2] Senior notes: maxim.md (Sections on mastectomy complications, ALND complications including 4 nerves and Stewart-Treves syndrome, adjuvant therapy side effects, breast implant complications including BIA-ALCL, breast reconstruction flap comparisons, prognostic factors) [4] Senior notes: maxim.md (Staging investigations — metastatic sites: bone, liver, lung, brain) [12] Lecture slides: The Managment of breast cancer_Prof A Kwong 20_2_2020.pdf (p. 42 — SLNB and axillary dissection complications rationale)
High Yield Summary
Breast Cancer — Key Points:
-
Definition: Malignant neoplasm of breast epithelium (TDLU). In-situ vs. invasive depends on basement membrane breach.
-
Epidemiology (HK): 1st most common cancer in females, 3rd overall; median age ~55 (younger than West); lifetime risk 1:16.
-
Risk Factors — "Oestrogen Exposure" is the unifying theme: Early menarche, late menopause, nulliparity, no breastfeeding, late first pregnancy, COC/HRT, obesity (post-menopausal).
-
Genetics: BRCA1/2 (autosomal dominant tumour suppressor genes for DNA repair); Li-Fraumeni (TP53); Cowden (PTEN); CDH1 → lobular cancer.
-
BRCA1: ~65% breast cancer risk by 70, ~39% ovarian; associated with triple-negative subtype. BRCA2: ~45% breast cancer risk by 70, ~11% ovarian; associated with male breast cancer (~6%).
-
Pathology: IDC NOS (80%) > ILC (3–8%) > Special types. DCIS = precursor to IDC; LCIS = marker/precursor for bilateral invasive cancer.
-
Molecular Subtypes: Luminal A (best prognosis, endocrine therapy), Luminal B, HER2+ (anti-HER2 therapy), Triple-negative (worst prognosis, chemo/PARP/immunotherapy).
-
Clinical Features: Hard, irregular, fixed, non-tender mass in UOQ; nipple discharge (unilateral, bloody, single duct = high risk); peau d'orange (dermal lymphatic obstruction); skin dimpling (Cooper's ligament invasion); nipple retraction (duct fibrosis/invasion).
-
Paget's Disease: Eczematoid nipple change + underlying breast cancer (usually HER2+). IBC: T4d, peau d'orange ≥ 1/3 breast, < 6 months history, NOT true infection.
-
Screening (Current): Emphasize breast awareness and early assessment of new breast changes. Routine monthly BSE is not recommended for average-risk women. Use risk-based mammography (e.g., CEWG risk-stratified approach in HK; USPSTF biennial screening age 40–74).
-
Genetic Testing: Test affected individual first → only test unaffected relatives if mutation found.
High Yield Summary — Differential Diagnosis of Breast Cancer
-
DDx of breast lump by age: Young → fibroadenoma, cyst, fibrocystic changes. Old → carcinoma, Phyllodes tumour. Fat necrosis and lipoma at any age.
-
Fibroadenoma = most common benign tumour; "breast mouse" — highly mobile, rubbery, well-defined; hormonally dependent; simple type = no cancer risk.
-
Phyllodes tumour = fibroepithelial; can be malignant; metastasises via blood NOT lymphatics → ALND not required; excise with ≥ 1 cm margin.
-
Fat necrosis = mimics cancer clinically AND radiologically → core biopsy mandatory to differentiate.
-
Nipple discharge: Most common pathological cause = intraductal papilloma. Suspicious features: unilateral, single duct, bloody, spontaneous. Malignancy in 5–15% of pathological discharge (most commonly DCIS).
-
Paget's disease = unilateral nipple eczema + underlying cancer (~80%, usually HER2+). DDx from bilateral nipple eczema (dermatitis).
-
IBC vs. mastitis: IBC = peau d'orange ≥ 1/3 breast, erythema, NO fever/leukocytosis; Mastitis = fever + leukocytosis, responds to antibiotics.
-
ADH/ALH = high-risk lesions (4–5× risk); if found on core biopsy → MUST do excisional biopsy to rule out adjacent malignancy.
-
LCIS = premalignant condition, NOT true cancer; marker of bilateral risk; observe unless pleomorphic type.
-
Triple assessment (clinical + radiological + pathological) resolves virtually all diagnostic dilemmas.
High Yield Summary — Diagnosis of Breast Cancer
-
Triple Assessment = Clinical + Radiological + Pathological. Combined sensitivity 99.6%, specificity 93%. Positive if ANY one is positive. Negative only when ALL three are negative.
-
Mammography: Primary imaging for > 35 years; CC + MLO views; malignant features = spiculated mass, pleomorphic/linear branching microcalcifications, architectural distortion. Not sensitive in dense breasts.
-
USG: First-line for < 35 years, pregnant, lactating; distinguishes cyst from solid; guides biopsy. Malignant = taller-than-wide, hypoechoic, spiculated, central vascularity.
-
BI-RADS: Standardised reporting. BI-RADS 4–5 → tissue diagnosis (biopsy). BI-RADS 3 → 6-month follow-up.
-
Core needle biopsy = first-line for tissue diagnosis. Provides architecture, grade, receptor status. FNAC only for low-risk/cystic lesions.
-
Receptor testing (ER/PR/HER2/Ki67) is mandatory for all new diagnoses — determines molecular subtype and guides therapy.
-
HER2: IHC 3+ or FISH-amplified = positive. IHC 2+ = equivocal → reflex FISH. HER2+ = higher recurrence, higher mortality, but targetable with trastuzumab.
-
MRI: High sensitivity, low specificity. Not routine. Indications: occult primary with positive axillary LN, ILC extent, implants, treatment response monitoring.
-
Staging: CXR (lung), USG abdomen (liver), bone scan (bone), PET-CT (stage ≥ IIIA or symptomatic), bloods (LFT, Ca/PO₄, CA15.3, CEA).
-
Discordance between any pillars → further investigation (repeat/excisional biopsy). Never dismiss a suspicious lesion on incomplete assessment.
High Yield Summary — Management of Breast Cancer
-
BCT = BCS + RT (compulsory). Equivalent survival to mastectomy. Margin = "no ink on tumour."
-
Contraindications to BCS: Multicentric disease, high tumour-breast ratio, diffuse microcalcifications, persistent positive margins, IBC, C/I to RT (pregnancy, prior RT, CTD), patient refusal of RT.
-
SLNB: For clinically node-negative early stage. Dual tracer (Tc-99m + blue dye). Max 3–4 nodes. If 1–2 positive SLN + planned RT (BCS) → ALND may NOT be needed (Z0011).
-
ALND: Clinically positive nodes, ≥ 3 positive SLN, IBC. Standard = Level I + II. Level III only if grossly positive.
-
Neoadjuvant systemic therapy: Locally advanced/inoperable; downstage to enable BCS; mark tumour with clip/seed. Stage II–III TNBC should receive chemo + pembrolizumab followed by adjuvant pembrolizumab; high-risk HER2+ should receive chemo + trastuzumab ± pertuzumab.
-
Adjuvant chemo/response-adapted therapy: Use OncotypeDX carefully for ER+/HER2− decisions; residual HER2+ after neoadjuvant therapy → T-DM1; residual HER2−/TNBC may receive capecitabine; high-risk gBRCA HER2− → olaparib.
-
Hormonal therapy (5–10 years): All ER/PR+. Tamoxifen (pre/post-menopausal); AI (post-menopausal only, more effective); GnRH agonist (pre-menopausal). NOT concurrent with chemo.
-
HER2 therapy: Trastuzumab-based therapy for HER2+ disease, usually total 1 year with cardiac monitoring; add pertuzumab for selected higher-risk disease; T-DM1 if residual invasive disease after neoadjuvant HER2 therapy.
-
Palliative: Bone mets → bisphosphonates/denosumab. Brain mets/cord compression/SVCO → RT ± steroids.
-
ALND complications: Long thoracic nerve (winged scapula), thoracodorsal nerve (weak shoulder adduction/IR), intercostobrachial nerve (paraesthesia medial arm), lymphoedema, Stewart-Treves syndrome.
High Yield Summary — Complications of Breast Cancer
Disease complications:
- Local: Skin ulceration, peau d'orange, dimpling, nipple retraction, chest wall invasion, brachial plexus invasion.
- Metastatic: Bone (pathological fractures, cord compression, hypercalcaemia), liver (hepatomegaly, jaundice), lung (effusion, dyspnoea), brain (raised ICP, focal neurology).
- SREs = pathological fractures + cord compression + hypercalcaemia.
Surgical complications: 4. Mastectomy: Seroma (most common specific), skin flap necrosis, post-mastectomy pain, phantom breast, arm morbidity. 5. ALND — 4 nerves: Long thoracic (winged scapula), thoracodorsal (weak adduction/IR), medial pectoral (pec major wasting), intercostobrachial (medial arm paraesthesia). Plus lymphoedema and Stewart-Treves syndrome (lymphangiosarcoma). 6. Implant: Capsular contracture, rupture (often silent), BIA-ALCL (ALK−, CD30+; capsulectomy curative if localised).
Therapy complications: 7. RT: Skin fibrosis, rib fracture, cardiotoxicity (left-sided), pulmonary fibrosis, secondary malignancy. 8. Anthracyclines: Dose-dependent irreversible cardiotoxicity. Trastuzumab: Reversible cardiotoxicity (not concurrent with anthracyclines). 9. Tamoxifen: Endometrial cancer, VTE (ER agonist effect in uterus/liver). AIs: Osteoporosis/fractures (no endometrial cancer risk). 10. Bisphosphonates/Denosumab: ONJ, hypocalcaemia (denosumab).
Benign Breast Disease
Benign breast disease encompasses a spectrum of non-cancerous breast conditions—including fibrocystic changes, fibroadenomas, and intraductal papillomas—that may present with pain, lumps, or nipple discharge and vary in their associated risk of subsequent malignancy.
Nipple Discharge Or Inversion
Nipple discharge or inversion refers to the spontaneous release of fluid from the nipple or retraction of the nipple inward, which may indicate benign conditions such as duct ectasia or intraductal papilloma, or may signal underlying malignancy such as breast carcinoma.